
Abstract
Purpose of Review
Numerous surgical techniques are available to treat osteochondral defects of the knee. The aim of this review is to analyse these procedures, including their methodology, outcomes and limitations, to create a treatment algorithm for optimal management.
Recent Findings
Osteochondral defects of the knee significantly alter the biomechanics of the joint. This can cause symptomatic and functional impairment as well as considerable risk of progressive joint degeneration. Surgical interventions aim to restore a congruent, durable joint surface providing symptomatic relief and reducing the risk of early arthritic changes. These methods include fixation, chondroplasty, microfracture, autologous matrix-induced chondrogenesis, autograft transplants, allograft transplants and autologous chondrocyte implantation. There is currently much debate as to which of these methods provides optimal treatment of osteochondral defects.
Summary
The overall evidence supports the use of each technique depending on the individual characteristics of the lesion. New technologies provide exciting prospects; however, long-term outcomes for these are not yet available.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteochondral defects of the knee occur when a unit of articular cartilage is removed from the surface of a joint with or without a portion of the underlying bone. These can occur as a result of mechanical factors (i.e. trauma or overuse leading to repetitive micro trauma) or biological factors (i.e. osteochondritis dissecans or osteonecrosis) [1]. Symptomatic defects can cause pain, locking, swelling and functional impairment with reports that these symptoms can be worse than those of an anterior cruciate ligament–deficient knee or even those awaiting a knee replacement [2]. The natural history of these defects typically results in the production of type I collagen in the form of fibrocartilage, rather than type II collagen normally found in articular, hyaline cartilage. Fibrocartilage has poorer characteristics with regard to resilience, stiffness and wear properties and, as such, has a predilection for advancing arthritis [3]. The aim of any surgical treatments of such defects is to re-establish the joint surface with hyaline cartilage to provide a congruent joint with correct alignment, symptomatic relief and reduce the risk of progressive arthritic changes requiring further intervention.
The ICRS (International Cartilage Repair Society) classify defects on a scale of grade 0 to 4 depending on the depth of the defect and involvement of subchondral bone (see Table 1) [4]. The risk of premature arthritis becomes inevitable in grade 3–4 defects due to articular incongruity [5]. As such, most treatments are aimed at these groups. Defects can also be classified by their anatomical location (such as medial femoral condyle, lateral femoral condyle or patellofemoral compartment) or the size of articular surface lost (in cm2).
Conservative management, including restricting physical activity and physiotherapy, have yielded average healing rates of 61% (range 10–95%). Poor prognosis is found in larger lesion size > 12 mm2, lesion stability and age (open physis) [6]. Patients in these cohorts and those with mechanical symptoms (locking or swelling) should be considered for surgical management.
Numerous surgical techniques exist to address these defects which exemplifies the difficulty in reproducing the function of hyaline cartilage and a congruent articular surface. Treatment options can be described as palliation (e.g. chondroplasty or microfracture), repair (fixation) or restoration (osteochondral autograft transplant (OAT), autologous matrix induced-chondrogenesis (AMIC), autologous chondrocyte implantation (ACI)) [7].
Fixation
Fixation of the osteochondral fragment into the defect is the first surgical option to be considered as this has potential to perfectly restore the native articular surface. It has been suggested that this is indicated if the fragment is partially or totally detached, in a weight-bearing zone and larger than 1 cm2 (fragments smaller than this are vulnerable to fragmentation on attempted fixation) [8]. This can be performed open or arthroscopically where the defect base is usually freshened by microfracture or drilling to provide blood supply to the fragment which is subsequently reattached.
A variety of fixation methods exist, the choice of which is largely dependent on the individual surgeon’s preference. Initially, Kirchner wires were used [9]; however, progression of technologies has led to the development of headless cannulated compression screws and bioabsorbable devices (such as pins or nails) which are naturally resorbed eliminating any requirement for routine removal. Research comparing these two fixation methods is limited, and as such, it is difficult to recommend the optimal surgical technique for this. One advantage of bioabsorbable devices is that they do not require routine removal; however, the majority of compression screws are not removed unless they become problematic. Whilst there are no randomised controlled trials (RCTs) comparing the two techniques, both have demonstrated good rates of radiographic healing (82% with metal headless compression screws [10] and 67% with bioabsorbable devices [11]). Whilst union rates may appear lower with bioabsorbable devices, it is worth noting the average defect size was larger in this cohort (average 5.3 cm2 vs. 3.8 cm2), a significant confounding factor. Both studies reported good International Knee Documentation Committee scores (or IKDC—one of many joint-specific subjective assessments of patient-reported outcomes) of 85 and 82 at follow-up of 5 years or greater. A recent systematic review reported good to excellent results of fixation methods from 13 studies, demonstrating radiographic union in 67–100% and improved patient-reported outcomes. Nevertheless, re-operation was common with reports of up to 44% requiring further procedures [12]. The most common reason for further surgery was excision of loose body fragments; however, chondral revision, chondral resurfacing procedures and unplanned removal of hardware were also reported. Unfortunately, they were unable to recommend an optimal fixation method or risk factors of failure due to the poor level of data restricted to mostly level 4 case series. This is clearly an area that could benefit from further research.
Chondroplasty
Chondroplasty involves debriding the edges of the defect to smooth the margins. Theoretically, this will reduce friction and risk of propagation resulting in a joint that moves more freely and with less pain. Traditionally done arthroscopically with a mechanical shaver, the newer method of using radiofrequency energy (RFE) is thought to create a plasma layer that might strengthen the cartilage base by realigning the collagen fibres and annealing the surface [13]. One RCT comparing the two techniques for grade 3 defects of medial femoral condyle demonstrated better Knee and Osteoarthritis Outcome Severity (KOOS) and physical activity (Tegner) scores in those treated with RFE [14]. Short-term improvements subsequent to RFE were also demonstrated in a large case series which also reported low complication and re-operation rates (2.2% and 2.7%, respectively) at 6 months [15]. As well as improved short-term results, longer follow-up of the same RCT has shown a significantly longer mean time to revision in those treated with RFE (94.1 vs. 62.5 months) [16].
It has been suggested that chondroplasty is best reserved for grade 2 or 3 defects, with the efficacy of attempting to create a plasma layer on grade 4 defects remaining unclear [13]. The use of RFE was reviewed by the National Institute of Health and Care Excellence (NICE) with guidelines suggesting that, whilst evidence for the procedure is limited, the short-term benefits and low safety concerns mean the procedure can be used with normal arrangements for clinical governance. Nonetheless, they do suggest the procedure is only performed by clinicians with specific training of the technique [17].
Microfracture
Bone marrow stimulation, via microfracture or drilling, aims to allow mesenchymal stem cells to migrate from the underlying bone marrow to the articular surface where they can form an amalgam of bone and fibrocartilage [18]. By filling the defect, this improves joint congruency and reduces the risk of early osteoarthritis [19]. Unfortunately, fibrocartilage lacks the mechanical integrity of hyaline cartilage, and it has been suggested that degeneration of repair tissue and deteriorate of clinical outcomes is an expectant result. Many studies have demonstrated that patient-reported outcomes improve significantly in the short to medium term (up to 5 years postoperatively). Unfortunately, this is usually followed by a decline in outcomes with reports of subjective scores comparable to preoperative levels 15 years postoperatively [20,21,22,23,24]. Complications are not uncommon, such as early OA reported in 40–50% of cases [25, 26] and bone overgrowth which is visualized on MRI in 63% of cases at 2 years. Whilst overgrowth is rarely symptomatic, with no significant difference in KOOS scores between those radiographically diagnosed with or without overgrowth, it does predict a significantly higher failure rate (25% vs. 3%) [27]. Risk factors for poorer outcomes include long-standing symptoms, poor baseline Lysholm score, concurrent mild degenerative changes or partial meniscectomy [23].
Continuing evolution of the technique has led to the advent of nanofracture. This aims to make finer perforations deeper into the subchondral bone, the advantage being less trabecular fragmentation and compaction. This has been demonstrated to provide better restoration of bone architecture and cartilage quality in ovine models [28] and defects of the talus [29]; however, studies on the knee have yet to be published.
Microfracture continues to be popular, largely due to its good short- to medium-term results and cost-effectiveness [30]. It has been suggested that this procedure is reserved for small defects in patients with low postoperative demands [31].
Autologous Matrix-Induced Chondrogenesis
AMIC involves a cell-free microstructural scaffold being laid over the defect after it has been debrided and stimulated (e.g. microfractured or drilled). The synthetic covering is cut to size and adhered with sutures or fibrin glue with the aim of capturing the bone marrow cells and stem cells released by the bone stimulation and subsequently provide a scaffolding network in which the cartilage can grow. RCTs comparing the use of scaffold insertion to microfracture have repeatedly demonstrated superior filling of defect and quantity of hyaline cartilage on MRI [22, 32]. Whilst clinical outcomes are equivalent at 12 months [32], AMIC appears to prevent the regression of outcomes commonly seen in microfracture with one RCT demonstrating significantly superior outcomes at 2 and 5 years. This trial included defects greater than 2 cm2 and found that only 7% of AMIC patients reported deteriorating outcomes at 5 years compared with 66% of MFx cases [22]. Modified Cincinnati score, pain scores and MRI outcomes were also significantly superior.
Unfortunately, literature on this subject is limited with no long-term results published yet. However, the relative simplicity and lack of specialist resources required in comparison to other techniques is appealing.
Osteochondral Autograft Transplant and Mosaicplasty
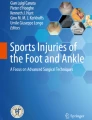
When a primary repair is not possible, osteochondral autograft transplant allows defects to be filled by harvesting tissue from a less important anatomical location (typically the margins of the femoral condyles or intercondylar notch). Similar to OAT, mosaicplasty also relies on transplanting articular cartilage using multiple smaller osteochondral grafts which are harvested and transplanted to fill the defect with a mosaic of smaller plugs [33]. Figure 1 demonstrates both of these techniques. Both procedures can be performed open or arthroscopically and provide immediate coverage with mature, hyaline articular cartilage. One additional benefit is the ability to control depth of the donor graft, facilitating a more congruent coverage and filling of the defect [34].

Illustration comparing OATS and mosaicplasty procedures
Debate regarding superiority of these two procedures continues. Whilst mosaicplasty benefits from reduced donor-site morbidity, there are concerns that fibrocartilage formation between plugs creates a mixed healing result [35]. Data from a systematic review imply that mosaicplasty is typically used for larger defects than OAT (2.71 cm2 vs. 1.02 cm2) [33]. This review found that outcome scores were better for OAT procedures; however, with such a large discrepancy in defect size, it is difficult to interpret these results. Good results have been reported; however, successful long- and medium-term results are strongly reliant on appropriate patient selection. In a series of 73 mosaicplasties, the risk of poor outcomes (defined as Lysholm score less than 64 or requiring arthroplasty surgery) at 10–14 years were reduced from 40 to 12.5% with appropriate patient selection. Risk factors for poorer outcomes were age 40 years or older (59%), female (61%) and defects larger than 3 cm2 (57%). Conversely, failure rates were low in males under 40 with defects smaller than 3 cm2 (12.5%) [36]. Other reports advocate use of the procedure in young, active patients [20].
When compared with microfracture, mosaicplasty demonstrated considerably lower rates of symptom recurrence 10 years postoperatively. This was found in all but one of the studies included in a Cochrane review evaluating long-term outcomes [20]. It is worth noting that the one randomized control trial included in this review that found no significant difference between the treatments had a small number of cases (14 mosaicplasty vs. 11 MFx) [26] which may reflect a steep learning curve associated with the procedure.
Whilst the procedure can have good results, obtaining a curved, congruent surface with donor implants is a technically challenging skill. As such, NICE guidelines require the procedure to be performed by experienced cartilage surgeons, with patient data uploaded to the ICRS Patient Registry for audit purposes [37].
Osteochondral Allografts
On some occasions, defects are so large that concerns of donor-site morbidity can prevent reconstruction via OAT or mosaicplasty procedures. For such cases, the use of osteochondral allograft (OCA) transplant has been suggested. Here fresh, fresh frozen or cryopreserved cadaveric samples are used to fill the defects. Fresh allografts do not required blood type or human leukocyte antigen matching due to the barrier that the intact hyaline cartilage provides [38]; however, their short shelf life (28 days from harvesting) and higher cost can restrict their availability [39]. Unfortunately, the processing and storage techniques of fresh frozen and cryopreserved treatments risk loss of up to 95% of chondrocytes in the sample [40]. Fresh samples appear to be most popular, being the most used allograft in a systematic review on the subject [38].
OCA has demonstrated favourable outcomes with radiographic union in 86% and excellent or good results in 86–89% at 2 years [39]. However, long-term results show a significant deterioration with survival rates falling from 95% at 5 years to 80–85% at 10 years and 65–74% at 15 years [41,42,43], whilst re-operation rates requiring revision or arthroplasty procedures of 32–47% in the first 10 years have been reported [41]. Risk factors for poor outcomes include age over 30 and those who have received three or more prior procedures [39] [43].
Research on the subject is largely composed of historic case series with a distinct lack of comparative studies or modern papers available suggesting that the development of restoration techniques has reduced demand for this procedure. Nevertheless, it remains an option for larger, deep defects (> 3 cm2 grade 4) or revision procedures [40].
Autologous Chondrocyte Implantation
Autologous chondrocyte implantation (ACI) is a two-stage process that aims to harvest chondrocytes from the patient via a 0.5–1-cm fragment, as demonstrated in Fig. 2. Chondrocytes from the sample are isolated and reproduced in vitro, and subsequently replanted into the defect along with a protective coverage 3–5 weeks later [44]. The procedure continues to see advancing developments. First-generation techniques used a layer of periosteum autograft to protect and contain chondrocytes, whilst the second generation used a piece of porcine collagen membrane. Third-generation techniques termed MACI (matrix-induced autologous chondrocyte implantation, not to be confused with AMIC) impregnate the chondrocytes into the collagen matrix in vitro, rather than the matrix being applied on top of cellular material.

Illustration demonstrating autologous chondrocyte implantation (ACI) procedure
Long-term results for first-generation techniques were generally poor, with no significant difference in comparison with MFx in several studies. In fact, one RCT with long-term results demonstrated that patients receiving ACI had a higher rate of failure than those receiving MFx (43% vs. 34%) at 14–15 years of follow-up. ACI patients were also more likely to require subsequent conversion to a total knee replacement (15% vs. 8%) [25]. In another case series, failure rates of 37% were reported after 20 years with 16% requiring conversion to a knee replacement. On average, arthroplasty was performed in under 6 years after the index procedure [45].
Results improved with second-generation techniques, with superior outcomes in comparison with mosaicplasty in larger defects (mean 4.0–4.4 cm2). In the present study, failure rates (defined as arthroscopic evidence of failure of the graft, or revision surgery of any kind) were actually superior with mosaicplasty in the short term (for the first 2 years); however, these patients subsequently suffered a steep decline which was not seen in the ACI cohort. At 10 years, ACI had significantly lower failure rates (17% vs. 55%) and better subjective outcome scores (Cincinnati and Bentley–Stanmore scores) [44].
Evolution of techniques and the use of MACI have seen further improvement with results. The SUMMIT trial is an ongoing, prospective, multicentre trial comparing MACI with microfracture in defects > 3 cm2. Their 5-year results have demonstrated superior outcome scores (KOOS, Cincinnati and Visual Analogue Scores) in those who received MACI. Impressively, the results for those treated with MACI appear to get better with time as serial results showed continued improvement between 2 and 5 years of follow-up. Reassuringly, treatment failures were minimal in both groups [46]. This improvement in clinical outcomes over time has also been demonstrated in a case series evaluating outcomes up to 5 years [47].
Current NICE guidelines recommend MACI as an option for treating symptomatic grade 3 or 4 defects greater than 2 cm2 in patients who have minimal arthritic changes and no previous surgical repairs to the articular cartilage [48]. Long-term results from the SUMMIT trial and other studies are required prior to more widespread use of the technique.
Discussion
The large number of treatment options available for osteochondral defects highlights the challenge of reproducing the articular surface of the knee. A recent meta-analysis aimed to compile results from all RCTs on the subject. Using data from 21 RCTs on microfracture, OAT, ACI and MACI, they found that the re-operation, re-intervention and adverse event rates were similar for all procedures. However, microfracture demonstrated the worst patient-reported outcomes, with particular emphasis placed on the poor long-term results of this operation. They concluded that cartilage repair techniques provided higher quality repair of tissue, lower failure rates and higher return to activity rates in comparison to MFx. According to efficacy and safety, they recommended that ACI was the best intervention, followed by OAT [49]. Unfortunately, no RCTs have been conducted on AMIC or OCA and hence outcomes of these treatments were not included for comparison.
It has previously been suggested that procedure choice is determined by size of the defect; however, consideration must also be taken regarding depth/ICRS grade of the defect and patient factors (including age, activity levels and associated degenerative changes). Whilst microfracture has previously been considered procedure of choice for defects < 2 cm2 [50], long-term results of this procedure and advancing technology make this difficult to justify. Nevertheless, the good short-term results, relative ease and low cost make it a common choice in reality. It is possible that the development of nanofracture techniques may improve long-term results; however, more research on the technique is required.
Conclusion
In general, fixation of fragments is the treatment of choice in the acute setting provided the bone fragment is of sufficiently good quality and size (> 1 cm2). Low-grade defects (ICRS grade 2) should be treated with chondroplasty to avoid propagation of the defect. Smaller grade 3–4 defects (< 3 cm2) are best treated with OAT or mosaicplasty depending on surgeon preference and defect configuration. It is probable that AMIC will have a developing role in smaller defects; however, the lack of long-term results of randomized studies mean this should be used with caution. Larger defects (> 3 cm2) should receive ACI. However, OCA or MACI treatment is a viable alternative if ACI is unavailable. This algorithm is summarized in Fig. 3.

Treatment algorithm for osteochondral defects of the knee
References
Grimm NL, Weiss JM, Kessler JI, Aoki SK. Osteochondritis dissecans of the knee: pathoanatomy, epidemiology, and diagnosis. Clin Sports Med. 2014;33(2):181–8.
Heir S, Nerhus TK, Røtterud JH, Løken S, Ekeland A, Engebretsen L, et al. Focal cartilage defects in the knee impair quality of life as much as severe osteoarthritis: a comparison of knee injury and osteoarthritis outcome score in 4 patient categories scheduled for knee surgery. Am J Sports Med. 2010;382:231–7.
Craig W, David JW, Ming HZ. A current review on the biology and treatment of the articular cartilage defects [part I & part II]. J Musculoskelet Res. 2003;7:157–81.
Bohndorf K. Osteochondritis [osteochondrosis] dissecans a review and new MRI classification. Eur Radiol. 1998;8:103–12.
Sanders TL, Pareek A, Obey MR, Johnson NR, Carey JL, Stuart MJ, et al. High rate of osteoarthritis after osteochondritis dissecans fragment excision compared with surgical restoration at a mean 16-year follow-up. Am J Sports Med. 2017;45:1799–805.
Andriolo L, Candrian C, Papio T, Cavicchioli A, Perdisa F, Filardo G. Osteochondritis dissecans of the knee—conservative treatment strategies: a systematic review. Cartilage. 2019;10(3):267–77.
McNickle AG, Provencher MT, Cole BJ. Sports .Overview of existing cartilage repair technology. Sports Med Arthrosc. 2008;16:196–201.
Robert H, Elise S, Dubois H. Osteochondritis dissecans of the knee, results of 43 refixations. Arthroskopie. 1998;11:177–81.
Federico DJ, Lynch JK, Jokl P. Osteochondritis dissecans of the knee: a historical review of etiology and treatment. Arthroscopy. 1990;6:190–7.
Barrett I, King AH, Riester S, van Wijnen A, Levy BA, Stuart MJ, et al. Internal fixation of unstable osteochondritis dissecans in the skeletally mature knee with metal screws. Cartilage. 2016;7:157–62.
Millington KL, Shah JP, Dahm DL, Levy BA, Stuart MJ. Bioabsorbable fixation of unstable osteochondritis dissecans lesions. Am J Sports Med. 2010;38:2065–70.
Leland DP, Bernard CD, Camp CL, Nakamura N, Saris DBF, Krych AJ. Does internal fixation for unstable osteochondritis dissecans of the skeletally mature knee work? A systematic review. Arthroscopy. 2019;35(8):2512–22.
Anderson SR, Faucett SC, Flanigan DC, Gmabardella RA, Amin NH. The history of radiofrequency energy and Coblation in arthroscopy: a current concepts review of its application in chondroplasty of the knee. J Exp Orthop. 2019;6:1.
Spahn G, Kahl E, Muckley T, Hofmann GO, Klinger HM. Arthroscopic knee chondroplasty using a bipolar radiofrequency-based device compared to mechanical shaver: results of a prospective, randomised, controlled study. Knee Surg Sports Traumatol Arthrosc. 2008;16:565–73.
Gharaibeh M, Szomor A, Chen DB, MacDessi SJ. A retrospective study assessing safety and efficacy of bipolar radiofrequency ablation for knee chondral lesions. Cartilage. 2018;9(3):241–7.
Spahn G, Hofmann GO, von Engelhardt LV. Mechanical debridement versus radiofrequency in knee chondroplasty with concomitant medial meniscectomy: 10-year results from a randomized controlled study. Knee Surg Sports Traumatol Arthrosc. 2016;24(5):1560–8.
Arthroscopic radiofrequency chondroplasty for discrete chondral defects of the knee. National Institute for Health and Care Excellence. 2014, Vol. IPG493. https://www.nice.org.uk/guidance/ipg493. Accessed 4th May 2020.
Steadman JR, Rodkey WG, Briggs KK, Rodrigo JJ. The microfracture technic in the management of complete cartilage defects in the knee joint. Orthopade. 1999;28:26–32.
Madry H, Kon E, Condello V, Peretti GM, Steinwachs M, Seil R, et al. Early osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc. 2016;18:419–33.
Kowalczuk M, Musahl V, Fu FH. Cochrane in CORR: surgical interventions [microfracture, drilling, mosaicplasty, and allograft transplantation] for treating isolated cartilage defects of the knee in adults. Clin Orthop Relat Res. 2018;476(1):16–8.
Minas T, Gomoll AH, Rosenberger R, Royce RO, Bryant T. Increased failure rate of autologous chondrocyte implantation after previous treatment with marrow stimulation techniques. Am J Sports Med. 2009;37:902–8.
Volz M, Schaumburger J, Frick H, Grifka J, Anders S. A randomized controlled trial demonstrating sustained benefit of autologous matrix-induced chondrogenesis over microfracture at five years. Int Orthop. 2017;41(4):797–804.
Solheim E, Hegna J, Inderhaug E, Oyen J, Harlem T, Strand T. Results at 10–14 years after microfracture treatment of articular cartilage defects in the knee. Knee Surg Sports Traumatol Arthrosc. 2016;24:1587–93.
Orth P, Gao L, Madry H. Microfracture for cartilage repair in the knee: a systematic review of the contemporary literature. Knee. 2020;28:670–706.
Knutsen G, Drogset JO, Engebretsen L, Grontvedt T, Ludvigsen TC, Loken S, et al. A randomized multicenter trial comparing autologous chondrocyte implantation with microfracture: long-term follow-up at 14 to 15 years. J Bone Joint Surg Am. 2016;98:1332–9.
Ulstein S, Aroen A, Rotterud JH, Loken S, Engebretsen L, Heir S. Microfracture technique versus osteochondral autologous transplantation mosaicplasty in patients with articular chondral lesions of the knee: a prospective randomized trial with long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2014;22:1207–15.
Mithoefer K, Venugopal V, Manaqibwala M. Incidence, degree, and clinical effect of subchondral bone overgrowth after microfracture in the knee. Am J Sports Med. 2016;44:2057–63.
Zedde P, Cudoni S, Giachetti G, Manunta ML, Masala G, Brunetti A, et al. Subchondral bone remodeling: comparing nanofracture with microfracture. An ovine in vivo study. Joints. 2016;4(2):87–93.
Tahta M, Akkaya M, Gursoy S, Isik C, Bozkurt M. Arthroscopic treatment of osteochondral lesions of the talus: nanofracture versus hyaluronic acid-based cell-free scaffold with concentration of autologous bone marrow aspirate. J Orthop Surg [Hong Kong]. 2017;25(2):2309499017717870.
Aae TF, Randsborg PH, Luras H, Aroen A, Lian OB. Microfracture is more cost-effective than autologous chondrocyte implantation: a review of level 1 and level 2 studies with 5 year follow-up. Knee Surg Sports Traumatol Arthrosc. 2018;26(4):1044–52.
Goyal D, Keyhani S, Lee EH, Hui JH. Evidence-based status of microfracture technique: a systematic review of level I and II studies. Arthroscopy. 2013;29(9):1579–88.
Stanish WD, McCormack R, Forriol F, Mohtadi N, Pelet S, et al. Novel scaffold-based BST-CarGel treatment results in superior cartilage repair compared with microfracture in a randomized controlled trial. J Bone Joint Surg Am. 2013;95(18):1640–50.
Kizaki K, El-Khechen HA, Yamashita F, Duong A, Simunovic N, Musahl V, et al. Arthroscopic versus open osteochondral autograft transplantation [mosaicplasty] for cartilage damage of the knee: a systematic review. J Knee Surg. 2019;9:2019
Marcacci M, Filardo G, Kon E. Treatment of cartilage lesions: what works and why? Injury. 2013;44(Suppl 1):S11–5.
CJ W. Treatment of focal articular cartilage lesions of the knee with autogenous osteochondral grafts: a 2- to 4-year follow-up study. Arch Orthop Trauma Surg. 2002;122:169–72.
Solheim E, Hegna J, Øyen J, Harlem T, Strand T. Results at 10 to 14 years after osteochondral autografting [mosaicplasty] in articular cartilage defects in the knee. Knee. 2013;20(4):287–90.
Mosaicplasty for symptomatic articular cartilage defects of the knee. IPG607. National Institute for Health and Care Excellence. 2018. https://www.nice.org.uk/guidance/ipg607 Accessed 4th May 2020.
Sherman SL, Garrity J, Bauer K, Cook J, Stannard J, Bugbee W. Fresh osteochondral allograft transplantation for the knee: current concepts. J Am Acad Orthop Surg. 2014;22(2):121–33.
Chahal J, Gross AE, Gross C, Mall N, Dwyer T, Chahal A, et al. Outcomes of osteochondral allograft transplantation in the knee. Arthroscopy. 2013;29(3):575–88.
Pisanu G, Cottino U, Rosso F, Blonna D, Marmotti AG, Bertolo C, et al. Large osteochondral allografts of the knee: surgical technique and indications. Joints. 2018;6(1):42–53.
Gross AE, Shasha N, Aubin P. Long-term follow-up of the use of fresh osteochondral allografts for posttraumatic knee defects. Clin Orthop Relat Res. 2008;466(8):1863–70.
Aubin PP, Cheah HK, Davis AM, Gross AE. Long-term follow-up of fresh femoral osteochondral allografts for posttraumatic knee defects. Clin Orthop Relat Res. 2001;391:S318–27.
Levy YD, Gortz S, Pulido PA, McCauley JC, Bugbee WD. Do fresh osteochondral allografts successfully treat femoral condyle lesions? Clin Orthop Relat Res. 2013;471:231–7.
Bentley G, Biant LC, Vijayan S, Macmull S, Skinner JA, Carrington RW. Minimum ten-year results of a prospective randomised study of autologous chondrocyte implantation versus mosaicplasty for symptomatic articular cartilage lesions of the knee. J Bone Joint Surg (Br). 2012;94(4):504–9.
Ogura T, Mosier BA, Bryant T, Minas T. A 20-year follow-up after first-generation autologous chondrocyte implantation. Am J Sports Med. 2017;45(12):2751–61.
Brittberg M, Recker D, Ilgenfritz J, Saris DBF. SUMMIT Extension Study Group. Matrix-applied characterized autologous cultured chondrocytes versus microfracture: five-year follow-up of a prospective randomized trial. Am J Sports Med. 2018;46(6):1343–51.
Marlovits S, Aldrian S, Wondrasch B, Zak L, Albrecht C, Welsch G, et al. Clinical and radiological outcomes 5 years after matrix-induced autologous chondrocyte implantation in patients with symptomatic, traumatic chondral defects. Am J Sports Med. 2012;40(10):2273–80.
Autologous chondrocyte implantation using chondrosphere for treating symptomatic articular cartilage defects of the knee. TA508. National Institute for Health and Care Excellence. 2018. https://www.nice.org.uk/Guidance/TA508. Accessed 4th May 2020.
Zamborsky R, Danisovic L. Surgical techniques for knee cartilage repair: an updated large-scale systematic review and network meta-analysis of randomized controlled trials. Arthroscopy. 2020;36(3):845–58.
Richter DL, Schenck RC, Wascher DC, Treme G. Knee articular cartilage repair and restoration techniques: a review of the literature. Sports Health. 2016;8(2):153–60.
Funding
The authors did not receive support from any organisation for the submitted work.
Author information
Authors and Affiliations
Contributions
M.H. and C.G. contributed to the study conception and design. Data collection and analysis were performed by M.H. and C.G. The first draft of the manuscript was written and edited by M.H. and Q.L. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Howell, M., Liao, Q. & Gee, C.W. Surgical Management of Osteochondral Defects of the Knee: An Educational Review. Curr Rev Musculoskelet Med 14, 60–66 (2021). https://doi.org/10.1007/s12178-020-09685-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12178-020-09685-1