
Abstract
The aim of the present study was to explore the association between family functioning, coping strategies, peer influences and alcohol use among Italian adolescents. Nine hundred and sixty-three Italian adolescents, aged from 14 to 17 years, completed self-report measures assessing alcohol use, family functioning, and coping strategies. According to previous research, adolescents were categorized into non-drinkers, social, binge and heavy drinkers. Results showed that adolescents belonging to groups characterized by alcohol misuse differ in terms of coping strategies, family functioning dimensions, and typology of friends. In particular, heavy drinkers appeared to have more friends who drink alcohol on a regular basis and they were younger when started to drink on a regular basis than other drinking groups. Moreover, discriminant function analysis shows that avoidant coping strategies, early age of drinking, great number of friends who regularly drink alcohol and family dysfunctions are significant in the differentiation of drinking groups, separating heavy drinkers from others categories of drinkers
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Excessive alcohol consumption among adolescents is nowadays a great problem that contributes to a variety of negative outcomes, such as hospital admissions, antisocial behaviors, risky sexual behaviors, growing numbers of accidental injuries, and a substantial portion of crime-related deaths (Kendler et al. 2011; Reyes et al. 2011). Recent studies have showed that alcohol use among adolescents is fairly common, even though underage drinking is illegal and despite widespread efforts to deter adolescents from drinking (Catanzaro and Laurent 2004). According to the European School Survey Project on Alcohol and Other Drugs (ESPAD 2011), the frequency and amount of alcoholic beverages consumed by young people in Europe varies greatly by country and culture. The ESPAD survey found that in two-thirds of European countries the vast majority of students (almost 90 %) aged 15 to 16 years have consumed alcohol at least once. Moreover, in half of the participating countries, 46 % of the students had consumed at least one glass of alcohol at the age of 13 or younger, and 12 % had been drunk at that age. The ESPAD also reported that consumption of alcohol among Italian adolescents during the 12 months period prior to the completion of the study was equal to the average consumption in all ESPAD countries (79 %). The report also cited statistics on the consumption of alcohol during the last 30 days, underling that in Italy the average (63 %) was in line with that of other European countries (60 %).
1.1 Classification of Drinking Patterns and Risk Factors
Researchers have described four drinking categories, mutually exclusive, among adolescents: non-drinkers, social drinkers, binge drinkers, and heavy drinkers (Baiocco et al. 2010; Laghi et al. 2012; Morawska and Oei 2005). Non-drinker may be defined as someone who drinks alcohol less than twice per year or does not habitually consume alcohol and social drinker as a moderate consumer of alcohol (three/four times a year to three/four times per month) who uses the substance for convivial purposes and is characterized by a later alcohol approach. Moreover, a binge drinker is typically defined as someone who drinks five or more alcoholic drinks on one occasion (Miller et al. 2007). Finally, a heavy drinker is someone who drinks five (four for women) or more drinks on a single occasion five or more times within a month. Little research has been conducted into psychosocial variables underlining excessive use of alcohol (Laghi et al. 2012; Laghi et al. 2013). Thus, state-specific estimates of binge drinking are essential in planning and implementing strategies to prevent this particular form of alcohol misuse. Nevertheless, it is necessary to identify protective and risk factors involved in the drinking phenomenon. Brook and collaborators (2001) described a developmental model that identified parental relationship, individual personality and behavioral characteristics, and peer relationships as critical factors in predicting adolescent substance use. Reviews of the risk factors for adolescent alcohol use provide support for the model, suggesting that the highest risks could be summarized into these categories (Ennett et al. 2008).
1.2 Personal Characteristics
Studies of psychological functioning have emphasized a variety of variables that can be related to alcohol misuse. In particular, there has long been interest on the part of the researchers in understanding the role of the coping strategies in predicting drinking behavior (e.g. Catanzaro and Laurent 2004). Coping was defined as cognitive and behavioral efforts to manage psychological or physiological stress (Lazarus 1993) or as a cognitive, emotional and behavioral response to stress (Beutler et al. 2003); recently, research also suggested that coping strategies become more important and effective during adolescence than in childhood (Cocoradă and Mihalaşcu 2012). Facing the pressure of major changes in life and a variety of problem situations, adolescents use multiple strategies to adapt (Schimmenti and Caretti 2010; Strong et al. 2008), and during this process, poor coping skills may precede development behavioral symptoms (Schimmenti et al. 2012). Research has shown specific forms of coping strategies to be related to drinking (Catanzaro and Laurent 2004; Hasking and Oei 2004). In particular, they have found a significant correlation between ineffective coping skills and alcohol use among adolescents. Hasking and colleagues (2011) suggested that use of avoidant coping is predictive of risky drinking behavior. Hamdan-Mansour and colleagues (2007) found that avoidant coping behaviors, perceived social support from family, and a family history of alcohol abuse are predictive of alcohol abuse among rural adolescents. Their results confirm previous findings; for example, Steiner and colleagues (2002) found that health risk behaviors and health problems are negatively correlated with adolescents’ positive coping strategies and positively correlated with avoidant coping strategies.
1.3 Family and Peers Relationships
Family relationships and parents’ behaviors are central indicators of adolescent activities (Cacioppo et al. 2013; Pace et al. 2012). In accordance with this evidence, Olson and colleagues (1979) developed the circumplex model to investigate family functioning. The main hypothesis of the circumplex model (Olson et al. 1979) is that well-functioning families are considered balanced, falling mid-range in terms of cohesion and flexibility. In this model, family cohesion is defined as the emotional bond that family members have toward one another. Family flexibility refers to the quality and expression of the family’s leadership, organization, roles, and relationship rules. Several researchers found that adolescents who have good relationships with their parents have lower levels of alcohol use (Amato and Gilbreth 1999; McArdle 2008). For example, Di Grande and collaborators (2000) suggested that adolescents who perceive their families to have high cohesion and adaptability levels were more likely than adolescents from balanced and mid-range families to use alcohol (Smart et al. 1990). In Italy, the few studies that have explored the relationship between alcohol use and family functioning have provided evidence of a weak relationship between an adolescent’s family context and his or her alcohol use (e.g., Gerbino et al. 2005; Vieno et al. 2011), but the findings are not completely coherent. Indeed, Laghi and colleagues (2012) showed that heavy drinkers, unlike social and binge drinkers, live in families characterized by problematic functioning, with weak emotional bonds and loosely-defined relationship rules.
Finally, one of the most consistent findings in adolescent alcohol use research in the last 30 years has been the strong association between substance-using peers and individual substance use (for a review, see Kuntsche et al. 2004). Peers can influence individuals directly (e.g., by offering drinks, buying alcoholic beverages for friends, or pressuring others to drink) and indirectly through modeling and perceived norms. In this sense, theoretical models of social behavior emphasize the importance of peer behavior as a modeling (Bandura 1977) or normative (Fishbein and Ajzen 1975) influence. Griffin and collaborators (2000) demonstrated that having drinking peers or perceiving that close friends drink affects individual drinking. Moreover, in a longitudinal study, Werner and collaborators (1995) showed that friends’ drinking behavior was a significant predictor of alcohol use. In addition, previous research discovered that the estimated percentage of friends who drink was a better predictor of adolescent drinking (Wills et al. 2001). Most of the extant research addressing peer influence on alcohol use has been conducted on college students in the United States (for a review, see Borsari and Carey 2006) but the results of such studies cannot be generalized to other countries. For instance, in a comparison of U.S. and Scottish college students, Delk and Meilman (1996) showed differences in the students’ drinking culture. For this reason, further investigation is also needed to better understand Italian adolescent drinking patterns.
Starting from previous findings on the role of family functioning, personality characteristics, and peer influences in adolescents drinking patterns, the purpose of this study is to evaluate the relevance of drinking patterns among Italian adolescents and then determine a drinking profile to help discern the four drinking categories among Italian adolescents (non-drinkers, social drinkers, binge drinkers, and heavy drinkers). The broad prediction is that a combination of family functioning, coping strategies, and peer influences will be necessary to discriminate the drinking categories. In particular, we hypothesized that the following:
-
H1: Adolescents who perceive their families as unbalanced are more likely to misuse alcohol than adolescents from balanced families;
-
H2: Adolescents who employ maladaptive coping strategies are more likely to misuse alcohol than adolescents who use adaptive coping strategies;
-
H3: Adolescents who have a higher percentage of friends who drink are more likely to misuse alcohol than adolescents with a lower percentage of friends who drink.
This study extended the current research by examining the associations among family functioning, coping strategies, peer influences, and patterns of alcohol consumption exhibited by early Italian adolescents.
2 Methods
2.1 Participants and Procedure
Participants in the study were 963 adolescents (595 boys, 368 girls) for ages 14 to 17 (M = 14.70, SD = .81) attending public high schools located in five cities of Italy. We selected the schools as being representative of the socioeconomic structure of the Italian middle-class population in general, based on local census data. The homogeneity of socioeconomic status was controlled by means of the Hollingshead’s Index (1975). The majority (91 %) of the participants’ parents was skilled workers and had a high school (44 %) or college (47 %) degree. Participants were recruited using a ‘passive’ consent procedure, i.e. informing students’ parents in advance about the nature of the study and providing the opportunity for the parents to call our research office if they did not want their child participating in the study. There were no parents that objected to the involvement of their young in the study, and all the adolescents gave their consent to participate to the research. Participants completed consecutively self-report measures on family functioning, coping strategies, and alcohol use/severity in their classrooms. We obtained the assent from all the adolescents involved in the study. From a total sample of 985 respondents, the majority provided useable data; only twenty-two questionnaires were rejected due to many missing answers. Data were collected between January 2012 and June 2012. Research procedures described in this article were performed in compliance with the American Psychological Association and Italian Psychological Association ethical guidelines for research.
2.2 Measures
Demographics and Alcohol Use/Severity
An Identifying Information Form was used to collect demographic information. The questionnaire included questions about age and gender. Alcohol use was assessed with a questionnaire (Baiocco et al. 2010) that measures drinking quantity and frequency using different questions: frequency of alcohol consumption; average number of drinks consumed per occasion in the last month; age when alcohol was first tried outside the family. Moreover, the questionnaire yielded information about the amount of friends who drink regularly. According to previous research (Baiocco et al. 2010; Laghi et al. 2012; Morawska and Oei 2005), the specific question – ‘Usually, how often do you drink alcoholic beverages (e.g. wine, beer, champagne)?’ - allows classifying the ‘not drinkers’ (drinking alcohol less than twice per year) and ‘social drinkers’ (drinking alcohol ranging from three/four times a year to three/four times per month). Furthermore, two specific questions – ‘Considering all types of alcoholic beverage, did you have 5 or more drinks (4 if you are female) on one single occasion during the past month?’ and ‘How many times in the last month?’ - allow classifying the ‘binge drinkers’ (one to eight binge drinking episodes in a month) and the ‘heavy drinkers’ (more than 8 binge drinking episodes in a month).
Family Adaptability and Cohesion Evaluation Scales
The Family Adaptability and Cohesion Evaluation Scales (FACES-IV; Olson 2011; Italian version, Baiocco et al. 2012) measures the family functioning using six scales: two balanced scales, Cohesion (sample item: ‘Family members are supportive of each other during difficult times’) and Flexibility (sample item: ‘My family is able to adjust to change when necessary’), assessing central-moderate areas and four unbalanced scales, Enmeshed (sample item: ‘Family members feel guilty if they want to spend time away from the family’), Disengaged (sample item: ‘Family members seem to avoid contact with each other when at home’), Chaotic (sample item: ‘Our family feels hectic and disorganized’), and Rigid (sample item: ‘There are clear consequences when a family member does something wrong’), assessing the upper and the lower extremes of Cohesion and Flexibility respectively (Olson and Gorall 2006). It is hypothesized that the central or balanced levels make for optimal family functioning, while the extremes or unbalanced levels are generally seen as problematic for relationship over the longer term. In addition, it is possible evaluate the Circumplex Total Ratio that provides a summary of a family’s balanced and unbalanced characteristics in a single score (Olson 2011) and is calculated by dividing the average of the two balanced scales of FACES IV (Cohesion and Flexibility) by the average of the four unbalanced scales (Disengaged, Enmeshed, Chaotic and Rigid). The lower the ratio score, the more unbalanced the system. Conversely, the higher the ratio score, the more balanced the system. There are seven items in each scale, making a total of 42 items. The participants are asked to rate how much they agree with the statement on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The dimensions formulated to define the construct of the family functioning were confirmed after factor analysis in previous studies and they accounted for 38.2 % of the post-rotational variance (Baiocco et al. 2012; Olson 2011). In addition, the six scales in FACES IV were also found to be reliable and valid (Baiocco et al. 2012). The Cronbach’s alpha coefficients ranged from .63 to .73 in previous studies (Baiocco et al. 2012) and from .71 to .78 in the current sample.
Coping Strategy Indicator
The Coping Strategy Indicator (CSI), developed by Amirkhan (1990), is a self-report measure of coping strategies and it consists of 33 items. Responses on each of the CSI’s 33-items are indicated by means of a three point scale: a lot (3) a little (2), or not at all (1). The checklist consists of three subscales: Social Support (SS; sample item: ‘Described your feelings to a friend’), Problem Solving (PS; sample item: ‘Rearranged things so your problem could be solved’), Avoidance (A; sample item: ‘Tried to distract yourself from the problem’), each contains 11 items and subscale scores are calculated by summing responses to appropriate items (range 0–33), higher scores indicate greater use of the strategy. Cronbach’s alpha coefficients indicate adequate internal consistency for each of the subscales ranging from .77 to .98 in previous studies (Amirkhan 1990; Clark et al. 1995) and ranging from .72 to .86 in the current study. In the original version of the scale respondents are asked to identify a stressful event occurring within the last 6 months and to consider the manner in which they had coped with it. In the current study, the respondents were required to think of a problem encountered in their school life or in the relationship with peer and adults (excluded family members) in the last months and reflect on their coping strategies.
2.3 Data Analysis
Descriptive statistics were computed for all the observed variables. Chi-square analyses were conducted to assess group differences in sociodemographic characteristics. Furthermore, univariate tests (ANOVA) and post hoc analyses with Tukey test (p < .01) were conducted to detect group differences about the age when they first tried alcohol and the number of friends who regularly drink alcohol. Group differences about family functioning and personal characterisitcs were analyzed using MANCOVA model with Wilks’ λ criterion. We considered ‘alcohol use’ group (non-drinkers versus social versus binge versus heavy) as the fixed factor while the family and coping strategies dimensions as the dependent variables; effects of gender and age were adjusted as covariates. Univariate tests (ANCOVA) and post hoc analyses with Tukey test (p < .01) following MANCOVA were carried out to detect group differences. A discriminant function analysis was conducted to determine which variables best discriminate between four groups (non-drinkers, social, binge and heavy drinkers).
3 Results
3.1 Individual Correlates of Drinking Patterns
The sample was composed of 346 non-drinkers (36 %), 387 social drinkers (40 %), 152 binge drinkers (16 %) and 78 heavy drinkers (8 %). The frequency distribution of the drinking patterns in the current study is in line with other studies (Miller et al. 2007; Tucker et al. 2003). Drinking groups differed according to sex [χ 2(3) = 12.57, p < .01]: males were more likely to be classified as social drinkers (41.5 % of males versus 38 % of females), binge drinkers (18.2 % of males versus 12 % of females) and heavy drinkers (8.2 % of males versus 7.9 % of females), while females were more likely to be classified as non-drinkers (42.1 % of females versus 32.1 % of males). Moreover, drinking group differed as the number of friends who regularly drink alcohol [F(3,822) = 36.77, p < .0001]. Post hoc analyses revealed that heavy drinkers (M = 2.63, SD = .14) appeared to have more friends who drink alcohol on a regular basis than binge drinkers (M = 1.98, SD = .10) and binge drinkers appeared to have more friends who drink alcohol on a regular basis than social drinkers (M = 1.51, SD = .06); non-drinkers reported the lowest number of friends who drink alcohol (M = 1.12, SD = .07).
Social, binge and heavy drinkers differed as to the age when they first tried alcohol [F(2,613) = 9.34, p < .0001]. Post hoc analyses revealed that heavy drinkers were younger than binge drinkers and social drinkers (M = 13.00; SD = .16 versus M = 13.86; SD = .12 versus M = 13.93; SD = .08, respectively).
3.2 Primary Analyses: Descriptive Statistics and Differences Between Groups
Descriptive analyses for all independent and dependent variables are presented in Table 1. To examine differences in family functioning dimensions and coping strategies use between drinking group, a MANCOVA model with Wilks’ λ criterion was conducted. The MANCOVA revealed the main effects for the groups [Wilks’ Lambda = .94, F = 2.28, p < .0001]. Age did not show significant covariations with groups [Wilks’ Lambda = .98, F = 1.58, p = .86], while gender showed significant covariations with groups [Wilks’ Lambda = .91, F = 9.67, p < .0001]. The groups differed as regard to the gender on coping strategies variables: in particular, Problem solving coping [F(1,961) = 5.35; p < .05] and Seeking social support coping [F(1,961) = 85.77; p < .0001]. Consistent with other studies, females reported higher scores than males in both scales (M = 23.90; SD = 4.39 versus M = 23.22; SD = 4.43 and M = 23.33; SD = 5.07 versus M = 20.24; SD = 5.17, respectively). Concerning family functioning, results from the univariate tests (ANCOVA) revealed that groups differed on the Circumplex Total Ratio [F(3,959) = 9.63, p < .0001], Cohesion [F(3,959) = 7.04, p < .0001], Flexibility [F(3,959) = 5.00, p < .01], Disengaged [F(3,959) = 5.36, p < .01], and Enmeshed [F(3,959) = 4.07, p < .01]. In particular, post hoc analyses revealed that non-drinkers showed higher mean scores than binge and heavy drinkers in the scales of Cohesion and Flexibility. Social drinkers showed lower mean scores than non-drinkers in the scale of Enmeshed. Furthermore, they showed higher mean scores than heavy drinkers in the scale of Cohesion. Binge drinkers and heavy drinkers showed higher mean scores than non-drinkers and social drinkers in the scale of Disengaged. Finally, binge and heavy drinkers showed lower mean scores than social and non-drinkers in the Circumplex Total Ratio. No differences between groups were found in other scales. Concerning coping strategies use, results from the univariate tests (ANCOVA) and post-hoc analyses revealed that the groups differed only on Avoidant coping [F(3,959) = 5.08, p < .01]; in particular, heavy drinkers showed higher mean scores than social and non-drinkers.
3.3 Discriminant Function Analysis
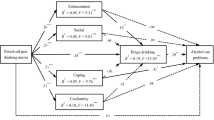
A discriminant function analysis was conducted to determine the variables that enabled us to differentiate between the four groups. Two significant functions emerged [χ 2 (18) = 77.46, p < .000; χ 2 (10) = 34.81, p < .000]. The first function accounted for most of the variance (86.8 %). Structure matrix (Table 2) shows that function 1 was principally explained by two social variables: the number of friends who regularly drink alcohol and the age when the subjects first tried alcohol. This function was termed social influence. Function 2 was explained by and the Circumplex Total Ratio of FACES IV and avoidant coping strategies. This function can be defined as parents/personality influence. An evaluation of the group centroids showed that function 1 best separates heavy drinkers from non-drinkers whereas function 2 adds to differentiate binge and heavy drinkers from non-drinkers. The results of discriminant classification show 66 % of the subjects correctly classified (64.3 % of non-drinkers; 65.7 % of social drinkers, 67 % of binge drinkers and 68.2 % of heavy drinkers).
4 Discussion and Conclusion
The principal aims of the present study were to evaluate the relevance of drinking patterns among Italian adolescents and related individuate dimensions, such as coping strategies, peer influences, and family functioning, in discriminating between drinking patterns. Data showed that 36 % of adolescents were classified as non-drinkers, 40 % as social drinkers, 16 % as binge drinkers, and 8 % as heavy drinkers. The percentages of binge and heavy drinkers in the current study are in line with other studies using a similar age sample (Miller et al. 2007; Tucker et al. 2003) but lower than in other research conducted in Italy with late adolescents (Laghi et al. 2012). Moreover, males were more likely to be classified as binge and heavy drinkers than females. The data, which is consistent with other studies (Gallimberti et al. 2011; ESPAD 2011), confirmed that binge and heavy drinking is indeed widespread among adolescents, especially among males.
The univariate and multivariate analysis showed that adolescents belonging to groups characterized by alcohol misuse differ in terms of typology of friends, family functioning dimensions, and coping strategies. Results indicate that heavy drinkers appeared to have more friends who drink alcohol on a regular basis than binge drinkers, and binge drinkers appeared to have more friends who drink alcohol on a regular basis than social drinkers; non-drinkers reported the lowest number of friends who drink alcohol. Furthermore, heavy drinkers were younger than binge and social drinkers when they started to drink on a regular basis. Data from the present study highlight that adolescents affiliating with friends who drink were more likely to drink than those affiliating with non-drinkers and are in agreement with other studies that found percentage of drinking friends to be good predictor of adolescent drinking (Baiocco et al. 2010). According to social learning theory, modeling and adherence to proscriptive norms are key mechanisms of influence (Borsari and Carey 2001). According this theoretical framework, peers will encourage a healthy use of alcohol through social reinforcement, modeling, and cognitive processes. Conversely, among adolescents, friends will support heavy alcohol use if this behavior is viewed as favorable rather than unfavorable among a peers group (Winfree et al. 1994).
Results showed that non-drinkers and social drinkers live in balanced families in which relational boundaries are better defined than those of binge and heavy drinkers. Moreover non-drinkers and their families are more able to modify their own relationship rules and structures in response to life challenges and everyday problems than binge and heavy drinkers. Nevertheless, non-drinkers and their families appear more dependent on each other and reactive to one another than social drinkers and their families. On the other hand, binge and heavy drinkers, unlike non-drinkers and social drinkers, live in families characterized by a problematic functioning, in which there is little involvement among family members and a great deal of personal separateness and independence. In these families, the members are unable to turn to one other for support and problem solving.
Previous studies provided evidence that negative family characteristics are linked to alcohol misuse. Recent findings have showed that heavy drinkers revealed more problematic family functioning than social drinkers (Laghi et al. 2012); in the same way, the data from the present study support previous assertions that adolescents’ alcohol use may be partially due to dysfunctional family relationships, including more conflicts and less cohesion (Lloyd-Richardson et al. 2002).
The results also showed that heavy drinkers, unlike non-drinkers and social drinkers, use avoidance as a strategy for coping with their problems. The literature supports the positive association between avoidant coping strategies and alcohol use among adolescents (Catanzaro and Laurent 2004; Hasking et al. 2011). A possible explanation for this relationship is that the adolescence is a period of rapid cognitive, social, emotional, and physical change (Forman 1993), which brings with it varying amounts of stress (Pace and Zappulla 2009). Stressful events experienced in adolescence may contribute to emotional or behavioral problems, such as alcohol use, especially during a period in which the autonomy process is characterized by disengagement from emotional bonds toward parents owing to feelings of distrust and the perception of alienation from them (Pace and Zappulla 2011). In families in which promotion of adolescents’ autonomy is not associated to adequate level of family functioning, avoidant coping strategies may represent maladaptive answers to developmental tasks (Seiffge-Krenke and Klessinger 2000). Moreover, in this period, individual susceptibility to negative peer pressure, linked to a lack of family cohesion and functioning, may exacerbate the level of risk that avoidant coping strategies represent toward alcohol consumption. In this sense, the results of the discriminant function analysis show that coping strategies, variables concerning alcohol use (age when regular drinking began and number of friends who regularly drink alcohol), and family functioning are significant in discriminating between drinking groups. The model suggests that social influence (number of friends who regularly drink alcohol and the age when the subjects first tried alcohol) best separates heavy drinkers from others categories of drinkers, while the second function - parental/personality influence (circumplex model of family functioning and avoidant coping strategies) - helps differentiate binge and heavy drinkers from non-drinkers.
In summary, our results highlight that peer influences and the age the adolescent first tried alcohol were strong predictors of alcohol consumption. On the other hand, family functioning plays a significant protective role for adolescents, while, conversely, low levels of involvement and affective support and the presence of inconsistent rules represent further risk factors, which may exacerbate the tendency toward alcohol misuse. Results may prove valuable to prevention specialists working with adolescents. An ecological framework for a public health prevention effort should consider health-related behaviors to be determined by several factors, such as family functioning, peer influences, and coping strategies.
4.1 Strengths and Limitations
This study contributes to the analyses of the complex relationship among perceived characteristics of an adolescent’s family relationships, coping strategies, peer influences, and alcohol use. However, some limitations have to be underlined, all of which suggest rewarding avenues for further research. First, the study includes only Italian participants. It would be interesting to see if our results can be reproduced in other countries. Second, all the data were collected using self-report measures, and the accuracy of individual reporters cannot be assured. Third, we collected all the data at a single point in time to focus specifically on the issues of the co-occurrence. It would be more correct to underscore the relationships among variables rather than their predictive roles. Future longitudinal research could investigate the paths that the variables explored in the present study would trace during development. Finally, further research should take into consideration the phenomenon of alcoholism among adolescents who do not attend school and who do not live in big cities.
Despite these limitations, our findings suggest that the interventions for adolescents who misuse alcohol should focus on increasing adaptive coping strategies and improving family relationships by helping parents improve communication skills and display acceptance or warmth as protective factors that help a young person reject alcohol. Finally, this study highlights the importance of a comprehensive approach to the prevention of alcohol use among adolescents.
References
Amato, P. R., & Gilbreth, J. G. (1999). Nonresident fathers and children’s well-being: a meta-analysis. Journal of Marriage and the Family, 61, 557–573.
Amirkhan, J. H. (1990). A factor analitically derived measure of coping: the strategy coping indicator. Journal of Personality and Social Psychology, 59, 1066–1074.
Baiocco, R., D’Alessio, M., & Laghi, F. (2010). Binge drinking among gay and lesbian youths: the role of internalized sexual stigma, self-disclosure and individuals’ sense of connectedness to the gay community. Addictive Behaviors, 35, 896–899.
Baiocco, R., et al. (2012). Factorial and construct validity of FACES IV among italian adolescents. Journal of Child and Family Studies. doi:10.1007/s10826-012-9658-1.
Bandura, A. (1977). Social learning theory. Englewood Cliffs: Prentice-Hall.
Beutler, L. E., Moos, R. H., & Lane, G. (2003). Coping, treatment planning, and treatment outcome: discussion. Journal of Clinical Psychology, 59, 1151–1167.
Borsari, B., & Carey, K. B. (2001). Peer influences in college drinking: a review of the research. Journal of Substance Abuse, 13, 391–424.
Borsari, B., & Carey, K. B. (2006). How the quality of peer relationships influences college alcohol use. Drug and Alcohol Review, 25(4), 361–370.
Brook, J. S., Brook, D. W., & Richter, L. (2001). Risk factors for adolescent marijuana use across cultures and across time. Journal of Genetic Psychology, 162, 357–374.
Cacioppo, M., Pace, U., & Zappulla, C. (2013). Parental psychological control, quality of family context and life satisfaction among Italian adolescents. Child Indicators Research, 6, 179–191.
Catanzaro, S. J., & Laurent, J. (2004). Perceived family support, negative mood regulation expectancies, coping, and adolescent alcohol use: evidence of mediation and moderation effect. Addictive Behaviors, 29, 1779–1797.
Clark, K. K., et al. (1995). Validation evidence for three measures of coping. Journal of Personality Assessment, 65(3), 434–455.
Cocoradă, E., & Mihalaşcu, V. (2012). Adolescent coping strategies in secondary school. Procedia - Social and Behavioral Sciences, 33, 188–192.
Delk, E. W., & Meilman, P. W. (1996). Alcohol use among college students in Scotland compared with norms from the United States. Journal of American College Health, 44(6), 274–281.
Di Grande, L., et al. (2000). Alcohol use and correlates of binge drinking among university students on the Island of Sardinia, Italy. Substance Use & Misuse, 35(10), 1471–1483.
Ennett, S. T., et al. (2008). The social ecology of adolescent alcohol misuse. Child Development, 79, 1777–1791.
ESPAD, 2011. The 2011 ESPAD Report: Substance Use Among Students in 36 European Countries [online]. Available from: http://www.espad.org/Uploads/ESPAD_reports/2011/The_2011_ESPAD_Report_FULL_2012_10_29.pdf.
Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. Reading: Addison-Wesley.
Forman, S. G. (1993). Coping skills intervention during childhood and adolescence. San Francisco: Jossey-Bass.
Gallimberti, L., et al. (2011). Underage drinking on Saturday nights, sociodemographic and environmental risk factors: A cross-sectional study. Substance Abuse Treatment, Prevention, and Policy, 6, 15–23.
Gerbino, M., et al., 2005. Fattori di protezione e di rischio nell’uso di alcol e droga in adolescenza. Psicologia clinica dello sviluppo, a. IX, 3.
Griffin, K. W., et al. (2000). Parenting practices as predictors of substance use, delinquency, and aggression among urban minority youth: moderating effects of family structure and gender. Psychology of Addictive Behaviors, 14(2), 174–184.
Hamdan-Mansour, A. M., Puskar, K., & Sereika, S. M. (2007). Perceived social support, coping strategies and alcohol use among rural adolescents/USA sample. International Journal of Mental Health and Addiction, 5, 53–64.
Hasking, P. A., & Oei, T. P. S. (2004). The complexity of drinking: Interactions between the cognitive and behavioural determinants of alcohol consumption. Addiction Research and Theory, 12, 469–488.
Hasking, P., Lyvers, M., & Carlopio, C. (2011). The relationship between coping strategies, alcohol expectancies, drinking motives and drinking behavior. Addictive Behaviors, 36, 479–487.
Hollingshead, A. (1975). The four-factor index of social status (Unpublished manuscript). New Haven: Yale University.
Kendler, K., Gardner, C., & Dick, D. (2011). Predicting alcohol consumption in adolescence from alcohol-specific and general externalizing genetic risk factors, key environmental exposures and their interaction. Psychological Medicine, 41(7), 1507–1516.
Kuntsche, E., Rehm, J., & Gmel, G. (2004). Characteristics of binge drinkers in Europe. Social Science & Medicine, 59, 113–127.
Laghi, F., et al. (2012). Family functioning and binge drinking among Italian adolescents. Journal of Health Psychology, 17(8), 1132–1141.
Laghi, F., et al. (2013). The role of parenting styles and alcohol expectancies in teen binge drinking: a preliminary investigation among Italian adolescents and their parents. Drugs Education Prevention and Policy. doi:10.3109/09687637.2012.713409.
Lazarus, R. S. (1993). Coping theory and research: past, present, and future. Psychosomatic Medicine, 55, 234–247.
Lloyd-Richardson, E. E., et al. (2002). Differentiating stages of smoking intensity among adolescents: stage-specific psychological and social influences. Journal of Consulting and Clinical Psychology, 70(4), 998–1009.
McArdle, P. (2008). Alcohol abuse in adolescents. Archives of Disease in Childhood, 93, 524–527.
Miller, J. W., et al. (2007). Binge drinking and associated health risk behaviors among high school students. Pediatrics, 119(1), 76–85.
Morawska, A., & Oei, T. P. S. (2005). Binge drinking in university students: a test of the cognitive model. Addictive Behaviors, 30, 203–218.
Olson, D. H. (2011). FACES IV and the circumplex model: validation study. Journal of Marital and Family Therapy, 3(1), 64–80.
Olson, D. H., & Gorall, D. M. (2006). Faces IV and the circumplex model. Minneapolis: Life Innovations.
Olson, D. H., Sprenkle, D. H., & Russell, C. (1979). Circumplex model of marital and family systems: i. cohesion and adaptability dimensions, family types, and clinical applications. Family Process, 18, 3–28.
Pace, U., & Zappulla, C. (2009). Identity processes and quality of emotional autonomy: the contribution of two developmental tasks on middle-adolescents’ subjective well-being. Identity An International Journal of Theory and Research, 9, 323–340.
Pace, U., & Zappulla, C. (2011). Problem behaviors in adolescence: the opposite role played by insecure attachment and commitment strength. Journal of Child and Family Studies, 20, 854–862.
Pace, U., Cacioppo, M., & Schimmenti, A. (2012). The moderating role of father’s care on the onset of binge eating symptoms among female late adolescents with insecure attachment. Child Psychiatry and Human Development, 43, 282–292.
Reyes, H. L. M., et al. (2011). The role of heavy alcohol use in the developmental process of desistence in dating aggression during adolescence. Journal of Abnormal Child Psychopathology, 39, 239–250.
Schimmenti, A., & Caretti, V. (2010). Psychic retreats or psychic pits? unbearable states of mind and technological addiction. Psychoanalytic Psychology, 27(2), 115–132.
Schimmenti, A., et al. (2012). Attachment disorganization and dissociation in virtual worlds: a study on problematic Internet use among players of online role-playing games. Clinical Neuropsychiatry, 9(2), 195–202.
Seiffge-Krenke, I., & Klessinger, N. (2000). Long-term effects of avoidant coping on adolescents’ depressive symptoms. Journal of Youth and Adolescence, 29(6), 617–630.
Smart, L. S., Chibucos, T. R., & Didier, L. A. (1990). Adolescent substance use and perceived family functioning. Journal of Family Issues, 11, 208–227.
Steiner, H., et al. (2002). Coping styles as correlates of health in high school students. Journal of Adolescent Health, 30, 326–335.
Strong, B., DeVault, C., & Cohen, T. F. (2008). The marriage and family experience: Intimate relationships in a changing society (10th ed.). Belmont: Thomson Learning, Inc.
Tucker, J. S., Orlando, M., & Ellickson, P. L. (2003). Patterns and correlates of binge drinking trajectories from early adolescence to young adulthood. Health Psychology, 22, 79–87.
Vieno, A., et al. (2011). Fattori di rischio dell’abuso di alcolici in adolescenza e il loro effetto sommativo. Psicologia Clinica Dello Sviluppo, XV(2), 407–425.
Werner, M. J., Walker, L. S., & Greene, J. W. (1995). Relation of alcohol expectancies to changes in problem drinking among college students. Archives of Pediatrics & Adolescent Medicine, 149, 733–739.
Wills, T. A., et al. (2001). Temperament related to early-onset substance use: test of a developmental model. Prevention Science, 2(3), 145–163.
Winfree, L. T., Vigil-Backstrom, T., & Mays, G. L. (1994). Social learning theory, self-reported delinquency, and youth gangs: a new twist on a general theory of crime and delinquency. Youth and Society, 26(2), 147–177.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guzzo, G., Lo Cascio, V. & Pace, U. The Role of Individual and Relational Characteristics on Alcohol Consumption among Italian Adolescents: A Discriminant Function Analysis. Child Ind Res 6, 605–618 (2013). https://doi.org/10.1007/s12187-013-9188-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12187-013-9188-4