
Abstract
Background
Nurses are a stressed group and this may affect their health and work performance. The determinants of occupational stress in nurses and other occupational groups have almost invariably been examined in between subject studies.
Purpose
This study aimed to determine if the main determinants of occupation stress, i.e. demand, control, effort and reward, operate within nurses.
Methods
A real time study using personal digital-assistant-based ecological momentary assessment to measure affect and its hypothesised determinants every 90 min in 254 nurses over three nursing shifts. The measures were negative affect, positive affect, demand/effort, control and reward.
Results
While the effects varied in magnitude between people, in general increased negative affect was predicted by high demand/effort, low control and low reward. Control and reward moderated the effects of demand/effort. High positive affect was predicted by high demand/effort, control and reward.
Conclusions
The same factors are associated with variations in stress-related affect within nurses as between.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nursing is often stressful [1] and associated with burnout [2] intention to leave the profession [3] and errors and safety violations [4, 5] which may be distress related [6]. It is therefore important to study stress in nurses both to increase our understanding of the processes that determine stress and because of the potential impact stressed nurses may have on the delivery and outcome of health care.
Two models of the causes of work-related stress dominate the literature on the environmental effects of stress: Karasek’s [7] demand control model and Siegrist’s [8] effort reward imbalance model. Karasek hypothesises that high demand is associated with stress but this is moderated by control so that the combination of high demand and low control is particularly stressful, while Siegrist proposes that high extrinsic effort (a very similar concept to demand) causes stress but this is moderated by reward so that high effort and low reward (the effort reward imbalance) leads to most stress. These models both in their original form and with additions and modifications [9] have received extensive study. There is considerable support for the central importance of demand or effort, control and reward as determinants of stress and some, less consistent, support for the role of control and reward as moderators of the effects of demand and effort [10–12]. Studies of nurses have shown that high demand and low control relates to poor physical and mental functioning [13], increased sickness absence [14] and burnout [15]. Similarly effort reward imbalance has been shown to relate to poor general health and psychological wellbeing [16], the intention to quit nursing [17] and burnout [18, 19].
Virtually all studies of occupational stress have examined the differences in stress and its determinants between people and attempted to determine, for example, whether people in high strain occupations or who perceived their work to have many demands or low control or reward report more stress and experience more ill health [e.g., 20, 21]. Very few studies have examined if the processes that determine the differences between people are also associated with variations in stress within people. It has been very forcibly argued that at a fundamental level psychological theories should apply to and be tested within people and that processes and theories that are important in differentiating between people do not necessarily apply within an individual [22]. This can have important implications for interventions to reduce stress and its consequences. First, many interventions are directed at changing what are thought to be critical processes within the individual. If these processes are not in fact critical for most individuals then such interventions are unlikely to be helpful and could even be harmful for some. Second, the alternative approach is to change aspects of the environment, especially the work environment, and the effects can only be assessed by observing changes within individuals experiencing different environmental conditions.
Stone and Shiffman [23] and others [24] have described ecological momentary assessment (EMA) in which data of interest are recorded frequently, in real time, and in the critical environment. Johnston et al. [25] used EMA methods to study the success of the demand control and effort reward imbalance models in explaining variations in self-rated stress in a pilot study of nurses. They developed a personal digital assistant (PDA)-based method which assessed affect and the main constructs from the demand control and effort reward imbalance models and tested it on a small sample of nurses measured frequently over three nursing shifts. They obtained preliminary information which suggested that such measurement was acceptable and that variations in a one item rating of self-reported stress did relate as predicted to the occurrence of high demand and low control and high effort and low reward. We build on Johnston et al. [25] by examining a larger group of nurse participants, assessed frequently over three work shifts using more comprehensive measurement of stress-related affect. It is clear from many reviews [11, 12] that the processes identified by the demand control and effort reward imbalance models are associated with negative emotional outcomes and so related transitory states are likely to be associated with negative affect. It is less clear (and seldom examined) if these processes predict positive affect.
This report is concerned with the associations, within nurses, between their perception of their work situation and stress-related affect. We examine: (1) whether periods of high demand and effort are associated with higher negative affect (NA), (2) if periods of high control and reward are associated with lower NA and (3) if control and reward moderate the effects of demand/effort on NA such that the greatest NA is experienced when demand or effort is high and control or reward low. The relationship between the same predictors and positive affect (PA) are examined to establish if the determinants of NA also relate to PA.
Methods
Design and Procedure
This study employed a within and between subject design incorporating both cross-sectional and longitudinal elements. Levels of negative and positive affect at work, and the putative determinants of stress that influence affect were assessed in nurses in four large English hospitals. Nurses, selected at random from lists provided by the Human Resources Department, were contacted by letter and returned consent forms to locally agreed collection points. Packs of questionnaires were then sent to consenting nurses and dates agreed for the completion of the PDA diaries. PDAs were delivered by research assistant to the participant’s ward and demonstrated prior to the first shift on which diaries were to be completed. The PDAs were programmed to run for the next three shifts and were returned to the research assistant upon completion. The study was approved by the North West Manchester Research Ethics Committee (06/MRE08/35), and by the appropriate NHS R&D authorities for each of the four participating NHS Trusts.
Participants
We tested 254 nurses from medical and surgical wards in each of the four hospitals. Two of the hospitals provided 75 nurses, one 69 and one 35. All qualified nurses working at least 22 h per week on medical and surgical wards were eligible. All shift patterns were accepted. Approximately 16 % of the nurses approached volunteered. EMA diaries were obtained from 254 nurses and 233 of these completed baseline questionnaires and provided basic demographic details. To check that the sample was representative we compared it with the total work force in three of the four hospitals we studied (the figures were not available for the fourth) on nursing grade, gender and type of ward. The distribution of nursing grades and the split between medical and surgical wards were very similar but men were slightly over represented in the sample tested at 14.6 % compared to 9.4 % in the population that we sampled from.
Materials
Nurses completed baseline questionnaire measures including the Positive and Negative Affect Scale (PANAS) [26] followed by PDA measures obtained frequently over three nursing shifts.
The format for the diary questions was very similar to that used by Johnston et al. [25]. It was operationalised using specially written software on Dell Axim 50 PDAs. In addition to EMA, nurses used the PDA to record critical incidents and end of shift ratings [27]. Data entry on the PDA was prompted by an auditory alarm that occurred throughout the shift at approximately 90-min intervals (with a window of ±15 min determined randomly by the program). There were therefore usually between six and nine diary entries per shift, depending on shift length. All ratings were done on analogue scales and the participants indicated their state by tapping with a stylus at the appropriate point on the scale. Participants rated their mood at that moment on nine scales measuring how alert, tired, happy, stressed, angry, energetic, sad, frustrated and nervous they were (see the Electronic Supplementary Material (ESM), Appendix 1, for examples of the PDA displays). The mood adjectives were taken from Kamarck et al. [28] and have been used extensively in real-time studies [29]. Following factor analysis (see “Data Analysis” section) NA was assessed by averaging stressed, angry, sad, frustrated and nervous and PA by averaging alert, happy and energetic. Further questions were mapped on the constructs central to the demand control and effort reward imbalance models, i.e. demand/effort, control and reward. Demand/effort was assessed by asking how hard and how fast participants had worked over the previous 10 min. The two scales, which correlated 0.77, were averaged. There is considerable overlap between the concepts of ‘demand’ and ‘effort’ in how they are usually measured. They were therefore treated as a single construct in the diary, in order to reduce measurement burden and confusion among the participants. Single scales were used to measure control (“control over work”) and reward which was as operationalised as “work has been appreciated”.
Data Analysis
The nine mood scales were factor analysed to improve the reliability of the mood measures and reduce the risk of chance findings achieving significance if all nine scales were analysed separately. A principal components analysis followed by varimax rotation of the average scores for each participant on the nine affect scales showed there to be two clear factors with Eigenvalues of 4.3 and 1.6. The first factor represented negative affect (NA), and consisted of the following adjectives (factor loadings in brackets); stressed (0.78), angry (0.86), sad (0.80), frustrated (0.83) and nervous (0.76) and factor 2 captured positive affect (PA) and consisted of alert (0.78), happy (0.77) and energetic (0.90). The scale “tired” loaded moderately on both factors (0.39, −48) and was not included in the factors. Stone et al. [30] also classified similar mood scales used in a form of real-time measurement into NA, PA and a single-item measure of tiredness.
To confirm the applicability of the factor analysis at the level of an individual entry, the data were analysed for separate occasions of measurement. There was sufficient data for analysis from the first six measurements on each of the three shifts. The same factor structure was seen across the 18 factor analyses with factor 1 representing NA and factor 2 PA. On the individual measurement occasions, Cronbach alphas for NA ranged between .74 and .87 with a median of .81. For PA alpha varied between .61 and .76 with a median value of .70. The validity of such EMA measurement does not depend on it relating closely to questionnaire equivalents but some degree of positive relationship might be expected. The PANAS [26] questionnaire measures of NA and PA were related to their EMA equivalent using multilevel modelling in models with three levels, participant, shift and time within shift (see below). The intercept was random at all levels. The scores were standardised to indicate the size of the relationships more clearly. NA assessed by questionnaire related positively to the EMA measure (β = .313, SE = .046 p < .001) as did PA (β = .288, SE = .044, p < .001).
The main analyses were conducted using MLwiN V 2.18 and V 2.22. Statistical testing was based on multilevel linear modelling [31]. We tested three-level models in which the EMA measures at each observation (level 1) were nested within shifts (level 2) which were nested within participants (level 3). The level 1 variables were diary captured demand/effort, reward, control, NA, PA, shift and the time into the shift when the measure was taken, with the start of the shift taken as zero time. The PDA software converted the analogue values to scores between 0 and 100 and following Johnston et al. [25] the diary scores for demand/effort, control and reward were rescaled into 1–5 when used as predictor variables. This led to more interpretable regression models.
The demand control and effort reward imbalance models were examined in an analysis with two main effects (demand/effort and either control or reward) and interaction terms representing demand/effort by control and demand/effort by reward. The main dependent variables were NA and PA; in addition the models were tested on the five individual items making up the NA scale, see ESM Appendix 2. The intercept was always treated as a random effect at all levels. The regression slopes of the relationship between main predictor variables and the outcome (NA or PA) were allowed to vary randomly between participants, i.e. the degree and direction of relationship between predictor and outcome was not required to be the same in all participants. To illustrate this, plots were obtained of the individual regression lines for each participant predicting the outcome from selected predictors. This standard procedure is described by Hox [30], page 28–30 and is available in MLwiN, [32], page 57–67. The control variables of shift and time into shift were treated as fixed. The predictor variables were centred within participants since we were primarily interested in the relationships within an individual over the period of real-time measurement. Most of the repeatedly measured data was moderately autocorrelated. A multilevel model including autocorrelation between occasion level residuals was used, as described by Rasbash et al. [33]. The alpha level was set at p < .01 with Bonferroni correction.
Results
Demographic details of participants are shown in Table 1. Their average age was 39.1 (range 21–62 years). Over the three shifts 5,522 diary entries were requested and 4,475 completed (a missing entry rate of 18.9 %). Removal of obvious errors, such as when all ratings for an entry were set to 0 or end of shift entries completed at the start of the next shift, reduced this to 4,259 regular diary entries. The correction for time series effects requires complete data at each time point and this reduced the final number of observations to 4,237 from 254 participants across the three shifts, an average of 16.8 entries per participant (range 1 to 29). Missing data were not imputed. Thirty-two participants provide data for only two shifts and 10 for only one; all were included in the analyses. The average values for the sample including overall and within subject standard deviations, bivariate correlations and intraclass correlations are shown in Table 2.
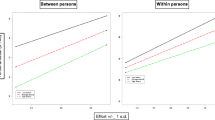
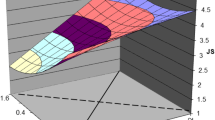
The demand control model was examined in a model that included shift, time into shift and demand/effort, control and the demand/effort by control interaction, see Table 3. The fixed effects show that NA increased as demand/effort increased, diminished as control increased and the demand/effort by control interaction was significant. A simple slopes plot is shown in Fig. 1a. As predicted, control moderated the effect of demand/effort. The consistency of all the effects in this model was very high with the estimates suggesting that the model applies to over 90 % of nurses. The variance estimates show that the slopes for demand/effort and control varied reliably between participants. This is illustrated in Fig. 2a in which the individual regression slopes of NA on demand/effort are shown; for clarity the intercept was fixed for this plot. It can be seen that demand/effort was associated with much greater increases in NA in some participants than others but in virtually all participants the slope was positive. Demand/effort was associated with an increase in PA, as was control. Control did not moderate the effects of demand/effort on PA.

a, b Plots of the interactions between the predictors on negative affect. a demand/effort by control, b demand/effort by reward

a, b Plots of individual regression slopes of negative affect on predictor variables. a Negative affect on demand/effort. b Negative affect on interaction of demand/effort and reward
The results of modelling the effort reward imbalance model are shown in Table 4. Reward was related to decreased NA and moderated the effect of demand/effort on NA as predicted (see Fig. 1b) for simple effects plot), although the effect was not very consistent as it was estimated that over 30 % of nurses do not show it. The individual regression slopes of this interaction are shown in Fig. 2b. This interaction has a negative slope (see the fixed effects details in Table 4) but some participants showed markedly different relationships to the sample as a whole. While most individual slopes are negative, the positive slopes suggest that in a few individuals high reward in combination with high demand/effort produced the greatest NA. Reward was associated with increased PA and did not moderate the effect of demand/effort on PA
Discussion
In a sample of nurses measured frequently over three work shifts, PDA-based EMA methods were able to assess work-related affect and its putative determinants. In within participant analysis a summary measure of NA related positively to demand/effort, negatively to control and control moderated the effects of demand/effort. PA related positively to demand/effort and control. Periods of increased perceived reward were associated with less NA and greater PA and reward moderated the effects of demand/effort on NA.
The primary aim of this report was to determine if the processes known to predict the differences between people in work-related stress also operate within people, nurses in this case. It appears that they do. Models of occupation stress are primarily concerned with the negative effects of the work situation and make the clearest predictions for negative emotions. Within the nurses in this study NA was related as predicted to factors identified by leading theorists as critical. NA was highest at periods of high demand/effort, low control and low reward. As well as specifying the factors thought to determine stress both Karasek and Siegrist [7, 8] specify the relationship between these factors with control moderating the effect of demand (Karasek) and reward moderating the effect of effort (Siegrist). Both effects were seen in relation to NA which was at its highest when demand/effort was high and control or reward low. This is a very powerful demonstration that the models of occupational stress that have been applied between people also apply within individuals over the working day. This finding also confirms the results of an earlier much smaller and more limited study [25]. Neither control nor reward moderated the effects of demand/effort on PA. Interestingly, and unexpectedly, demand/effort was associated positively with PA. This indicates that demand/effort has both good and bad aspects since it is associated with high negative and positive affect in the majority of nurses.
The demonstration that the same relationships hold within individuals as between them is of importance. The results of the fixed effects aspects analysis suggest that the relationships obtained are not trivial. Of equal importance to the size of these effects is the consistency of these relationships. Both theoretically and practically it is important to know if these relationships are found in most nurses. The estimates of the percentage of the sample showing the predicted relationships suggest that most of the effects occur in at least 80 % of nurses. The consistency of the expected relationships was particularly strong for the factors examined in the tests of the demand control model with NA. When the moderating effects of control are allowed for the positive effect of demand/effort, the negative effect of control and its moderating effect were all seen in over 90 % of nurses. This is a very powerful demonstration of the applicability of the demand control model within individuals. The effort reward imbalance model did not fit the data so consistently, with the expected moderating effect of reward being seen in less than 70 %. However, we caution against a premature decision that the effort reward imbalance model is less applicable within nurses. We asked participants to rate how “appreciated” they felt and while this captures aspects of reward it is unlikely to encompass the complete concept, many aspects of which do not vary over short time periods. Moreover, reward was a strong, consistent predictor of PA and so is clearly not a trivial variable. We think it best to interpret these findings as showing that perceptions of reward are important correlates of affect within people and that reward is worthy of further study.
While the model fit was good within most individuals, the degree of relationships varied between people and a minority of participants did not show the expected effects. This is important both theoretically and practically. Theoretically, one needs to know why some individuals show counter theoretical relationships. Why, for example, do some people in conditions of high demand/effort report more NA when they perceive that they are being rewarded more? This could relate to aspects of their personality (are they cynical individuals for example) or it could relate to the particular circumstances that led to the reward, perhaps an obviously distressed nurse elicits appreciative (rewarded) behaviour from a patient or colleague. These are questions for future research on the personal and situational factors that moderate the relationships shown in this study. The practical implication is that while it may be of benefit to many if nursing could be made less demanding or the nurse provided with more reward, a significant few might not benefit and may even be disadvantaged.
We consider that the diaries were practical. EMA measurement is a compromise between coverage of the areas of interest, psychometric soundness and practicality. The average time for EMA diary entries was under 50 s so little time was spent on this aspect of the diaries. Systematic data was obtained that interrelated as predicted. Data completion rates were high with over 80 % of entries completed. This is impressive if one recalls that the participants were nurses working on busy medical and surgical wards. Rutledge et al. [29] report a similar figure in an EMA study of a mixed group of physicians and nurses. There was substantial variation between hospitals in completion rates with the highest being over 90 % while the lowest was just over 70 %. It is not possible to determine the cause of this variation since the staff running the study varied between hospitals and the hospitals differed in their characteristics. It is our impression that completion rates are higher when, unremarkably, the researcher administering the PDA emphasises the importance of attempting to complete all entries but differences in organisation climate between hospitals are also likely to be important. We consider that this study has many positive features including the substantial sample of nurses of all grades assessed over many measurement occasions in the work environment and the high completion rate. The obvious limitation is that predictor and outcome were measured at the same time using one instrument. Clearly, one cannot draw causal conclusions from this study. However, the detailed pattern of the results, the support for the theoretical predictions, particularly the support for the moderating effects of control and reward, and the different results with different outcome measures strongly suggest that the findings are not primarily due to common method variance. In addition we have shown in this sample that serious incidents (identified by the participant at the end of the shift) were associated with a subsequent increase in NA [27]. Future work should attempt to obtain separate, ideally objective, measures of the work situation and the participants’ stress-related responses. The low rate of volunteering for the study, 16 %, is also a concern. The nature of the sample can powerfully affect how well mean values generalise to the true population but has a smaller effect on the interrelationship between measures which is, of course, the focus of this study. Nevertheless in future studies it would be very helpful if EMA measurement could be made attractive to more nurses.
References
Williams S, Michie S, Pattani S. Improving the Health of the NHS Workforces: Report of the Partnership on the Health of the NHS Workforce. London: The Nuffield Trust; 1998.
Estryn-Behar M, Van Der Heijden BIJM, Oginska H, et al. The impact of social work environment, teamwork characteristics, burnout, and personal factors on intent to leave among European nurses. Medical Care. 2007;45:939-950.
Coomber B, Barriball KL. Impact of job satisfaction components on intent to leave and turnover for hospital-based nurses: A review of the research literature. Int J Nurs Studies. 2007;44:297-314.
Aiken L, Clarke S, Sloane D, Sochalski J, Silber J. Hospital nurse staffing and patient mortality, nurse burnout and job dissatisfaction. JAMA. 2002;288:1987-1993.
Fogarty GJ, McKeon CM. Patient safety during medication administration: The influence of organizational and individual variables on unsafe work practices and medication errors. Ergonomics. 2006;49:444-456.
Elfering A, Semmer NK, Grebner S. Work stress and patient safety: Observer-rated work stressors predictors of characteristics of safety-related events reported by young nurses. Ergonomics. 2006;49:457-469.
Karasek RA. Job demands, job decision latitude, and mental strain: Implications for job redesign. Admin Sci Quarterly. 1979;24:285-307.
Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occ Health Psychol. 1996;1:27-41.
Johnson JV, Hall EM. Job strain, work place social support, and cardiovascular disease: A cross-sectional study of a random sample of the Swedish working population. Am J Public Health. 1988;78:1336-42.
van der Doef M, Maes S. The job demand-control (−support) model and physical health outcomes: A review of the strain and buffer hypotheses. Psychol Health. 1998;13:909-936.
van der Doef M, Maes S. The job demand-control (−support) model and psychological well-being: A review of 20 years of empirical research. Work & Stress. 1999;13:87-114.
van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: Drawing up the balance of 45 empirical studies. Soc Sci Med. 2005;60:1117-1131.
Cheng Y, Kawachi I, Coakley EH, Schwartz J, Colditz G. Association between psychosocial work characteristics and health functioning in American women: Prospective study. BMJ. 2000;320:1432-1436.
Verhaeghe R, Mak R, Van Maele G, Kornitzer M, De Backer G. Job stress among middle-aged health care workers and its relation to sickness absence. Stress Health. 2003;19:265-274.
Escriba-Aguir V, Perez-Hoyos S. Psychological well-being and psychosocial work environment characteristics among emergency medical and nursing staff. Stress Health. 2007;23:153-160.
Weyers S, Peter R, Boggild H, Jeppensen HJ,Siegrist J 2006 Psychosocial work stress is associated with poor self rated health in Danish nurses: A test of the effort-reward imbalance model. Scan J Caring Sci 20:26–34.
Lavoie-Tremblay M, O’Brien-Pallas L, Gelinas C, Desforges N, Marchionni C. Addressing the turnover issue among new nurses from a generational viewpoint. J Nurs Man. 2008;16:724-733.
Bakker AB, Killmer CH, Siegrist J, Schaufeli WB. Effort-reward imbalance and burnout among nurses. J Adv Nurs. 2000;31:884-891.
Spence Laschinger HK, Finegan J. Situational and dispositional predictors of nurse manager burnout: A time lagged analysis. J Nurs Man. 2008;16:601-607.
Aboa-Éboule C, Brisson C, Blanchette C, et al. GR. Effort-Reward Imbalance at work and psychological distress: A validation study of post-myocardial infarction patients. Psychosom Med. 2011;73:448-45.
Hausser JA, Mojzisch A, Niesel M, Schulz-Hardt S. Ten years on: A review of recent research on the Job Demand–Control (−Support) model and psychological well-being. Work & Stress. 2010;24:1-35.
Molenaar PCM. A manifesto on psychology as idiographic science: Bringing the person back into scientific psychology, this time forever. Measurement. 2004;2:201-218.
Stone AA, Shiffman S. Ecological momentary assessment (EMA) in behavioral medicine. Ann Behav Med. 1994;16:199-202.
Bolger N, Davis A, Rafaeli E. Diary methods: Capturing life as it is lived. Ann Rev Psychol. 2003;54:579-616.
Johnston DW, Beedie A, Jones MC. Using computerised ambulatory diaries for the assessment of job characteristics and work-related stress in nurses. Work & Stress. 2006;20:163-172.
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Per Soc Psychol. 1988;54:1063-1070.
Jones MC, Johnston DW. Does clinical incident seriousness and receipt of work-based support influence mood experienced by nurses at work? A behavioural diary study. Int J Nurs Studies. 2012;48:978-987.
Kamarck TW, Shiffman SM, Smithline L, et al. The diary of ambulatory behavioral states: A new approach to the assessment of psychosocial influences on ambulatory cardiovascular activity. In D, Krantz & A., Baum (eds.) Technology & Methodology in Behavioral Medicine. Hillsdale. NJ: Laurence Erlbaum. 1998;1988:163-193.
Rutledge T, Stucky E, Dollarhide A, et al. A real-time assessment of work stress in physicians and nurses. Health Psychol. 2009;2009(28):194-200.
Stone AA, Schwarz JE, Schkade D, Schwarz N, Kreuger AB, Kahneman D. A population approach to the study of emotion: Diurnal rhythms of a working day examined with the Day Reconstruction method. Emotion. 2006;6:139-149.
Hox J. Multilevel Analysis: Techniques and applications. 2nd ed. Hove: Routledge; 2010.
Rasbash JR, Steele F, Browne W, Prosser B. A user’s guide to MLwiN version 2.0. Centre for Multilevel Modelling. London: University of London; 2004.
Rasbash JR, Charlton CMJ, Jones K, Pillinger RJ. Manual Supplement for MLwiN Version 2.10, Centre for Multilevel Modelling. Bristol: University of Bristol; 2009.
Conflict of Interests Statement
The authors have no conflicts of interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article presents independent research commissioned by the National Institute for Health Research (NIHR) Service Delivery and Organisation (SDO) Programme. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The NIHR SDO Programme is funded by the Department of Health. This research was supported by SDO grant SDO/92/05, lead investigator L. McKee. The late Jon Rasbash provided us with very important advice on the conduct and reporting of the analyses in this paper and was as always a source of help and encouragement. We thank Marie Johnston for her helpful comments on drafts of this paper. Correspondence regarding this article should be addressed to Professor Derek Johnston, School of Psychology, University of Aberdeen, Kings College, Aberdeen, AB24 3FX, Scotland.
About this article
Cite this article
Johnston, D.W., Jones, M.C., Charles, K. et al. Stress in Nurses: Stress-Related Affect and Its Determinants Examined Over the Nursing Day. ann. behav. med. 45, 348–356 (2013). https://doi.org/10.1007/s12160-012-9458-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-012-9458-2