
Abstract
Until recently, the genetic aberrations that are causally linked to the pathogenesis of myelodysplastic syndromes (MDS) and myeloproliferative neoplasms were largely unknown. Using novel technologies like high-resolution SNP-array analysis and next generation sequencing, various genes have now been identified that are recurrently mutated. Strikingly, several of the newly identified genes (ASXL1, DNMT3A, EZH2, IDH1 and IDH2, and TET2) are involved in the epigenetic regulation of gene expression. Aberrant epigenetic modifications have been described in many types of cancer, including myeloid malignancies. It has been proposed that repression of genes that are crucial for the cessation of the cell cycle and induction of differentiation might contribute to the malignant transformation of normal hematopoietic cells. Several therapies that aim to re-express silenced genes are currently being tested in MDS, like histone deacetylase inhibitors and hypomethylating agents. It will be interesting to assess whether patients carrying mutations in epigenetic regulators respond differently to these novel forms of epigenetic therapies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Myelodysplastic syndromes (MDS) represent a heterogeneous group of malignant hematopoietic disorders that predominantly affect the elderly [1–3]. In patients suffering from MDS, the myeloid cells in the bone marrow are characterized by uni- or multilineage dysplasia, which is often accompanied by hyperplasia and enhanced apoptosis. This ineffective hematopoiesis may result in one or more peripheral cytopenias. Furthermore, approximately 30% of patients develop acute myeloid leukemia (AML). Due to considerable differences in the number and severity of cytopenias and in the propensity of developing AML, the median overall survival of distinct patient groups may vary from 5 months to ≥9 years [4]. The diversity in the clinical presentation of MDS emphasizes the need for tailored treatment of patients. Current therapy options comprise supportive therapy (transfusions, antibiotics), growth factor therapy (erythropoietin, granulocytic-colony stimulating factor), chemotherapy (cytarabine with/without anthracycline), immunotherapy (lenalidomide, thalidomide, anti-thymocyte globulin, cyclosporin A), epigenetic therapy (azacitidine, decitabine) and stem cell transplantation (SCT) [2, 3]. To date, SCT is the sole treatment that may result in cure; however, due to high toxicity of the treatment and the advanced age of many MDS patients it can only be applied in a subset of cases. Assessing the appropriate treatment for each patient requires accurate diagnosis, classification and prognostication of the diverse syndromes. This is based on bone marrow morphology, blast count, peripheral blood cytopenias and the karyotype of the malignant clone. Various systems that take these parameters into account have been developed and can be used to stratify patients with different clinical behavior into distinct categories. Systems comprise the International Prognostic Scoring System (IPSS), the World Health Organisation (WHO) classification system, and the WHO classification-based prognostic scoring system (WPSS) [1–3]. Recurrent aberrant karyotypes, which are incorporated in these systems, cannot entirely account for the genetic defects that are at the basis of the pathogenesis of MDS, as they are detected only in approximately 50% of patients [4]. A more accurate prediction of clinical outcome may require the incorporation of small genetic defects that have been revealed by the application of high-resolution SNP-arrays, Sanger sequencing, and whole exome sequencing [5–7]. Affected genes encode signal transduction proteins (BRAF, CBL, GNAS, JAK2, KRAS, NRAS and PTPN11), transcription factors and cofactors (ETV6, NPM1, RUNX1 and TP53), cell cycle regulators (CDKN2A and PTEN), components of the RNA splicing machinery (PRPF40B, SF1, SF3A1, SF3B1, SRSF2, U2AF35, U2AF65 and ZRSR2), and epigenetic regulators (ASXL1, DNMT3A, EZH2, IDH1 and IDH2, and TET2). Epigenetic regulators influence gene expression by methylation of DNA and modification of the DNA-associated histone proteins (see Box 1) [8]. The discovery of mutations in these epigenetic regulators might be in line with observations describing both deregulated DNA methylation patterns in MDS, which correlated with overall survival, and clinical response to hypomethylating agents, which was associated with a decrease in DNA methylation [9–12]. It will be interesting to investigate whether clinical responses also correlate with the presence of mutations in epigenetic factors. We will summarize the current knowledge about the mutated epigenetic factors in this review.
The ASXL1 protein
The epigenetic regulator ASXL1 (Fig. 1a) displays a dual function in that it mediates both gene repression and gene activation, depending on the cellular context [13–15]. Gene regulation by ASXL1 in mammalian cells is exerted by interaction of ASXL1 with nuclear receptors, like RARα and PPARγ, upon ligand induction (Fig. 1a). Subsequent gene silencing involves complex formation with the epigenetic regulators HP1 and LSD1 [13, 14], whereas gene activation involves both the C-terminal PHD domain of ASXL1 and the interaction of ASXL1 with the histone methyltransferase SRC1 [15] (Fig. 1a). The human ASXL1 gene is located on chromosome 20q11.21. Although chromosome 20q may be affected by deletions (del(20q)) in MDS, ASXL1 does not reside in the commonly deleted region [4, 16]. However, truncating ASXL1 mutations, which are predominantly heterozygous and monoallelic, occur in 16% of patients with MDS and are closely associated with RAEB-1 (refractory anemia with excess blasts-1) and RAEB-2 (23 and 30% of patients, respectively); besides, ASXL1 mutations occurs in 22% of patients with secondary AML post-MDS [17–20]. In line with this distribution is the observation that the presence of ASXL1 mutations showed a correlation with progression of MDS to AML [20]. In addition, the presence of ASXL1 mutations correlated with poor overall survival in various patient cohorts, and multivariate analyses indicated that ASXL1 mutations represent an independent poor risk factor for overall survival [5, 20]. These results might be of importance for future prognostication, especially since most ASXL1 mutations were detected in lower-risk (low and intermediate-1 risk) patients [5]. It is tempting to speculate that patients harboring ASXL1 mutations might benefit from epigenetic therapy since disruption of this epigenetic factor might confer an aberrant epigenetic profile. However, to date, both the impact of ASXL1 mutations on the epigenetic profile and the contribution of these mutations to the pathogenesis of MDS remain unknown. Notably, the adverse effects of ASXL1 mutations on prognosis are opposite to the correlation of isolated del(20q) with good prognosis [3, 4], suggesting that del(20q) and mutations of ASXL1 represent different pathogenic events in MDS. This is consistent with the observation that ASXL1 mutations (n = 63) co-occurred with 28% of isolated del(20q) deletions in a cohort of 439 MDS patients [5]. Of importance is that all ASXL1 mutations described in this cohort were heterozygous, including the ones that co-occurred with del(20q). This observation confirms the previous observations [16] that the ASXL1 gene does not reside in the commonly deleted region on chromosome 20q. As ASXL1 mutations and del(20q) seem to represent different events, this might indicate that ASXL1 mutations result in dominant-negative functions or gain of functions rather than loss of function; however, haploinsufficiency cannot be excluded at present. Mutations of ASXL1 also occurred in the context of diverse isolated cytogenetic abnormalities (30% of chromosome 7/7q deletions, 17% of trisomy 8 and 9% of del(5q)), and co-occurrence was seen with 20% of TET2 mutations, 47% of IDH mutations and 50% of EZH2 mutations, suggesting that these epigenetic factors might display complementary functions in epigenetic regulation and in the pathogenesis of MDS. To examine possible effects of the ASXL1 mutations, we will highlight some features of the discovered mutations. Mutations of ASXL1 affect the longest isoform (Fig. 1a) and target the last two exons, encoding amino acids 361–1541 [17–20]. One of the most frequently occurring, but disputed, mutations observed in these cohorts was the p.G646WfsX12 frameshift mutation. At present, the status of this mutation is uncertain, since it was claimed to be a PCR-artifact [21]. However, large-scale analysis of 439 MDS samples by Bejar et al. [5] revealed just one p.G646WfsX12 mutation, while the total percentage of ASXL1 mutations in this study was similar to the percentage reported in previous studies [17–20] (14 vs. 16%); furthermore, Bejar and colleagues affirmed the somatic origin of this mutation. This indicates that the status of this variant remains controversial. Probably, repeated PCR and sequence analysis of paired somatic and germ line samples should be executed to determine the true nature of this variant. In addition to the germ line analysis of the p.G646WfsX12 mutation, the somatic origin of 2 out of 5 missense variants (R402Q and A1486T) was confirmed by Bejar and colleagues. Missense variants had also been detected in the initial cohorts [18, 20], but had not been included in the calculations as their somatic origin had not been verified; some of them were identified as single nucleotide polymorphisms (SNPs) in subsequent studies [5]. Nevertheless, even when all possible missense mutations are included, then still more than 90% of all ASXL1 mutations are truncating mutations, predicting an ASXL1 protein that lacks its PHD domain in all cases and the RARα-binding domain in most cases. Since it is not clear whether mutant ASXL1 is transcribed and translated into protein, it would be interesting to assess the presence of mutant ASXL1 protein in MDS cells. If the mutated ASXL1 gene is expressed, the function of the mutant proteins should be investigated. Future functional analysis of the truncated proteins could be extended to the examination of the confirmed missense mutation R402Q [5] as well as two in-frame deletion–insertion variants that compromise amino acids 639–660 [20] (Fig. 1a); examination of these mutant proteins would be of particular interest since these variants alter a small region within the SRC1-binding domain without affecting the overall reading frame. The frequent disruption of ASXL1 domains that are implicated in gene activation (the PHD domain, the RARα-binding domain and the SRC1-binding domain) indicates that only the repressive domains (the HP1- and LSD1-binding domains) remain intact. Although the RARα-binding domain plays a role in RARα-dependent repression, this domain is not required for the RARα-independent repressive capacity of ASXL1 displayed in in vitro assays [13]. Therefore, if expressed, the repressive domains might interfere with epigenetic regulation. In summary, ASXL1 mutations could represent different pathogenic events from del(20q) and may result in dominant-negative function or gain of function. The repressive domains of ASXL1 might be important for the mutant function.

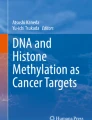
Epigenetic regulators that are mutated in MDS. Schematic pictures of proteins, including functional and interacting domains, are shown. a The ASXL1 protein; HP1 HP1-binding domain, LSD1 LSD1-binding domain, SRC1 SRC1-binding domain, RARα RARα-binding domain, PHD PHD domain, asterisk R402Q, black bar in-frame deletions. b The DNMT3A and DNMT3A3 proteins; PWWP PWWP domain, PHD PHD-zinc finger domain, MT methyltransferase domain, asterisk p.Q237X, p.L422fs, p.E599X. c The EZH2 protein; EED EED-binding domain, SUZ12 SUZ12-binding domain; CXXC cysteine-rich domain, SET SET domain. d The IDH1 and IDH2 domains; large (red) and small (pink) domains of the active region are indicated; asterisk IDH1-R132, IDH2-R140 and R172. e The TET2 protein; conserved domains are indicated with hatched bars
The DNMT3A protein
The DNMT3A protein (Fig. 1b) is a DNA methyltransferase that catalyzes de novo methylation of cytosines in genomic DNA (Box 1) [22, 23]. DNA methylation plays an important role in human development, self-renewal of stem cells, DNA repair and cellular differentiation: not only has it been linked to chromosomal integrity by both repression of transposable elements and stabilization of chromosomes, but it is also involved in gene repression and maintenance of active chromatin states, thereby controlling genomic imprinting, X chromosome inactivation and proper gene expression [22–26]. These processes are severely deregulated in tumor cells, which exhibit widespread chromosomal loss of DNA methylation and concurrent chromosomal aberrations as well as altered gene expression: tumor suppressors are suppressed whereas oncogenes are activated as a result of gene hypermethylation and gene hypomethylation, respectively [26, 27]. These abnormalities are also implicated in the pathogenesis of MDS and may be elicited, at least in part, by the DNMT3A mutations that have been detected in MDS [6, 28, 29]. Mutations of the DNMT3A gene, located on chromosome 2p23.3, were detected in 6% of MDS patients and exhibited equal distribution amongst the different MDS subtypes [6, 28, 29]. The patient cohorts that were screened for DNMT3A mutations were too small to perform multivariate analysis for clinical outcome. Nevertheless, the presence of DNMT3A mutations correlated with poor clinical outcome in univariate analysis: patients harboring DNMT3A mutations showed increased progression toward AML and inferior overall survival. It will be interesting to assess the effect of treatment with hypomethylating agents (azacitidine and decitabine) on clinical outcome in patients carrying DNMT3A mutations, since acquired mutations of this DNA methyltransferase are expected to affect DNA methylation patterns. At present, it remains elusive whether DNMT3A mutations result in loss of function, dominant-negative function or gain of function. Although DNMT3A mutations in MDS seemed to have no effect on global methylation levels [29], similar DNMT3A mutations detected in AML correlated with either hypermethylation or hypomethylation of distinct genes, and concurrent gene repression and gene activation [30]. This duality might be explained by the observation that methylation by wild-type DNMT3A is required for repression of genes as well as for maintenance of active chromatin states [25]. The mechanism by which DNMT3A mutations result in hypermethylation and hypomethylation needs to be further investigated. Mutations of DNMT3A are predominantly heterozygous and constitute mainly monoallelic events. The observation that levels of mutant transcripts were similar to levels of wild-type transcript [6] suggests that patients carrying DNMT3A mutations may express both wild-type and mutant DNMT3A protein and implies that mutations may result in dominant-negative or gain of function rather than loss of function. Accordingly, overexpression of a DNMT3A gene that harbored a missense mutation promoted proliferation in myeloid 32D cells [31], which would not be observed if mutations confer mere loss of function. Mutations comprise missense mutations (86%) and truncating mutations (14%) [6, 28, 29]. The truncating mutations (n = 3) result in a predicted protein lacking either all known functional domains (p.Q237X) or the PHD-zinc finger and methyltransferase domains (p.L422fs and p.E599X) (Fig. 1b) [6, 29]. Notably, the remaining N-terminal amino acids have been implicated in DNA binding [32]; moreover, the truncated protein p.Q237X resembles isoform DNMT3A3 (166 amino acids; Fig. 1b), which is catalytically inactive and may display a regulatory function by targeting full-length DNMT3A to the chromatin [33, 34]. This isoform is not ubiquitously expressed; instead, it is present in developing gonads, testicular cells and resting fibroblasts. Therefore, the mutant (truncated) DNMT3A protein resembling DNMT3A3 might be regulatory active in cells where DNMT3A3 should not operate. If the missense mutations result in a catalytically inactive protein, they might possess the same function as the truncated proteins. The missense mutations target the methyltransferase domain (Fig. 1b), which binds to the methyl donor and catalyzes the methylation of DNA [23]. The most frequently targeted amino acid (R882, 50% of DNMT3A mutations in MDS) corresponds to DNMT3B-R823. The DNMT3B protein, a paralog of DNMT3A, catalyzes de novo DNA methylation too, and its R823 is mutated in ICF (immunodeficiency, centromeric instability, facial anomalies) syndrome [35]. The R823G mutant is catalytically active, but cannot dissociate from the DNA to search for a new target, which results in decreased activity observed in in vitro assays [35]. Consistent with this observation is the reduced activity of the R882-mutated DNMT3A proteins in in vitro assays [31]. Next to R823G, additional DNMT3B mutations in ICF syndrome have been described, which result in significant hypomethylation of heterochromatic genes in peripheral blood cells [35, 36]. Of note, these mutations comprise mostly missense mutations in the MT domain and some truncating mutations in the N-terminal region [36], thereby showing a strong resemblance to the DNMT3A mutations observed in MDS. In summary, we hypothesize that mutated DNMT3A proteins retain their DNA-binding potential but lose their potential to methylate DNA properly as they are captured onto the DNA. As azacitidine and decitabine have been described to function by capturing DNMT proteins to the DNA, the question arises whether these hypomethylating agents will be effective in cells harbouring DNMT3A mutations.
The EZH2 protein
The EZH2 protein (Fig. 1c) is a histone methyltransferase that catalyzes progressive mono- through trimethylation of H3K27 [37], for which it depends both on its C-terminal SET domain and on its interaction with the EED and SUZ12 proteins (Box 1) [38]. The different methylation levels of H3K27 play an important role in many cellular processes, including hematopoiesis, and H3K27me3 is involved in gene repression [39]. Overexpression of EZH2 has been described in various malignancies, and therefore EZH2 has been labeled as a potential oncogene [38]. In line with this, an activating point mutation in the SET domain of EZH2 (Tyr641) was identified in diverse lymphomas [37]. In contrast, no activating EZH2 mutations were found in MDS. Instead, mutations of EZH2 that result in loss of function were detected in 6% of patients with MDS [5, 40–42]. The EZH2 gene is located at chromosome 7q36.1, a region that is frequently affected in MDS by chromosome 7/7q deletions, and occasionally by microdeletions [4, 40, 42]. Microdeletions of chromosome 7q36.1 co-occurred with truncating EZH2 mutations that deleted or disrupted the important SET domain on the remaining allele, indicating that no functional EZH2 protein could be expressed in these MDS cells [40, 42]. In addition to the hemizygous mutations that result in loss of EZH2 at both alleles, biallelic homo- and heterozygous mutations were observed [40, 41]. Mutations comprised truncating and missense mutations that were scattered throughout the coding sequence. All truncating mutations resulted in the disruption or deletion of the SET domain, and most missense mutations targeted the SET domain as well. Analysis of some of these mutants showed loss of H3K27me3 in affected cells [41, 42], thereby confirming the loss of function of mutant EZH2 proteins. Mutations of EZH2 occurred in the context of normal and non-complex karyotypes (mainly del(5q), del(20q) and trisomy 8) [5, 40, 41] and co-occurred with 8% of TET2 mutations, 13% of IDH mutations and 22% of ASXL1 mutations [5], indicating that these proteins function in different epigenetic processes and that their mutations represent complementary events in the pathogenesis of MDS. Until now, the co-occurrence of EZH2 and DNMT3A mutations has not been investigated in large patient cohorts. Most of the mutations that were found in EZH2 occurred in the absence of a chromosome 7/7q deletion [5, 40–42]. The presence of EZH2 mutations correlated with adverse prognosis, comparable to the well-known poor prognosis of patients with a chromosome 7/7q deletion [3–5, 40, 41]. In multivariate analysis, the correlation with poor prognosis was shown to be independent from other known risk factors [5]. This observation is of particular relevance as most EZH2 mutations were detected in lower-risk patients [5, 40]. Since patients with chromosome 7/7q deletions particularly benefit from treatment with azacitidine [11], it might be hypothesized that patients harboring EZH2 mutations might benefit from this treatment as well. The use of EZH2 inhibitors has been suggested for the treatment of malignancies that show increased EZH2 activity [38]. The loss-of-function mutations of EZH2 that occur in MDS argues against the use of these inhibitors in myeloid malignancies.
The IDH1 and IDH2 proteins
The IDH1 protein (Fig. 1d) is located in the cytosol and peroxisomes of eukaryotic cells, whereas its paralog IDH2 (Fig. 1d) is situated in mitochondria [43, 44]. Both proteins convert isocitrate to α-ketoglutarate (α-KG; also known as 2-oxoglutarate (2-OG)) (Fig. 2a), while reducing nicotinamide adenine dinucleotide phosphate (NADP+) to NADPH. These reactions have important functions in the metabolic pathways and in the protection of mammalian cells from oxidative stress-induced tumorigenesis. Mutations in the IDH genes were first detected in brain tumours: the IDH1 gene, located at chromosome 2q33.3, is frequently mutated in grade II–III gliomas and secondary glioblastomas (50–100%), whereas the IDH2 gene, located at chromosome 15q26.1, is only occasionally mutated in these malignancies (0–7%) [45]. In MDS, the IDH genes are mutated in approximately 10% of patients [5, 19, 46–49]. The mutations comprise missense mutations, which target either one single codon in the IDH1 gene (c.394-396CGT, encoding amino acid p.R132) or one of two codons in the IDH2 gene (c.418-420CGG, encoding amino acid p.R140, or c.514-516AGG, encoding amino acid p.R172). Notably, the R140 mutations in the IDH2 gene represent the most frequently occurring mutations in MDS (61%), but have not been identified in gliomas and glioblastomas. Although the IDH2-R140, IDH2-R172 and IDH1-R132 residues reside in the active site of the proteins (Fig. 1d) [43], cells carrying IDH mutations did not show impaired levels of α-KG and NADPH [50, 51]. Apparently, these products were generated by the unaffected wild-type protein that could be expressed because mutations of the IDH genes constitute predominantly monoallelic events, leaving one allele intact [5, 19, 46–49]. The mutant IDH proteins showed a gain of function as they could convert the α-KG that is generated by wild-type IDH proteins into 2-hydroxyglutarate (2-HG) (Fig. 2a) [52]. This oncometabolite competitively inhibits α-KG-depending enzymes [52, 53], among which are the Jumonji family of histone demethylases (JHDM) [54] and the TET proteins, as will be described in the section on TET2. Since the oncometabolite 2-HG that is formed by mutant IDH proteins inhibits the function of the TET2 protein, mutations of IDH and TET2 are expected to be mutually exclusive. This hypothesis was confirmed as IDH mutations hardly co-occurred with mutations in TET2, whereas they co-occurred with approximately 7% of EZH2 mutations and 11% of ASXL1 mutations [5]. Furthermore, IDH mutations were found in the context of normal karyotype, isolated del(5q), isolated del(20q) and isolated trisomy 8 [5, 55, 56]. At present, the effect of IDH mutations on clinical outcome is not that clear, as different studies in various cohorts of patients showed different results [5, 47, 49]. Prospective studies involving large patient cohorts should be performed to clarify this issue.

Formation and function of the oncometabolite 2-HG. a Wild-type IDH proteins convert isocitrate to α-ketoglutarate (α-KG), which is converted to the oncometabolite 2-hydroxyglutarate (2-HG) by mutant IDH proteins. b 2-Hydroxyglutarate inhibits the conversion of 5-methylcytosine (5mC) into 5-hydroxymethylcytosine (5hmC) by competing with the cofactor α-KG
The TET2 protein
The TET family of proteins was shown to be able to demethylate DNA by converting 5-methylcytosine (5mC) into 5-hydroxymethylcytosine (5hmC) (Box 1) [57]. 5-Hydroxymethylcytosine can be further oxidized into formyl- and carboxylcytosine (5fC and 5cC), which can subsequently be recognized by thymine-DNA glycosylase base-excision repair enzymes and replaced by unmethylated cytosines [58, 59]. The TET proteins bind to the transcriptional start site of actively transcribed genes, indicating that they may act to keep the chromatin of active genes in an open configuration by the demethylation of CpG nucleotides. The conversion of 5mC into 5hmC by TET proteins depends on the cofactors Fe2+ and α-KG (Fig. 2b). This dependence reveals an interesting link between the TET proteins and the IDH proteins, as IDH1 and IDH2 convert isocitrate to α-KG (Fig. 2a), thereby supplying the cofactor for the TET proteins. As described in the previous section, mutations of IDH1 and IDH2 result in a gain of function; instead of catalyzing the conversion of isocitrate into α-KG, the mutant proteins convert α-KG, generated by the wild-type enzyme, into 2-HG (Fig. 2a). The generated 2-HG was shown to inhibit the function of the TET proteins by competitive binding to the α-KG binding site (Fig. 2b) [52, 53]. The TET2 protein (Fig. 1e) was also targeted by mutations in MDS and many different types of myeloid malignancies [5, 60, 61]. In MDS, mutations were found in 20–25% of cases. They appear to be more prevalent in lower-risk patients, but the presence of TET2 mutations does not appear to be an independent prognostic factor. In approximately half of the cases, TET2 mutations were bi-allelic, either by uniparental disomy, deletion or independent mutations in both copies of the gene. The occurrence of nonsense mutations at the very N-terminal part of the coding region in some patients, and deletions that span the entire gene in others, strongly suggested that the mutations result in loss of function. This was confirmed in mouse models, in which inactivation of TET2 in myeloid cells induced hematopoietic malignancies [62–64]. In line with the idea that the function of the TET2 protein is inhibited either by the oncometabolite 2-HG or by loss-of-function mutations, is the observation that IDH mutations and TET2 mutations are mutually exclusive in most patients. As loss of function of the TET2 protein results in defective 5hmC formation and inhibition of demethylation of DNA [65], the effect of hypomethylating agents in patients with TET2 mutations might be particularly efficient. Two recent studies appear to indicate that this may be the case [66, 67]. This needs to be further confirmed in larger prospective clinical trials.
Conclusion
Mutations of epigenetic regulators (ASXL1, DNMT3A, EZH2, IDH1 and IDH2, and TET2) occur frequently in myelodysplastic syndromes. The presence of ASXL1 and EZH2 mutations represents an independent factor for poor clinical outcome, and the impact of DNMT3A and IDH mutations on overall survival requires further investigation. The concurrence of several mutant proteins in a MDS clone might indicate that these proteins perform different functions in epigenesis and pathogenesis, which seems to be the case for ASXL1 and EZH2, whereas mutations that are mutually exclusive might indicate that the corresponding proteins depend on each other for proper function, as is the case for TET2 and the IDH proteins. Future functional assays and prospective clinical studies might reveal the impact of mutations on the epigenetic landscape, on the pathogenesis of MDS and on response of patients to (epigenetic) therapy.
References
Cazzola M, Della Porta MG, Travaglino E, Malcovati L. Classification and prognostic evaluation of myelodysplastic syndromes. Semin Oncol. 2011;38(5):627–34.
Tefferi A, Vardiman JW. Myelodysplastic syndromes. N Engl J Med. 2009;361:1872–85.
Nimer SD. Myelodysplastic syndromes. Blood. 2008;111:4841–51.
Haase D, Germing U, Schanz J, Pfeilstöcker M, Nösslinger T, Hildebrandt B, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110:4385–95.
Bejar R, Stevenson K, Abdel-Wahab O, Galili N, Nilsson B, Garcia-Manero G, et al. Clinical effect of point mutations in myelodysplastic syndromes. N Engl J Med. 2011;364(26):2496–506.
Walter MJ, Ding L, Shen D, Shao J, Grillot M, McLellan M, et al. Recurrent DNMT3A mutations in patients with myelodysplastic syndromes. Leukemia. 2011;25(7):1153–8.
Yoshida K, Sanada M, Shiraishi Y, Nowak D, Nagata Y, Yamamoto R, et al. Frequent pathway mutations of splicing machinery in myelodysplasia. Nature. 2011;478(7367):64–9.
Qiu J. Epigenetics: unfinished symphony. Nature. 2006;441(7090):143–5.
Figueroa ME, Skrabanek L, Li Y, Jiemjit A, Fandy TE, Paietta E, et al. MDS and secondary AML display unique patterns and abundance of aberrant DNA methylation. Blood. 2009;114(16):3448–58.
Shen L, Kantarjian H, Guo Y, Lin E, Shan J, Huang X, et al. DNA methylation predicts survival and response to therapy in patients with myelodysplastic syndromes. J Clin Oncol. 2010;28(4):605–13.
Garcia-Manero G, Fenaux P. Hypomethylating agents and other novel strategies in myelodysplastic syndromes. J Clin Oncol. 2011;29(5):516–23.
Blum W. How much? How frequent? How long? A clinical guide to new therapies in myelodysplastic syndromes. Hematology Am Soc Hematol Educ Program. 2010;2010:314–21.
Lee SW, Cho YS, Na JM, Park UH, Kang M, Kim EJ, et al. ASXL1 represses retinoic acid receptor-mediated transcription through associating with HP1 and LSD1. J Biol Chem. 2010;285(1):18–29.
Park UH, Yoon SK, Park T, Kim EJ, Um SJ. Additional Sex Comb-like (ASXL) proteins 1 and 2 play opposite roles in adipogenesis via reciprocal regulation of peroxisome proliferator-activated receptor γ. J Biol Chem. 2011;286(2):1354–63.
Cho YS, Kim EJ, Park UH, Sin HS, Um SJ. Additional Sex Comb-like 1 (ASXL1), in cooperation with SRC-1, acts as a ligand-dependent coactivator for retinoic acid receptor. J Biol Chem. 2006;281(26):17588–98.
Huh J, Tiu RV, Gondek LP, O’Keefe CL, Jasek M, Makishima H, et al. Characterization of chromosome arm 20q abnormalities in myeloid malignancies using genome-wide single nucleotide polymorphism array analysis. Genes Chromosomes Cancer. 2010;49(4):390–9.
Gelsi-Boyer V, Trouplin V, Adélaïde J, Bonansea J, Cervera N, Carbuccia N, et al. Mutations of polycomb-associated gene ASXL1 in myelodysplastic syndromes and chronic myelomonocytic leukaemia. Br J Haematol. 2009;145(6):788–800.
Boultwood J, Perry J, Pellagatti A, Fernandez-Mercado M, Fernandez-Santamaria C, Calasanz MJ, et al. Frequent mutation of the polycomb-associated gene ASXL1 in the myelodysplastic syndromes and in acute myeloid leukemia. Leukemia. 2010;24(5):1062–5.
Rocquain J, Carbuccia N, Trouplin V, Raynaud S, Murati A, Nezri M, et al. Combined mutations of ASXL1, CBL, FLT3, IDH1, IDH2, JAK2, KRAS, NPM1, NRAS, RUNX1, TET2 and WT1 genes in myelodysplastic syndromes and acute myeloid leukemias. BMC Cancer. 2010;10:401.
Thol F, Friesen I, Damm F, Yun H, Weissinger EM, Krauter J, et al. Prognostic significance of ASXL1 mutations in patients with myelodysplastic syndromes. J Clin Oncol. 2011;29(18):2499–506.
Abdel-Wahab O, Kilpivaara O, Patel J, Busque L, Levine RL. The most commonly reported variant in ASXL1 (c.1934dupG;p.Gly646TrpfsX12) is not a somatic alteration. Leukemia. 2010;24(9):1656–7.
Jurkowska RZ, Jurkowski TP, Jeltsch A. Structure and function of mammalian DNA methyltransferases. Chembiochem. 2011;12(2):206–22.
Cheng X, Blumenthal RM. Mammalian DNA methyltransferases: a structural perspective. Structure. 2008;16(3):341–50.
Tadokoro Y, Ema H, Okano M, Li E, Nakauchi H. De novo DNA methyltransferase is essential for self-renewal, but not for differentiation, in hematopoietic stem cells. J Exp Med. 2007;204(4):715–22.
Wu H, Coskun V, Tao J, Xie W, Ge W, Yoshikawa K, et al. Dnmt3a-dependent nonpromoter DNA methylation facilitates transcription of neurogenic genes. Science. 2010;329(5990):444–8.
Irizarry RA, Ladd-Acosta C, Wen B, Wu Z, Montano C, Onyango P, et al. The human colon cancer methylome shows similar hypo- and hypermethylation at conserved tissue-specific CpG island shores. Nat Genet. 2009;41(2):178–86.
Esteller M. Aberrant DNA methylation as a cancer-inducing mechanism. Annu Rev Pharmacol Toxicol. 2005;45:629–56.
Lin J, Yao DM, Qian J, Chen Q, Qian W, Li Y, et al. Recurrent DNMT3A R882 mutations in Chinese patients with acute myeloid leukemia and myelodysplastic syndrome. PLoS One. 2011;6(10):e26906.
Thol F, Winschel C, Ludeking A, Yun H, Friesen I, Damm F, et al. Rare occurence of DNMT3A mutations in myelodysplastic syndromes. Haematologica. 2011. doi:10.3324/haematol.2011.045559.
Shen Y, Zhu YM, Fan X, Shi JY, Wang QR, Yan XJ, et al. Gene mutation patterns and their prognostic impact in a cohort of 1185 patients with acute myeloid leukemia. Blood. 2011;118(20):5593–603.
Yan XJ, Xu J, Gu ZH, Pan CM, Lu G, Shen Y, et al. Exome sequencing identifies somatic mutations of DNA methyltransferase gene DNMT3A in acute monocytic leukemia. Nat Genet. 2011;43(4):309–15.
Suetake I, Mishima Y, Kimura H, Lee YH, Goto Y, Takeshima H, et al. Characterization of DNA- binding activity in the N-terminal domain of the DNA methyltransferase Dnmt3a. Biochem J. 2011;437(1):141–8.
Galetzka D, Tralau T, Stein R, Haaf T. Expression of DNMT3A transcripts and nucleolar localization of DNMT3A protein in human testicular and fibroblast cells suggest a role for de novo DNA methylation in nucleolar inactivation. J Cell Biochem. 2006;98(4):885–94.
Galetzka D, Weis E, Tralau T, Seidmann L, Haaf T. Sex-specific windows for high mRNA expression of DNA methyltransferases 1 and 3A and methyl-CpG-binding domain proteins 2 and 4 in human fetal gonads. Mol Reprod Dev. 2007;74(2):233–41.
Moarefi AH, Chédin F. ICF syndrome mutations cause a broad spectrum of biochemical defects in DNMT3B-mediated de novo DNA methylation. J Mol Biol. 2011;409(5):758–72.
Brun ME, Lana E, Rivals I, Lefranc G, Sarda P, Claustres M, et al. Heterochromatic genes undergo epigenetic changes and escape silencing in immunodeficiency, centromeric instability, facial anomalies (ICF) syndrome. PLoS One. 2011;6(4):e19464.
Sneeringer CJ, Scott MP, Kuntz KW, Knutson SK, Pollock RM, Richon VM, et al. Coordinated activities of wild-type plus mutant EZH2 drive tumor-associated hypertrimethylation of lysine 27 on histone H3 (H3K27) in human B-cell lymphomas. Proc Natl Acad Sci USA. 2010;107(49):20980–5.
Chase A, Cross NC. Aberrations of EZH2 in cancer. Clin Cancer Res. 2011;17(9):2613–8.
Cui K, Zang C, Roh TY, Schones DE, Childs RW, Peng W, et al. Chromatin signatures in multipotent human hematopoietic stem cells indicate the fate of bivalent genes during differentiation. Cell Stem Cell. 2009;4(1):80–93.
Nikoloski G, Langemeijer SMC, Kuiper RP, Knops R, Massop M, Tönnissen ERLTM, et al. Somatic mutations of the histone methyltransferase gene EZH2 in myelodysplastic syndromes. Nat Genet. 2010;42:665–7.
Ernst T, Chase AJ, Score J, Hidalgo-Curtis CE, Bryant C, Jones AV, et al. Inactivating mutations of the histone methyltransferase gene EZH2 in myeloid disorders. Nat Genet. 2010;42:722–6.
Makishima H, Jankowska AM, Tiu RV, Szpurka H, Sugimoto Y, Hu Z, et al. Novel homo- and hemizygous mutations in EZH2 in myeloid malignancies. Leukemia. 2010;24(10):1799–804.
Reitman ZJ, Yan H. Isocitrate dehydrogenase 1 and 2 mutations in cancer: alterations at a crossroads of cellular metabolism. J Natl Cancer Inst. 2010;102(13):932–41.
Fu Y, Huang R, Du J, Yang R, An N, Liang A. Glioma-derived mutations in IDH: from mechanism to potential therapy. Biochem Biophys Res Commun. 2010;397(2):127–30.
Bourne TD, Schiff D. Update on molecular findings management and outcome in low-grade gliomas. Nat Rev Neurol. 2010;6(12):695–701.
Kosmider O, Gelsi-Boyer V, Slama L, Dreyfus F, Beyne-Rauzy O, Quesnel B, et al. Mutations of IDH1 and IDH2 genes in early and accelerated phases of myelodysplastic syndromes and MDS/myeloproliferative neoplasms. Leukemia. 2010;24(5):1094–6.
Thol F, Weissinger EM, Krauter J, Wagner K, Damm F, Wichmann M, et al. IDH1 mutations in patients with myelodysplastic syndromes are associated with an unfavorable prognosis. Haematologica. 2010;95(10):1668–74.
Yoshida K, Sanada M, Kato M, Kawahata R, Matsubara A, Takita J, et al. A nonsense mutation of IDH1 in myelodysplastic syndromes and related disorders. Leukemia. 2011;25(1):184–6.
Patnaik MM, Hanson CA, Hodnefield JM, Lasho TL, Finke CM, Knudson RA, et al. Differential prognostic effect of IDH1 versus IDH2 mutations in myelodysplastic syndromes: a Mayo Clinic Study of 277 patients. Leukemia. 2011. doi: 10.1038/leu.2011.298.
Dang L, White DW, Gross S, Bennett BD, Bittinger MA, Driggers EM, et al. Cancer-associated IDH1 mutations produce 2-hydroxyglutarate. Nature. 2009;462(7274):739–44.
Gross S, Cairns RA, Minden MD, Driggers EM, Bittinger MA, Jang HG, et al. Cancer-associated metabolite 2-hydroxyglutarate accumulates in acute myelogenous leukemia with isocitrate dehydrogenase 1 and 2 mutations. J Exp Med. 2010;207(2):339–44.
Figueroa ME, Abdel-Wahab O, Lu C, Ward PS, Patel J, Shih A, et al. Leukemic IDH1 and IDH2 mutations result in a hypermethylation phenotype, disrupt TET2 function, and impair hematopoietic differentiation. Cancer Cell. 2010;18(6):553–67.
Xu W, Yang H, Liu Y, Yang Y, Wang P, Kim SH, et al. Oncometabolite 2-hydroxyglutarate is a competitive inhibitor of α-ketoglutarate-dependent dioxygenases. Cancer Cell. 2011;19(1):17–30.
Chowdhury R, Yeoh KK, Tian YM, Hillringhaus L, Bagg EA, Rose NR, et al. The oncometabolite 2- hydroxyglutarate inhibits histone lysine demethylases. EMBO Rep. 2011;12(5):463–9.
Caramazza D, Lasho TL, Finke CM, Gangat N, Dingli D, Knudson RA, et al. IDH mutations and trisomy 8 in myelodysplastic syndromes and acute myeloid leukemia. Leukemia. 2010;24(12):2120–2.
Pardanani A, Patnaik MM, Lasho TL, Mai M, Knudson RA, Finke C, et al. Recurrent IDH mutations in high-risk myelodysplastic syndrome or acute myeloid leukemia with isolated del(5q). Leukemia. 2010;24(7):1370–2.
Tahiliani M, Koh KP, Shen Y, Pastor WA, Bandukwala H, Brudno Y, et al. Conversion of 5- methylcytosine to 5-hydroxymethylcytosine in mammalian DNA by MLL partner TET1. Science. 2009;324(5929):930–5.
He YF, Li BZ, Li Z, Liu P, Wang Y, Tang Q, et al. Tet-mediated formation of 5-carboxylcytosine and its excision by TDG in mammalian DNA. Science. 2011;333(6047):1303–7.
Ito S, Shen L, Dai Q, Wu SC, Collins LB, Swenberg JA, et al. Tet proteins can convert 5- methylcytosine to 5-formylcytosine and 5-carboxylcytosine. Science. 2011;333(6047):1300–3.
Delhommeau F, Dupont S, Della Valle V, James C, Trannoy S, Massé A, et al. Mutation in TET2 in myeloid cancers. N Engl J Med. 2009;360(22):2289–301.
Langemeijer SM, Kuiper RP, Berends M, Knops R, Aslanyan MG, Massop M, et al. Acquired mutations in TET2 are common in myelodysplastic syndromes. Nat Genet. 2009;41(7):838–42.
Quivoron C, Couronné L, Della Valle V, Lopez CK, Plo I, Wagner-Ballon O, et al. TET2 inactivation results in pleiotropic hematopoietic abnormalities in mouse and is a recurrent event during human lymphomagenesis. Cancer Cell. 2011;20(1):25–38.
Moran-Crusio K, Reavie L, Shih A, Abdel-Wahab O, Ndiaye-Lobry D, Lobry C, et al. Tet2 loss leads to increased hematopoietic stem cell self-renewal and myeloid transformation. Cancer Cell. 2011;20(1):11–24.
Li Z, Cai X, Cai CL, Wang J, Zhang W, Petersen BE, et al. Deletion of Tet2 in mice leads to dysregulated hematopoietic stem cells and subsequent development of myeloid malignancies. Blood. 2011;118(17):4509–18.
Ko M, Huang Y, Jankowska AM, Pape UJ, Tahiliani M, Bandukwala HS, et al. Impaired hydroxylation of 5-methylcytosine in myeloid cancers with mutant TET2. Nature. 2010;468(7325):839–43.
Pollyea DA, Raval A, Kusler B, Gotlib JR, Alizadeh AA, Mitchell BS. Impact of TET2 mutations on mRNA expression and clinical outcomes in MDS patients treated with DNA methyltransferase inhibitors. Hematol Oncol. 2011;29(3):157–60.
Itzykson R, Kosmider O, Cluzeau T, Mansat-De Mas V, Dreyfus F, Beyne-Rauzy O, et al. Impact of TET2 mutations on response rate to azacitidine in myelodysplastic syndromes and low blast count acute myeloid leukemias. Leukemia. 2011;25(7):1147–52.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Nikoloski, G., van der Reijden, B.A. & Jansen, J.H. Mutations in epigenetic regulators in myelodysplastic syndromes. Int J Hematol 95, 8–16 (2012). https://doi.org/10.1007/s12185-011-0996-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-011-0996-3