
Abstract
Objectives
Radioiodine therapy is an effective treatment for lung metastasis from thyroid cancer. However, cases of lung metastasis without iodine uptake are often encountered. In such cases, FDG accumulation in lung lesions is often observed. There is a reverse relationship between iodine and FDG accumulation in thyroid cancer lesions, the so-called “flip-flop” phenomenon. The aim of this study was to assess the relationship between patient age and the occurrence of the flip-flop phenomenon.
Methods
Eighty-six patients who underwent radioiodine therapy for lung metastasis were studied retrospectively (age 17–73 years; median 60 years; males:females 22:64). We compared the clinical data and imaging findings (size and FDG uptake of lung nodules) between patients with (n = 44) and without (n = 42) iodine uptake in lung metastasis.
Results
Significantly more young patients showed iodine accumulation in lung metastasis than old patients (p = 0.0025). Lung metastases with larger size or greater FDG uptake showed no iodine uptake more frequently with significant difference (p = 0.015 and <0.001, respectively). Among patients with FDG uptake in the lung metastasis, 57.1 % of young patients (<60 years) and 24.3 % of the old patients (≥60 years) showed iodine uptake (p = 0.0029).
Conclusions
Higher patient age and lung nodules with large size or FDG accumulation are negative factors for iodine accumulation in lung metastases from thyroid cancer. In addition, our results show that young patients have a greater likelihood of iodine uptake even when FDG accumulates in lung metastasis, in contrast to old patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Radioiodine therapy (RIT) is used for the purpose of thyroid bed ablation and treatment of metastatic lesions in patients with differentiated thyroid cancer (DTC) [1–3]. RIT reduces the cancer-specific mortality, recurrence rate and progression rate in DTC patients [4, 5]. RIT is effective only when radioiodine accumulates in the lesions, but we often encounter patients without iodine uptake in their thyroid cancer lesions.
After cervical lymph nodes, the lung is the most frequent site of metastasis from thyroid cancer [6–8]. Judging whether lung lesions are likely to accumulate radioiodine is very important to avoid performing RIT for patients who will not benefit from it.
A study that analyzed prognostic factors in patients with distant metastasis from DTC showed that extensive metastases, older age at the diagnosis of the metastases, the absence of iodine uptake by metastases, and moderately differentiated follicular cell type were of independent prognostic significance for survival [9].
Two-[F-18]-fluorodeoxyglucose positron emission tomography (FDG-PET) has expanded rapidly and is used for the evaluation of many types of malignant tumor. The role of FDG-PET or FDG-PET/computed tomography (CT) is to detect iodine-131-negative lesions in DTC patients, particularly those with a high thyroglobulin (Tg) level but without iodine uptake [10–14].
There is a reverse relationship between iodine and FDG accumulation in thyroid cancer lesions, the so-called “flip-flop” phenomenon [15]. This phenomenon has been explained in connection with the dedifferentiation of cancer cells [15].
Patient age affects the outcome of RIT for thyroid cancer; therefore, we thought that the flip-flop phenomenon might be influenced by patient age. In this study, we compared the clinical data including patient age and image findings (size and FDG uptake of lung metastasis) between patients with and without iodine uptake in lung metastasis, and also assessed the difference in the flip-flop phenomenon as related to patient age.
Materials and methods
Patients
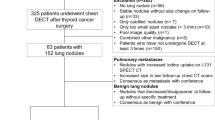
This retrospective study was approved by the review board of our institution, and the requirement of written informed consent was waived. We enrolled a total of 86 DTC patients (78 papillary carcinomas, 7 follicular carcinomas and 1 papillary and follicular carcinoma) who received their first session of RIT against DTC between October 2007 and June 2014, underwent FDG-PET/CT and were diagnosed as having lung metastasis from thyroid cancer using the following criteria: (1) pathological diagnosis, (2) iodine uptake in the lung lesions, (3) interval increase in either the size or number of pulmonary nodules, and (4) combination of multiple lung nodules [>10] and either elevated Tg [>50 ng/mL] or elevated anti-Tg antibody [>300 IU/mL]. The patients’ ages ranged from 17 to 73 years (median 60 years). All patients underwent complete thyroid hormone withdrawal for 4 weeks before RIT for the purpose of TSH elevation, and all patients were given a low-iodine diet for 2 weeks in preparation for iodine-131 administration (Sodium iodide I-131 Capsule; Fujifilm RI Pharma, Tokyo). The median serum TSH level of our patients just before the iodine-131 administration was 97.2 μU/mL, with a range of 2.44–487.1 μU/mL. The four patients with very low TSH levels (TSH 2.53–8.85 ng/mL, free T3 2.80–3.62 ng/dL, free T4 0.73–0.99 pg/mL) were clinically diagnosed as having hormone-producing tumors and showed pulmonary iodine uptake. The administered dose of iodine-131 ranged from 3.07 to 6.05 GBq (median 4.45 GBq), determined on the basis of clinical data such as the extent of disease progression, the patient’s age, and the patient’s weight, but not the results of pretherapeutic diagnostic scintigraphy.
I-131 scintigraphy
Post-therapy imaging was performed 5–7 days after the iodine-131 administration. Whole-body scintigraphy was performed using a dual-head gamma camera (Symbia T6, Siemens Healthcare, Malvern, PA, or GCA901A/WB, Toshiba Medical Systems, Tokyo) with high-energy collimators. Single-photon emission computed tomography (SPECT)/CT images were obtained with a gamma camera with a six-section spiral CT within the same gantry after the Symbia T6 was installed and used for the iodine-131 scintigraphy. SPECT/CT scans from the neck to the chest were obtained. CT-based attenuation correction and no scattering correction were applied to the SPECT images. SPECT/CT images were used only for the presentation of the representative cases (Figs. 1, 2, 3).

A whole-body scan for iodine-131 (a), CT (b), SPECT/CT (c), and FDG-PET/CT (d) images in a 26-year-old man at his first RIT session. The whole-body scan for iodine-131 showed diffuse uptake in the bilateral lung fields and focal strong uptake in the right lower lung field. The greatest dia. of the largest lung nodule was <5 mm. SPECT/CT showed strong iodine uptake in the lung nodule but no FDG uptake

A whole-body scan for iodine-131 (a), CT (b), SPECT/CT (c), and FDG-PET/CT (d) images in a 55-year-old man at his first RIT session. The whole-body scan for iodine-131 showed no uptake in bilateral lung fields. The greatest dia. of the largest lung nodule was >1 cm. No iodine uptake on SPECT/CT but strong FDG uptake on FDG-PET was found in the nodule

A whole-body scan for iodine-131 (a), FDG-PET MIP (Maximum Intensity Projection) (b), SPECT/CT (c), and FDG-PET/CT (d) images in a 57-year-old woman at her first RIT session. The whole-body scan for iodine-131 and FDG-PET MIP image both showed uptake in bilateral lung. Iodine-131 and FDG uptake in the lung nodules were detected on the fusion images of SPECT/CT and PET/CT
Diagnostic CT protocol
The diagnostic neck and chest CT, covering the region from the skull base to the upper mediastinum, was performed with a 64-multidetector-row computed tomography (MDCT) scanner (Aquilion 64; Toshiba Medical Systems) after I-131 scintigraphy, using the following parameters: tube voltage 120 kV, effective tube current 300 mA, collimation 0.5 mm, and pitch 27.0. Each patient received 100 mL of intravenous nonionic contrast material containing 300 mg I/mL [Iopamiron 300 (Iopamidol) from Bayer Schering Pharma, Osaka, Japan or Omnipaque 300 (Iohexol) from Daiichi-Sankyo Pharmaceuticals, Tokyo] at a flow rate of 1.5 mL/s, and scanning was started 80 s after the start of contrast injection. Non-contrast-enhanced CT was performed on four patients because of iodine allergy or renal dysfunction. The MDCT scan was reconstructed by filtered back projection into 512 × 512 pixel images with a slice thickness of 5 mm.
FDG-PET/CT
All patients underwent FDG-PET/CT at the first session of RIT for metastasis screening. FDG-PET/CT acquisition was performed under the TSH-stimulated state. In each patient, 185 MBq of FDG was intravenously administered after fasting for at least 4 h. Scans were conducted from the middle of the thigh to the top of the skull 60 min after the FDG administration. FDG-PET/CT images were obtained using an integrated PET/CT scanner, the Discovery STE (GE Medical Systems, Milwaukee, WI) or Biograph mCT (Siemens Medical Solutions, Erlangen, Germany). All emission scans were performed in the three-dimensional mode, and the acquisition time per bed position was 3 min for the Discovery STE and 2 min for the Biograph mCT.
We reconstructed the PET images using the ordered-subset expectation–maximization method (VUE Point Plus) with two full iterations of 28 subsets for the Discovery STE and iterative True-X algorithm and TOF (Ultra HD-PET) with two full iterations of 21 subsets. The True-X algorithm incorporates an additional specific correction for the point-spread function. The full-width at half maximum values of the Discovery STE and Biograph mCT were 5.2 and 4.4 mm, respectively. A low-dose 16-slice CT (tube voltage, 120 kV; effective tube current, 30–250 mA, Discovery STE) and a low-dose 32-slice CT (tube voltage. 120 kV; the use of angular and longitudinal dose modulation, CAREDose4D®, Biograph mCT) from the vertex to the proximal thigh were performed for attenuation correction, and for determining the precise anatomic location of the lesions before acquisition of the PET image. The CT scan was reconstructed by filtered back projection into 512 × 512 pixel images with a slice thickness of 5 mm to match the PET scan. The FDG-PET/CT, diagnostic CT, and iodine-131 scintigraphy were performed within 5 days of each other.
Analysis
The clinical data (age, sex, Tg level, and initial or recurrent disease) and the image findings (size and FDG uptake of lung nodules) were compared between the patients with and without iodine uptake in their lung metastases. The patients with high anti-Tg antibody were excluded from the analysis of Tg.
In this study, the patients with recurrent disease were those diagnosed with lung metastasis more than 1 year after surgery for thyroid cancer. The patients with higher iodine uptake in the lung compared to the mediastinum and the patients with higher FDG uptake in lung nodules than in the background were defined as positive for iodine and FDG uptake, respectively.
For the analysis of lung nodule size, the greatest diameter of the largest nodule was measured and classified into the following three groups: (1) dia. <5 mm; (2) dia. 5 mm to <1 cm; (3) dia. ≥1 cm.
Statistics
Statistical analyses were performed using JMP 11 software (SAS Institute, Cary, SC). The Wilcoxon rank sum test and Chi-square test were performed to analyze the differences between cases with and without iodine uptake in lung metastasis.
Results
Forty-four of the 86 patients (51.2 %) with lung metastasis showed iodine uptake in the lung. There was no significant difference in TSH level between the patients with and without iodine uptake in the lung, both including and not including the four patients with hormone-producing tumors (data not shown).
The patients in the group without iodine uptake in lung metastasis (n = 42, 48.8 %) were significantly older than those with iodine uptake (n = 44, 51.2 %; p = 0.0005, Table 1). Only 15 of the 46 patients (32.6 %) aged 60 years or older showed iodine uptake in the lung metastasis, whereas 29 of the 40 younger patients (72.5 %) did (Table 2).
Male patients (9 of 22 patients, 40.9 %) and patients with recurrent disease (16 of 34 patients, 47.1 %) showed pulmonary iodine uptake less frequently compared to the female patients (35 of 64 patients, 54.7 %) and patients at their initial diagnosis (28 of the 52 patients, 53.8 %) although these differences were not statistically significant (p = 0.20 and p = 0.54, respectively, Table 1). The median Tg level in patients without pulmonary iodine uptake (230 ng/mL) was less than those with the uptake (401.5 ng/mL); however, there was no significant difference in Tg level between these two groups (p = 0.36, Table 1).
For the analysis of lung nodule size, we classified the patients into three groups depending on the size of the largest lung nodule. The patients with larger nodules were significantly less likely to show iodine uptake (p = 0.015, Table 3; Figs. 1, 2). In addition, we investigated the relationship between FDG uptake and iodine uptake in the lung lesions. The patients with FDG uptake in the lung lesions were significantly more likely to have no iodine uptake in the lung metastasis (p < 0.0001, Table 3; Figs. 1, 2).
The patients were divided into two groups depending on their age to assess the relationship between the flip-flop phenomenon and patient age. The cutoff age was set at 60 years because the possibility of pulmonary iodine uptake became less than 50 % when the patients were 60 years or older (Table 2). Among patients with FDG uptake in the lung metastasis, 57.1 % of the young patients (<60 years) showed iodine uptake while only 24.3 % of the old patients (<60 years) did (p = 0.029, Table 4). There was no significant difference in the possibility of pulmonary iodine uptake between young and old patients when FDG did not accumulate in lung metastasis (p = 0.40, Table 4).
Discussion
In the present study, the relationship between patient age and iodine uptake in lung metastasis was analyzed in detail. Twenty-nine of 40 young patients under 60 years of age (62.5 %) showed iodine uptake in lung metastasis, in contrast to only 15 of 46 patients who were 60 years old or older (32.6 %). Furthermore, 15 of 19 patients under 50 years of age (78.9 %) showed pulmonary iodine uptake while only 2 of 11 patients who were 70 years old or older (18.2 %) did. Our results showed a significant correlation between patient age and iodine uptake in lung metastases, which strongly coincides with the finding that older DTC patients with distant metastases have worse prognoses [7, 9, 16, 17].
In the present study, there was no significant difference in pulmonary iodine uptake between male and female patients, consistent with previous reports showing no significant relationship between prognosis and gender [7, 9, 18]. The previous report analyzing thyroid cancer of children showed a better prognosis in patients whose distant metastasis was already detected when their thyroid cancer was diagnosed [19]. On the other hand, no such difference was found in a previous study on adult patients with thyroid cancer [7]. Our result showed no significant difference depending on the timing of lung metastasis onset, consistent with the previous study on adult patients.
The level of Tg is related to the amount and activity of normal thyroidal or thyroid cancer cells, and the Tg level increases noticeably when TSH stimulation is performed at the RIT [20]. Our study showed a higher Tg level in patients with pulmonary iodine uptake compared to those without it though the difference was not statistically significant. The production of Tg is low in patients with poorly differentiated thyroid cancer and absent in those with anaplastic thyroid cancer [20]. Our results might indicate a relationship between the absence of iodine uptake in lung lesions and the dedifferentiation of thyroid cancers.
The size of the largest lung metastasis was negatively correlated with iodine uptake in the lung metastases of the present patient population. The size of the largest lung metastasis is probably correlated with either the period from the occurrence of metastasis or the growth speed. It was reported that macroscopic lung metastasis has a relationship with poor prognosis [9]. In that study, the size of lung metastasis was analyzed on a chest X-ray, and was >1 cm dia. Lung nodules were associated with a poor prognosis. Here, we examined the size of lung nodules on CT in greater detail, and the results suggested that simply measuring the greatest diameter of the largest lung nodule enables the prediction of iodine accumulation in lung metastasis.
In our study, only 33.3 % of the patients with FDG-avid pulmonary lesions had iodine uptake in the pulmonary lesions, whereas 77.1 % of the patients with non-FDG-avid pulmonary lesions had iodine uptake. This result is consistent with the so-called “flip-flop phenomenon,” which means that thyroid cancer lesions tend to not accumulate iodine if they are FDG-avid [15]. This phenomenon can be explained by the findings of a previous report in which glucose transporter 1 (GLUT-1) expression was observed in sodium iodine symporter (NIS)-negative specimens, and NIS was expressed in most GLUT-1-negative specimens [21].
The old patients were less likely to accumulate iodine in lung metastasis when their lesions showed FDG uptake (9 of 37 patients, 24.3 %). However, more than a half of the young patients with FDG uptake in lung metastasis also showed iodine uptake (8 of 14 patients, 57.1 %). FDG accumulation generally indicates dedifferentiation of thyroid cancer and decreased NIS expression. Thyroid cancer is a unique malignancy because age is a key indicator of its prognosis, although the reason for the relationship between age and prognosis has not yet been fully defined [22]. Juvenile thyroid cancer has some differences with adult thyroid cancer including a high NIS expression close to normal thyroidal tissue [23]. This evidence suggests that the lung metastases of young patients possess a high NIS expression, which is sufficient to show iodine uptake even when they somewhat dedifferentiate. Our results indicate that the FDG-avidity of lung metastasis from thyroid cancer does not have the same implications for patients of different ages.
One of the limitations is that this is a retrospective study, although the consecutive patients who underwent FDG-PET and RIT for DTC with lung metastasis were included. Most lung metastases were diagnosed clinically. The lesion-based analysis could be more informative to assess the flip-flop phenomenon. However, it was difficult to perform lesion-based analysis for several reasons including the fusion of iodine/FDG uptake, misregistration of iodine/FDG uptake in lung nodules and the large difference in the number of lung nodules among the cases.
Conclusion
Our results show that higher patient age, larger size of lung nodules, and FDG-avid lung nodules are related to a lack of iodine uptake in the lung metastasis of patients with differentiated thyroid cancer. There is an age difference in the iodine/FDG “flip-flop” phenomenon of lung metastasis from thyroid cancer; among patients whose lung lesions are FDG-avid, young patients still have a good chance of pulmonary iodine uptake while the chances of old patients are much lower.
References
Robbins RJ, Schlumberger MJ. The evolving role of (131)I for the treatment of differentiated thyroid carcinoma. J Nucl Med. 2005;46(Suppl 1):28S–37S.
Luster M, Clarke SE, Dietlein M, Lassmann M, Lind P, Oyen WJ, et al. Guidelines for radioiodine therapy of differentiated thyroid cancer. Eur J Nucl Med Mol Imaging. 2008;35:1941–59.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Tsang RW, Brierley JD, Simpson WJ, Panzarella T, Gospodarowicz MK, Sutcliffe SB. The effects of surgery, radioiodine, and external radiation therapy on the clinical outcome of patients with differentiated thyroid carcinoma. Cancer. 1998;82:375–88.
Tubiana M, Schlumberger M, Rougier P, Laplanche A, Benhamou E, Gardet P, et al. Long-term results and prognostic factors in patients with differentiated thyroid carcinoma. Cancer. 1985;55:794–804.
Schlumberger M, Challeton C, De Vathaire F, Travagli JP, Gardet P, Lumbroso JD, et al. Radioactive iodine treatment and external radiotherapy for lung and bone metastases from thyroid carcinoma. J Nucl Med. 1996;37:598–605.
Shoup M, Stojadinovic A, Nissan A, Ghossein RA, Freedman S, Brennan MF, et al. Prognostic indicators of outcomes in patients with distant metastases from differentiated thyroid carcinoma. J Am Coll Surg. 2003;197:191–7.
Dinneen SF, Valimaki MJ, Bergstralh EJ, Goellner JR, Gorman CA, Hay ID. Distant metastases in papillary thyroid carcinoma: 100 cases observed at one institution during 5 decades. J Clin Endocrinol Metab. 1995;80:2041–5.
Schlumberger M, Tubiana M, De Vathaire F, Hill C, Gardet P, Travagli JP, et al. Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab. 1986;63:960–7.
Pak K, Kim SJ, Kim IJ, Kim BH, Kim SS, Jeon YK. The role of 18F-fluorodeoxyglucose positron emission tomography in differentiated thyroid cancer before surgery. Endocr Relat Cancer. 2013;20:R203–13.
Kohlfurst S. The role of nuclear medicine in differentiated thyroid cancer. Wien Med Wochenschr. 2012;162:407–15.
Wang W, Macapinlac H, Larson SM, Yeh SD, Akhurst T, Finn RD, et al. [18F]-2-fluoro-2-deoxy-d-glucose positron emission tomography localizes residual thyroid cancer in patients with negative diagnostic (131)I whole body scans and elevated serum thyroglobulin levels. J Clin Endocrinol Metab. 1999;84:2291–302.
Palmedo H, Bucerius J, Joe A, Strunk H, Hortling N, Meyka S, et al. Integrated PET/CT in differentiated thyroid cancer: diagnostic accuracy and impact on patient management. J Nucl Med. 2006;47:616–24.
Kaneko K, Abe K, Baba S, Isoda T, Yabuuchi H, Sasaki M, et al. Detection of residual lymph node metastases in high-risk papillary thyroid cancer patients receiving adjuvant I-131 therapy: the usefulness of F-18 FDG PET/CT. Clin Nucl Med. 2010;35:6–11.
Feine U, Lietzenmayer R, Hanke JP, Held J, Wohrle H, Muller-Schauenburg W. Fluorine-18-FDG and iodine-131-iodide uptake in thyroid cancer. J Nucl Med. 1996;37:1468–72.
Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91:2892–9.
Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994;97:418–28.
Nagamachi S, Wakamatsu H, Kiyohara S, Nishii R, Mizutani Y, Fujita S, et al. Comparison of diagnostic and prognostic capabilities of (1)(8)F-FDG-PET/CT, (1)(3)(1)I-scintigraphy, and diffusion-weighted magnetic resonance imaging for postoperative thyroid cancer. Jpn J Radiol. 2011;29:413–22.
La Quaglia MP, Black T, Holcomb GW 3rd, Sklar C, Azizkhan RG, Haase GM, et al. Differentiated thyroid cancer: clinical characteristics, treatment, and outcome in patients under 21 years of age who present with distant metastases. A report from the Surgical Discipline Committee of the Children’s Cancer Group. J Pediatr Surg. 2000;35:955–9 (discussion 960).
Francis Z, Schlumberger M. Serum thyroglobulin determination in thyroid cancer patients. Best Pract Res Clin Endocrinol Metab. 2008;22:1039–46.
Chung JK. Sodium iodide symporter: its role in nuclear medicine. J Nucl Med. 2002;43:1188–200.
Haymart MR. Understanding the relationship between age and thyroid cancer. Oncologist. 2009;14:216–21.
Jarzab B, Handkiewicz-Junak D, Wloch J. Juvenile differentiated thyroid carcinoma and the role of radioiodine in its treatment: a qualitative review. Endocr Relat Cancer. 2005;12:773–803.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Isoda, T., BaBa, S., Maruoka, Y. et al. Impact of patient age on the iodine/FDG “flip-flop” phenomenon in lung metastasis from thyroid cancer. Ann Nucl Med 30, 518–524 (2016). https://doi.org/10.1007/s12149-016-1104-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-016-1104-9