
Abstract
Aim
In this study, it was aimed to explore the prognostic factors in patients who received selective internal radiation therapy for hepatocellular cancer.
Materials and methods
A retrospective evaluation was made of 28 (24 male, 4 female, mean age 65.4 ± 6.8 years) hepatocellular cancer patients who received selective internal radiation therapy with Y-90 resin microspheres. Using Cox proportional hazards regression analysis, the relationship between age, gender, MELD score, serum albumin and AFP levels, number of liver lesions, size of the largest lesion, absence of 18F-FDG uptake, maximum standardized uptake value and overall survival times was analyzed.
Results
Treatment was applied to the right lobe in 22 and both in 6 patients. Mean treatment dose was 1.5 ± 0.2 GBq. Number of liver lesions were 1, <5 and multiple in 16, 5 and 7 patients, respectively, and the mean size of the largest lesion was 41.5 mm (min–max 15–160 mm). While 18F-FDG uptake was seen in 24 patients, liver lesions were hypometabolic in 4 patients. Mean SUVmax of liver lesions was calculated as 5.3 ± 0.3. During the mean 17.8 (min–max 2–39) months follow-up period, 19 patients died. Median survival time was computed as 18 ± 5 months (95 % CI 8.1–27.8). Age (p = 0.04), serum AFP level (p = 0.03) and size of the largest lesion (p = 0.02) had a significant negative effect on survival according to the Cox proportional hazards regression analysis.
Conclusion
Age, serum AFP level and the size of the largest liver lesion have a negative significant effect on survival of hepatocellular cancer patients who received selective internal radiation therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The most frequent primary hepatic tumor is hepatocellular carcinoma (HCC), which is the third most common cause of cancer-related deaths worldwide [1, 2]. Survival depends on treatment options, which is strongly associated with the stage of the disease [3]. Treatment options vary from local ablative treatments or chemotherapy to curative treatments such as surgical resection or liver transplantation [4–7].
In the past, HCCs have been accepted as radio-resistant tumors due to the limited effect of external beam radiotherapy. Different from external beam radiotherapy, selective internal radiation therapy (SIRT) has been shown to be a promising local ablative treatment method providing high doses selectively on the tumor but preserving the disease-free liver parenchyma and decreasing the side effects [8]. Survival of HCC after SIRT has a variable range and beyond the established criteria for patient selection, information about prognostic factors is limited. The relationship between clinical/radiological characteristics and survival after SIRT has been analyzed in a few recent studies [9–11].
In this study, it was aimed to explore the radiological characteristics, prognostic factors and survival rates of a patient group who received SIRT for HCC.
Materials and methods
Patients
The study included 28 patients (24 males, 4 females, mean age 65.4 ± 6.8 years, range 54–75 years) who received SIRT treatment for HCC between June 2008 and April 2013. All the patients had unresectable HCC lesions and none of them had received prior treatment before SIRT. Patients with decompensated Child C cirrhosis were not included in the study. Age, gender, Model for End-stage Liver Disease (MELD) score, serum albumin and alpha-fetoprotein (AFP) level of patients, number, size, 18F-FDG uptake patterns (hyper/hypo-metabolic) and SUVmax of liver lesions were noted for statistical analysis. The patients were divided into 3 groups according to the number of lesions (single, <5, multiple). Patients who died of other diseases were excluded from the study.
18F-FDG PET/CT
PET/CT images were acquired with a GE Discovery ST PET/CT scanner. Patients fasted for at least 6 h before imaging and blood glucose levels were checked. Those with a blood glucose level above 150 mg/dL did not undergo scanning. Oral contrast was given to all patients. Images from the vertex to the proximal femur were obtained while the patients were in the supine position. Whole body 18F-FDG PET/CT imaging was performed approximately 1 h after an intravenous injection of 296–370 MBq 18F-FDG. During the waiting period, patients rested in a quiet room without taking any muscle relaxants. PET images were acquired for 4 min per bed position. Emission PET images were reconstructed with non-contrast CT images. CT images were also obtained from the patient’s integrated 18F-FDG PET/CT with the use of a standardized protocol of 140 kV, 70 mA, tube rotation time of 0.5 s per rotation, a pitch of 6 and a slice thickness of 5 mm. Patients were allowed to breathe normally during the procedure. Attenuation-corrected PET/CT fusion images were reviewed in three planes (transaxial, coronal and sagittal) on a Xeleris Workstation 4.2 (GE Medical Systems). PET/CT images were evaluated and confirmed visually and semi-quantitatively with standardized uptake value (SUV) by consensus of two experienced nuclear medicine specialists.
SIRT treatment
In all patients, the widely accepted parameters of liver reserve, bone marrow reserve (granulocytes >1500/μL, platelets >60,000/μL), and hepatic vascularity were used as inclusion and exclusion criteria. Liver reserve was evaluated using bilirubin, aspartate transaminase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP) levels in the blood. A bilirubin level <2 mg/dL and AST/ALT/ALP levels less than 5 times the normal upper limit were required for radio-embolization. In patients who were suitable for therapy, the 90Y dose was adjusted according to the following body surface area (BSA) method: activity (GBq) = (BSA − 0.2) + tumor volume/total liver volume. Informed consent was obtained from all patients. The 90Y resin microspheres (Sirtex Medical, Australia) were injected through superselective catheterization of the hepatic artery catheter under intermittent fluoroscopic visualization. Within 1–24 h after microsphere infusion, Bremsstrahlung images were obtained to confirm that the 90Y was deposited only in the liver. All patients were hospitalized overnight and medications such as analgesics, antiemetic, and H2 antagonists were administered, if necessary. All patients were closely monitored until acute or late toxicities were resolved.
Treatment response and survival
Treatment response was evaluated by RECIST criteria in all the patients. In addition, 18F-FDG PET/CT was performed at the sixth week of treatment in patients with liver lesions FDG avid in baseline scan. Disease progression criteria were accepted as increase in tumor volume, progressive elevation of serum AFP levels and detection of new distant metastases. Date of death was noted for overall survival analysis.
Data and statistical analysis
SPSS software package (Version 16.0, SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Life tables and Kaplan–Meier analysis were performed for survival analysis. Cox-regression analysis was used to analyze the effect of age and gender, MELD score, serum albumin and AFP levels of patients, number, size, 18F-FDG uptake pattern and SUVmax of liver lesions to overall survival times.
Results
Treatment was applied to the right lobe in 22 patients and both lobes in 6 patients. The mean treatment dose was calculated as 1.5 ± 0.2 GBq. Acute radiation syndrome that could be relieved by symptomatic treatment developed in all the patients. Y-90 uptake was observed in the liver lesions of all patients during Bremsstrahlung imaging. Gastric ulcer was seen in 2 patients in the follow-up period. During the follow-up period, 1 patient received a second dose of SIRT and 2 patients TACE for radiologically progressive disease. The mean MELD score, serum albumin and AFP levels of patients were calculated as 8.0 ± 1.8, 3.7 ± 0.6 and 108.3 ± 187.4, respectively.
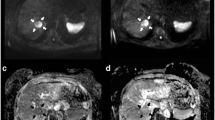
The number of liver lesions were single, fewer than 5 and multiple in 16, 5 and 7 patients, respectively, and the mean size of the largest lesions was 41.5 mm (min–max 15–160 mm). While liver lesions of 24 patients were 18F-FDG avid, they were hypometabolic in 4 patients. The mean SUVmax of liver lesions was calculated as 5.3 ± 0.3.
At 6 weeks after treatment, the mean MELD score, serum albumin and AFP levels of patients were calculated as 7.5 ± 1.4, 3.1 ± 0.4 and 89.1 ± 110.2, respectively. At that time, the mean size of the largest lesions was 38.6 mm (min–max 15–132 mm) and mean SUVmax of liver lesions was 3.5 ± 0.7. The liver lesions of 6 out of 24 patients became hypometabolic after SIRT. Partial response to treatment was observed in 12 out of 28 patients.
During the mean 17.8 ± 14.8 months follow-up period, 19 patients died (Fig. 1). Median survival time was computed as 18 ± 5 months (min–max 2–39 months) (95 % CI 8.1–27.8) (Table 1). AFP level (p = 0.03), age (p = 0.04) and size of the largest lesion (p = 0.02) had a significant negative effect on survival according to Cox proportional hazards regression analysis (Table 2).

Overall survival for whole patient group
Discussion
The therapeutic options for HCC have evolved in the past decade and different systemic and local therapies such as sorafenib, sunitinib, chemo-embolization and radio-embolization have been used for this malignancy. The anti-tumor effects of these therapeutic methods may result in changes in the radiological characteristics of the tumor, such as vascularization and necrosis. However, a significant change in tumor size according to RECIST criteria might not be seen in a large proportion of patients. Several studies have demonstrated that RECIST criteria might not be a reliable indicator of response to treatment in HCC [12–15]. Although 18F-FDG PET/CT can be used to evaluate early response to therapy in most solid tumors, due to the variety of glucose 6 phosphatase activity in HCCs, an important group of tumors are not 18F-FDG avid. Therefore, the role of 18F-FDG PET/CT in the response evaluation of HCCs is limited.
SIRT is an emerging treatment modality of unresectable HCCs with well-described technique, outcome and safety data [8–12]. Although the appropriateness criteria for SIRT are standard and well known, treatment outcome and survival after SIRT have a wide range [16, 17]. Due to this variability of survival and outcome, a few recent studies have focused on pretreatment clinical and radiological prognostic factors to predict survival times [9–11]. In this single center experience, some descriptive and morphological features of our patients were analyzed to predict the survival times after SIRT. Age and size of the largest lesion were found to have a significant negative correlation with survival times. A one unit increase in age and size of the largest lesion caused 1.9- and 1.2-fold increase in hazard, at any time. In a recent study by Golfieri et al. [11] survival and tolerability of radio-embolization were compared in elderly and younger HCC patients. No significant difference between survival times was determined between the two groups of younger and older than 70 years although no analysis was made of the effect of age below 70 years. In another study, Salem et al. [10] retrospectively investigated change in radiological parameters in the prediction of outcome of HCC patients treated with SIRT. Lower hepato-pulmonary shunt fraction, central hypervascularity and well-defined tumor margins were found to be associated with improved progression-free survival. Weng et al. [9] determined the number of tumor nodules, the MELD score and serum C-reactive protein levels to be independent risk factors.
In the current study, no relationship was shown between survival times and the number of liver lesions, absence of 18F-FDG uptake, maximum standardized uptake values and response to treatment. As SIRT was applied to the whole liver lobe, the number of lesions in the same lobe might not be an important prognostic factor. However, in this analysis, the size of the largest lesion was one of the significant factors. In consideration of the 4 mm mean range of beta particles of Y-90 in the tumors without peripheral vascularity, radiation exposure of peripheral tumor cells could be limited [18]. The role of 18F-FDG PET/CT in the management of HCC patients has been controversial. In a previous study of the current study group with a smaller patient number, the prognostic importance was shown of 18F-FDG uptake in HCC patients treated with SIRT [19]. Contrarily, in the current analysis, no relationship could be established between survival times and 18F-FDG uptake and SUV values. In this analysis, another insignificant factor to predict survival was the response to treatment. An absence of complete response and the local nature of SIRT might be explanations for this situation. In addition, more parameters could not be analyzed because of the retrospective design and limited number of patients. Larger and prospective-randomized studies are needed to describe the need and role of 18F-FDG PET/CT in the monitoring of HCC patients treated with SIRT and the prognostic importance of a wide range of clinical parameters.
Conclusion
Age, serum AFP level and size of the largest liver lesion have a significant negative effect on survival of hepatocellular cancer patients who received selective internal radiation therapy. According to the data of this retrospective analysis, younger patients with smaller lesions seem to be more appropriate to SIRT.
References
Röcken C, Carl-McGrath S. Pathology and pathogenesis of hepatocellular carcinoma. Dig Dis. 2001;19:269–78.
Llovet JM, Fuster J, Bruix J, Barcelona-Clínic Liver Cancer Group. The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004;10:115–20.
Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinoma in patients with cirrhosis. N Engl J Med. 1996;334:693–9.
Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37:429–42.
Treiber G. Systemic treatment of hepatocellular carcinoma. Dig Dis. 2001;19:311–23.
Aguayo A, Patt YZ. Nonsurgical treatment of hepatocellular carcinoma. Semin Oncol. 2001;28:503–13.
Lau WY, Kennedy AS, Kim YH, et al. Patient selection and activity planning. Int J Radiat Oncol Biol Phys. 2012;82(401Y):407.
Ahmadzadehfar H, Biersack HJ, Ezziddin S. Radioemmbolisation of liver tumors with Yttrium-90 microspheres. Semin Nucl Med. 2010;40:105–21.
Weng Z, Ertle J, Zheng S, Lauenstein T, Mueller S, Bockisch A, Gerken G, Yang D, Schlaak JF. A new model to estimate prognosis in patients with hepatocellular carcinoma after yttrium-90 radioembolization. PLoS ONE. 2013;8(12):e82225.
Salem ME, Jain N, Dyson G, Taylor S, El-Refai SM, Choi M, Shields AF, Critchfield J, Philip PA. Radiographic parameters in predicting outcome of patients with hepatocellular carcinoma treated with yttrium-90 microsphere radioembolization. ISRN Oncol. 2013;15(2013):538376.
Golfieri R, Bilbao JI, Carpanese L, Cianni R, Gasparini D, Ezziddin S, Paprottka PM, Fiore F, Cappelli A, Rodriguez M, Ettorre GM, Saltarelli A, Geatti O, Ahmadzadehfar H, Haug AR, Izzo F, Giampalma E, Sangro B, Pizzi G, Notarianni E, Vit A, Wilhelm K, Jakobs TF, Lastoria S, European Network on Radioembolization with Yttrium-90 Microspheres (ENRY) study collaborators. Comparison of the survival and tolerability of radioembolization in elderly vs. younger patients with unresectable hepatocellular carcinoma. J Hepatol. 2013;59(4):753–61. doi:10.1016/j.jhep.2013.05.025.
Faivre S, Zappa M, Vilgrain V, Boucher E, Douillard JY, Lim HY, Kim JS, Im SA, Kang YK, Bouattour M, Dokmak S, Dreyer C, Sablin MP, Serrate C, Cheng AL, Lanzalone S, Lin X, Lechuga MJ, Raymond E. Changes in tumor density in patients with advanced hepatocellular carcinoma treated with sunitinib. Clin Cancer Res. 2011;17(13):4504–12.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60.
Kim KW, Lee JM, Choi BI. Assessment of the treatment response of HCC. Abdom Imaging. 2011;36(3):300–14.
Sangro B, Salem R, Kennedy A, et al. Radioembolization for hepatocellular carcinoma: a review of the evidence and treatment recommendations. Am J Clin Oncol. 2011;34:422–31.
Seinstra BA, Defreyne L, Lambert B, Lam MG, Verkooijen HM, van Erpecum KJ, van Hoek B, van Erkel AR, Coenraad MJ, Al Younis I, van Vlierberghe H, van den Bosch MA. Transarterial radioembolization versus chemoembolization for the treatment of hepatocellular carcinoma (TRACE): study protocol for a randomized controlled trial. Trials. 2012;13:144.
Giammarile F, Bodei L, Chiesa C, Flux G, Forrer F, Kraeber-Bodere F, Brans B, Lambert B, Konijnenberg M, Borson-Chazot F, Tennvall J, Luster M, The Therapy, Oncology and Dosimetry Committees. EANM procedure guideline for the treatment of liver cancer and liver metastases with intra-arterial radioactive compounds. Eur J Nucl Med Mol Imaging. 2011;38(7):1393–406.
Kucuk ON, Soydal C, Araz M, Bilgic S, Ibis E. Prognostic importance of 18F-FDG uptake pattern of hepatocellular cancer patients who received SIRT. Clin Nucl Med. 2013;38(7):e283–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Soydal, C., Keskin, O., Kucuk, O.N. et al. Prognostic factors for prediction of survival of hepatocellular cancer patients after selective internal radiation therapy. Ann Nucl Med 29, 426–430 (2015). https://doi.org/10.1007/s12149-015-0962-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-015-0962-x