
Abstract
The prognosis of patients receiving allogeneic hematopoietic stem cell transplantation (HSCT) for refractory acute lymphoblastic leukemia (ALL) is very poor. To improve survival rates, we attempted to intensify the conditioning regimen with daunorubicin, vincristine, prednisolone, medium-dose etoposide, cyclophosphamide, and total body irradiation (DNR/VCR/PSL plus medium-dose VP/CY/TBI). Four patients in relapse or induction failure of B-precursor ALL without other complications underwent allogeneic HSCT. Initially, chemotherapy comprising DNR 60 mg/m2 for 3 days, VCR 1.4 mg/m2 for 1 day, and PSL 60 mg/m2 for 3 days was administered, which was followed by medium-dose VP/CY/TBI; some modifications were made for individual patients. All patients achieved engraftment and complete remission after HSCT. Regimen-related toxicities were tolerable and no patient died within 100 days. Two patients were alive without disease on days 563 and 1,055. The third patient relapsed on day 951, while the fourth died on day 179 without disease. Our results indicate that intensified myeloablative HSCT should be considered for patients with refractory ALL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
We previously reported that allogeneic hematopoietic stem cell transplantation (allo-HSCT) using a conditioning regimen with medium-dose etoposide, cyclophosphamide, and total body irradiation (VP/CY/TBI) was therapeutically promising for treating acute lymphoblastic leukemia (ALL) [1]. In that study, the 3-year overall survival rate was 88.6% when the patients underwent allo-HSCT in complete remission (CR). Out of the two patients who received allo-HSCT in non-CR, one is still alive and was included in the present case series.
In a recent retrospective cohort from the Center for International Blood and Marrow Transplant Research, the 3-year overall survival rate was 16% in patients who underwent allo-HSCT in relapse or primary induction failure of ALL [2]. Although we attempted to perform HSCT in CR because of its survival benefits, relapse sometimes occurs just before the scheduled allo-HSCT. In such cases, there are two therapeutic options: patients either receive reinduction chemotherapies and undergo allo-HSCT after achieving CR or allo-HSCT is directly performed in relapse. Because it is unlikely that salvage chemotherapy will induce CR in early-relapsed ALL [3] as well as in primary induction failure, immediate allo-HSCT is considered for patients in relapse just before scheduled allo-HSCT. Terwey et al. [4] documented that reinduction chemotherapy may be omitted if patients meet the following criteria: available donor, ≤50% bone marrow blasts, short duration of first CR, and/or high-risk cytogenetics. In addition, some studies showed that patients with fewer bone marrow blasts at allo-HSCT had better outcomes [2, 5]. We hypothesized that a low leukemia burden just before allo-HSCT was necessary even if allo-HSCT was not performed in CR. Here, we present the findings for allo-HSCT in patients with relapse or primary induction failure of ALL, in whom intensified myeloablative conditioning comprising daunorubicin, vincristine, prednisolone (DNR/VCR/PSL), and medium-dose VP/CY/TBI was used.
2 Case series
Four patients with B-precursor ALL (B-ALL) in relapse or induction failure underwent allo-HSCT between July 2007 and August 2009 at the Hokkaido University Hospital [2 males, 2 females; median age at HSCT 30 years (range 18–43 years)]. Patient characteristics, basic data on allo-HSCT and outcomes are summarized in Table 1. One patient had been included in our previous study [1] (Case 1). All patients received induction chemotherapy containing DNR, VCR, and PSL at least once. No patient had any history of auto- or allo-HSCT.
Patients received DNR/VCR/PSL and medium-dose VP/CY/TBI sequentially (Table 2). Initially, DNR/VCR/PSL comprising DNR at a dose of 60 mg/m2 for 3 days, VCR at 1.4 mg/m2 (max. 2.0 mg) for 1 day, and PSL at 60 mg/m2 for 3 days was administered as a cytoreduction chemotherapy before HSCT, but some modifications were made for individual patients: Cases 1 and 2 received a decreased dosage of DNR at 60 mg/person/day, and day 3 chemotherapy was omitted in Case 4. Medium-dose VP/CY/TBI was reported previously: briefly, VP at 15 mg/m2 on days −7 and −6, CY at 60 mg/kg on days −5 and −4, and fractionated TBI at 2 Gy twice daily on days −3 to −1. Median time interval between DNR/VCR/PSL and VP/CY/TBI was 7 days (range 0–11 days). Tacrolimus and short-term methotrexate for GVHD prophylaxis, granulocyte-colony stimulating factor (G-CSF), and antibiotic prophylaxis were routinely administered. MRD status was monitored by PCR amplification of immunoglobulin DNA rearrangement, as previously reported [6], or by RT-PCR of the minor BCR–ABL fusion gene (Case 2, see Table 1).
Median nucleated cell count was 153,500/mm3 (range 47,000–634,000/mm3) and median percentage of blasts was 67.0% (range 7.2–95.0%) at the time of diagnosis of relapse or primary induction failure of ALL. Two patients underwent bone marrow examination between administration of DNR/VCR/PSL and VP/CY/TBI. Nucleated cell counts and blast percentage were 700/mm3 and 35.0% in Case 1, and 23,000/mm3 and 35.7% in Case 3, respectively, indicating that the leukemia burden was reduced. All patients achieved engraftment at a median of day 14.5 after HSCT (range 14–15 days). Median duration of neutropenia was 24.5 days (range 18–29 days). Febrile neutropenia was observed in Cases 2 and 3, and both were treated with intravenous antibiotics. Grade 3 and 4 non-hematological toxicities as determined by Common Terminology Criteria for Adverse Events version 3 were also seen in these 2 patients. Stomatitis and diarrhea were the most common regimen-related toxicities (RRT). All patients developed acute GVHD (3 grade I–II and 1 grade III–IV) and chronic GVHD (3 limited and 1 extensive).
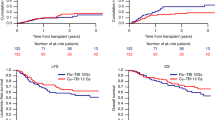
Median follow-up was 816 days (range 179–1,420 days). All patients achieved CR after allo-HSCT. Case 2 achieved molecular CR that was sustained until the final follow-up. Day 100 mortality rate was 0%. Only 1 patient (Case 1) developed a late CNS relapse (on day 951). At final follow-up, two patients were alive without disease on days 563 and 1,055, respectively, one was alive with disease on day 1,420, and one (Case 3) died on day 179 without disease.
3 Discussion
To achieve optimal outcomes in patients with acute leukemia undergoing allo-HSCT, disease status at HSCT is critical. Relapse rate in patients with relapsed ALL undergoing allo-HSCT is higher than that for CR [7]. Duval et al. [2] investigated risk factors for undergoing allo-HSCT in relapse or induction failure, with the following factors being associated with a poor prognosis: second/greater relapse or primary refractory, ≥25% bone marrow blasts, cytomegalovirus-seronegative donor, and age of ≥10 years. Three-year survival rate in patients with ALL varied between 10 and 46% according to the predictive score. Similarly, Oyekunle et al. [5] demonstrated that ≤20% bone marrow blasts at allo-HSCT was beneficial for survival. In our study, 3 patients had >30% bone marrow blasts (Table 1), and all patients were considered to have a poor prognosis according to the criteria of Duval et al.
Few studies have investigated survival in refractory acute leukemia after sequential treatment with chemotherapy and a myeloablative or non-myeloablative conditioning regimen for allo-HSCT [8–10]; however, high frequencies of relapse and treatment-related toxicities present major obstacles to survival. To overcome these drawbacks, we decided to administer DNR/VCR/PSL in anticipation of debulking of leukemia, followed by allo-HSCT using a conditioning regimen with VP/CY/TBI. While combination chemotherapies consisting of vincristine and steroids (as key drugs for ALL) and anthracyclines have been incorporated in many studies since the 1960s [11–14], these have rarely been administered as a conditioning regimen. Bone marrow blasts were reduced as expected by DNR/VCR/PSL, so that the leukemia burden could be minimized at allo-HSCT. Administration of DNR/VCR/PSL did not apparently increase the number of severe toxicities, as compared with our previous study [1]. The high CR rates, tolerable toxicities and long-term survival rates in our study are encouraging compared with results of previous studies. Improvements in supportive care might contribute to reduction in toxicity [15].
Reinduction chemotherapy followed by allo-HSCT in CR is another therapeutic option, which rarely leads to CR in early-relapsed ALL [3] or primary induction failure. Furthermore, longer reinduction schedules might lead to more infectious events during multiple neutropenic periods. In our present case series, all patients with the exception of Case 4 (primary induction failure) experienced relapse just before the scheduled allo-HSCT, indicating it was rare to predict CR with conventional chemotherapy. The duration of neutropenia was less than 1 month and no microbiologically documented infections were seen in our study, suggesting that our therapeutic approach has some advantages in reducing adverse events.
Another reinduction chemotherapy using novel anti-leukemic agents is considered in early relapse or refractory disease. Some clinical studies have been conducted in patients with relapsed or refractory ALL to assess the safety and efficacy of novel anti-leukemic agents, including nucleotide analogs [16–18] and molecular targeted agents [19, 20]. While these agents were tolerable, responses were not completely satisfactory. A few studies have suggested that these novel agents are possible candidates for a conditioning regimen [21]. It is clear that further studies are needed to determine the optimal use of these agents.
In conclusion, an intensified conditioning regimen incorporating DNR/VCR/PSL plus medium-dose VP/CY/TBI followed by allo-HSCT should be administered for selected patients. Note that intensified allo-HSCT should only be considered under clinical research programs, because our findings are based on our small retrospective case series.
References
Shigematsu A, Kondo T, Yamamoto S, Sugita J, Onozawa M, Kahata K, et al. Excellent outcome of allogeneic hematopoietic stem cell transplantation using a conditioning regimen with medium-dose VP-16, cyclophosphamide and total-body irradiation for adult patients with acute lymphoblastic leukemia. Biol Blood Marrow Transplant. 2008;14:568–75.
Duval M, Klein JP, He W, Cahn JY, Cairo M, Camitta BM, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010;28:3730–8.
Fielding AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109:944–50.
Terwey TH, Massenkeil G, Tamm I, Hemmati PG, Neuburger S, Martus P, et al. Allogeneic SCT in refractory or relapsed adult ALL is effective without prior reinduction chemotherapy. Bone Marrow Transplant. 2008;42:791–8.
Oyekunle AA, Kröger N, Zabelina T, Ayuk F, Schieder H, Renges H, et al. Allogeneic stem-cell transplantation in patients with refractory acute leukemia: a long-term follow-up. Bone Marrow Transplant. 2006;37:45–50.
Toubai T, Tanaka J, Ota S, Fukuhara T, Hashino S, Kondo T, et al. Minimal residual disease (MRD) monitoring using rearrangement of T-cell receptor and immunoglobulin H gene in the treatment of adult acute lymphoblastic leukemia patients. Am J Hematol. 2005;80:181–7.
Doney K, Hägglund H, Leisenring W, Chauncey T, Appelbaum FR, Storb R. Predictive factors for outcome of allogeneic hematopoietic cell transplantation for adult acute lymphoblastic leukemia. Biol Blood Marrow Transplant. 2003;9:472–81.
Schmid C, Schleuning M, Schwerdtfeger R, Hertenstein B, Mischak-Weissinger E, Bunjes D, et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood. 2006;108:1092–9.
Inoue M, Yasui M, Sawada A, Koyama M, Kondo O, Miyamura T, et al. Encouraging results of stem cell transplantation following a melphalan-preceding intensified preparative regimen for refractory acute leukemia in children. Rinsho Ketsueki. 2007;48:1470–7. (in Japanese).
Liu QF, Fan ZP, Zhang Y, Jiang ZJ, Wang CY, Xu D, et al. Sequential intensified conditioning and tapering of prophylactic immunosuppressants for graft-versus-host disease in allogeneic hematopoietic stem cell transplantation for refractory leukemia. Biol Blood Marrow Transplant. 2009;15:1376–85.
Mathé G, Hayat M, Schwarzenberg L, Amiel JL, Schneider M, Cattan A, et al. Acute lymphoblastic leukemia treated with a combination of prednisone, vincristine, and rubidomycin. Value of pathogen-free rooms. Lancet. 1967;290:380–2.
Larson RA, Dodge RK, Burns CP, Lee EJ, Stone RM, Schulman P, et al. A five-drug remission induction regimen with intensive consolidation for adults with acute lymphoblastic leukemia: cancer and leukemia group B study 8811. Blood. 1995;85:2025–37.
Durrant IJ, Prentice HG, Richards SM. Intensification of treatment for adults with acute lymphoblastic leukemia: results of U.K. Medical Research Council randomized trial UKALL XA. Medical Research Council Working Party on Leukaemia in Adults. Br J Haematol. 1997;99:84–92.
Annino L, Vegna ML, Camera A, Specchia G, Visani G, Fioritoni G, et al. Treatment of adult acute lymphoblastic leukemia (ALL): long-term follow-up of the GIMEMA ALL 0288 randomized study. Blood. 2002;99:863–71.
Kashiwazaki H, Matsushita T, Sugita J, Shigematsu A, Kasashi K, Yamazaki Y, et al. Professional oral health care reduces oral mucositis and febrile neutropenia in patients treated with allogeneic bone marrow transplantation. Support Care Cancer. doi:10.1007/s00520-011-1116-x (published online February 15, 2011).
Kurtzberg J, Ernst TJ, Keating MJ, Gandhi V, Hodge JP, Kisor DF, et al. Phase I study of 506U78 administered on a consecutive 5-day schedule in children and adults with refractory hematologic malignancies. J Clin Oncol. 2005;23:3396–403.
Kantarjian H, Gandhi V, Cortes J, Verstovsek S, Du M, Garcia-Manero G, et al. Phase 2 clinical and pharmacologic study of clofarabine in patients with refractory or relapsed acute leukemia. Blood. 2003;102:2379–86.
Advani AS, Gundacker HM, Sala-Torra O, Radich JP, Lai R, Slovak ML, et al. Southwest Oncology Group Study S0530: a phase 2 trial of clofarabine and cytarabine for relapsed or refractory acute lymphocytic leukaemia. Br J Haematol. 2010;151:430–4.
Raetz EA, Cairo MS, Borowitz MJ, Blaney SM, Krailo MD, Leil TA, et al. Chemoimmunotherapy reinduction with epratuzumab in children with acute lymphoblastic leukemia in marrow relapse: a Children’s Oncology Group Pilot Study. J Clin Oncol. 2008;26:3756–62.
Schindler J, Gajavelli S, Ravandi F, Shen Y, Parekh S, Braunchweig I, et al. A phase I study of a combination of anti-CD19 and anti-CD22 immunotoxins (Combotox) in adult patients with refractory B-lineage acute lymphoblastic leukaemia. Br J Haematol. doi:10.1111/j.1365-2141.2011.08762.x (published online July 7, 2011).
McGregor BA, Brown AW, Osswald MB, Savona MR. The use of higher dose clofarabine in adults with relapsed acute lymphoblastic leukemia. Am J Hematol. 2009;84:228–30.
Acknowledgments
The authors sincerely thank all the involved clinical staff.
Conflict of interest
None of the authors has a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Arita, K., Kondo, T., Sugita, J. et al. Sequential chemotherapy and myeloablative allogeneic hematopoietic stem cell transplantation for refractory acute lymphoblastic leukemia. Int J Hematol 94, 291–295 (2011). https://doi.org/10.1007/s12185-011-0919-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-011-0919-3