
Abstract
Purpose
Cardiac sarcoidosis is most commonly found in the left ventricular (LV) free wall. Presence in the right ventricle (RV) is less common but might be useful for detecting cardiac involvement of sarcoidosis. 18F-fluorodeoxyglucose (18F-FDG) PET has been used to detect LV regions with cardiac sarcoidosis. However, the same has not been done for RV involvement. The aims of the current study were to evaluate RV 18F-FDG uptake and its relationship to the distribution of LV wall 18F-FDG-positive segments in the LV, and to evaluate whether patients with positive RV 18F-FDG uptake met the 1993 diagnostic criteria of the Japanese Ministry of Health and Welfare (JMHW) guidelines regarding sarcoidosis with suspected cardiac involvement.
Method
Fifty-nine biopsy-proven extra-cardiac sarcoidosis patients (age 56.1 ± 14.7 years) with suspected cardiac involvement based on abnormal electrocardiography or echocardiography findings underwent fasting 18F-FDG PET or PET/CT. The LV wall was divided into 17 segments and RV uptake was also evaluated.
Result
Among 59 patients, 35 (59.3 %) showed some abnormal 18F-FDG uptake in the RV and/or LV wall. With respect to the RV wall, 13 (22.0 %) showed abnormal 18F-FDG uptake. The number of LV-involved segments was 4.8 ± 2.4 in the patients with RV 18F-FDG uptake, which was significantly higher than in the patients without RV uptake, 1.8 ± 2.2 (P < 0.0001). Patients with RV uptake more frequently met the diagnostic criteria of the 1993 JMHW guidelines (n = 27), than did those without RV uptake (84.6 vs. 34.8 %, P = 0.0033).
Conclusion
18F-FDG PET identified RV involvement less frequently than LV involvement in this study population. However, patients who had RV uptake showed a greater number of LV-involved segments and met the JMHW diagnostic criteria more frequently. Although RV uptake is less frequent, 18F-FDG RV uptake may be useful in diagnosing cardiac involvement in sarcoidosis.
Clinical trial registration
UMIN000006533.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Sarcoidosis is a multisystem granulomatous disease with unknown etiology. It is commonly found in young and middle-aged adults. Incidence varies widely due to differences in environmental risk factors and genetic factors, and manifestation varies from an asymptomatic state to a progressive disease [1, 2]. Cardiac involvement sarcoidosis (CS) is considered to be the main cause of morbidity and death related to conducting-system abnormalities, ventricular arrhythmia, and heart failure [1, 2]. Recently, the incidence of cardiac involvement sarcoidosis has reportedly been increasing and this increase has been associated with increasing mortality in Europe and North America [3]. Therefore, the need for sensitive and accurate diagnosis of cardiac involvement has increased in recent years.
18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) is a useful diagnostic test for detecting active inflammatory lesions associated with sarcoidosis [4, 5]. 18F-FDG is also useful for detecting cardiac involvement in sarcoidosis [5, 6].
Data on right ventricular (RV) 18F-FDG uptake have been very limited, and moreover the prevalence and diagnostic usefulness of RV 18F-FDG uptake have not been well reported. A limited number of autopsy studies have examined RV involvement in sarcoidosis. The frequency of RV involvement was lower than that of left ventricular (LV) involvement [7, 8]. However, the frequency of RV involvement has not been fully studied. In addition, the association between RV involvement and the distribution of LV sarcoidosis lesions has not been studied in accordance with 1993 Japanese Ministry of Health and Welfare (JMHW) guidelines. Therefore, the aims of this study were to evaluate the frequency of RV 18F-FDG uptake and its relationship to the numbers of 18F-FDG-positive LV regions in sarcoidosis patients with suspected cardiac involvement. In addition, we also evaluated whether patients who had positive RV 18F-FDG uptake more frequently met the diagnostic criteria of JMHW guidelines regarding cardiac sarcoidosis than did patients who did not have RV 18F-FDG uptake [9].
Materials and methods
Study population
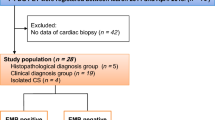
Seventy-six histologically proven extra-cardiac sarcoidosis patients were prospectively involved in this study from January 2003 to May 2013. These patients had suspected cardiac involvement given their electrocardiography (ECG) or echocardiographic (UCG) abnormalities. Patients with a history of coronary artery disease (CAD) were excluded from this study. We performed additional evaluations, including stress myocardial perfusion imaging or coronary angiography (CAG) in those with multiple coronary risk factors to exclude patients with CAD. Using echocardiography we also excluded patients with any other known heart disease such as myocarditis, valvular heart disease, or other cardiomyopathies [4, 10, 11]. In terms of LV wall assessment, 17 patients who showed diffuse physiological myocardial 18F-FDG uptake were also excluded from LV analysis [5]. Therefore, 59 patients (14 male, 45 female, 56.1 ± 14.7 years old) with biopsy-proven extra-cardiac sarcoidosis were included in this study (Table 1). Cardiac involvement was defined based on the 1993 JMHW guidelines for diagnosing cardiac sarcoidosis (Table 2) [9]. This study protocol was approved by the ethics committee of the Hokkaido University Graduate School of Medicine. Written informed consent was obtained prior to the study.
PET imaging
All patients fasted for at least 6 h before 18F-FDG PET studies to reduce physiological myocardial uptake of 18F-FDG [5]. Unfractionated heparin (UFH; 50 IU/kg, Mochida, Tokyo) was injected intravenously in all patients 15 min prior to 18F-FDG injection also in order to reduce physiological myocardial 18F-FDG uptake [10]. Prior to 18F-FDG PET imaging studies, we checked for contraindication of heparin use such as active bleeding, bleeding risk, or a history of heparin-induced thrombocytopenia (HIT). None of the patients in this study population had contraindication for heparin use. PET imaging was performed using a Siemens ECAT EXACT HR+ scanner (Siemens/CTI, Knoxville, TN, USA) (n = 37) or a Biograph 64 TruePoint with TrueV PET/computed tomography (CT) scanner (Siemens Japan, Tokyo) (n = 22). Transmission scanning for PET or a low-dose CT for PET/CT was performed for attenuation correction. Scans were performed at 45–60 min after the administration of 224.1 ± 57.0 MBq of 18F-FDG [12]. Blood samples were obtained before and 15 min after UFH administration to measure immunoreactive insulin (IRI) and free fatty acids (FFA). Fasting plasma glucose level was measured before 18F-FDG injection.
Data analysis
ECG data analysis
Resting 12-lead ECG and 24-hour ambulatory ECGs were analyzed by cardiologists blinded to clinical and 18F-FDG PET information. Based on the JMHW guidelines, right bundle branch block (RBBB), atrioventricular (AV) block, left-axis deviation, ventricular tachycardia (VT), premature ventricular contraction (PVC) (>grade 2 in Lown’s classification), and abnormal Q or ST-T changes were defined as abnormal [9].
Echocardiography
All patients underwent transthoracic UCG using a 2.5 MHz echo-Doppler probe with a SONOS 5500 imaging system (Agilent Technologies, Andover, MA, USA). Echocardiography data were also analyzed by cardiologists blinded to clinical and 18F-FDG PET information. The LV end-diastolic and end-systolic dimensions were analyzed using M-mode or B-mode echocardiography. Based on JMHW guidelines, abnormal wall motion, regional wall thinning or thickening, and dilatation of the left ventricle were considered abnormal for UCG [9].
18F-FDG PET or PET/CT imaging analysis
Acquired images were resliced into a series of short-axis, horizontal long-axis, and vertical long-axis images. 18F-FDG uptake in the RV and LV myocardium were evaluated visually. Uptake was defined as being positive if it was greater than that for a physiologically normal liver [4, 13]. The LV wall was divided into 17 segments based on American Society of Nuclear Cardiology (ASNC) imaging guidelines [14] to count the number of 18F-FDG involved segments. Two nuclear medicine physicians blinded to clinical and other test data independently evaluated the LV myocardial 18F-FDG images. Discordant findings were evaluated by a third observer. In RV analysis, we evaluated first whether or not there was any positive uptake. In the case of positive RV 18F-FDG uptake, we also evaluated the distribution as being either diffuse or focal. Positive RV uptake was examined regionally. A regional 18F-FDG uptake that was higher than that of a physiologically normal liver was defined as positive [4, 6]. Evaluation criteria for positive regional RV myocardial 18F-FDG uptake were similar. RV uptake was measured against numbers of LV-involved segments and JMHW guideline criteria [9].
Perfusion analysis
Perfusion analysis was done for 56 patients (94.9 %; 50 patients were studied by 99mTc-MIBI scintigraphy, and 6 patients with 15O-water PET) of the 59 patients. Two nuclear medicine physicians independently evaluated the myocardial perfusion images or myocardial blood flow. Discordant findings were evaluated by a third observer. We assessed myocardial perfusion distribution based on ASNC imaging guidelines (Updated imaging guidelines for nuclear cardiology procedures 2001).
Statistical analysis
Data are expressed as the mean ± standard deviation (SD), and a P value of less than 0.05 is considered statistically significant. For intra-group comparisons, Wilcoxon signed-rank tests were applied to compare differences in the total number of positive 18F-FDG uptake segments between patients with and patients without RV uptake. Fisher’s exact test was used to compare discrete data as appropriate. Pearson’s correlation coefficient was used for the comparison of the patients’ characteristics among the 18F-FDG uptake variations. Statistical calculations were carried out using statistical software (JMP version 10, SAS Institute, Cary, NC, USA).
Results
Patient characteristics
Characteristics of study subjects are found in Table 1. Forty-five patients (76.3 %) showed ECG abnormalities. Three patients’ UCG data were not evaluated due to poor image quality. Thus, 58.9 % (33/56) of patients showed echocardiographic abnormalities. There was no patient who had normal ECG and normal UCG in the current study. Fifty-six out of 59 (94.9 %) patients had myocardial perfusion imaging and 22 of 56 patients (39.3 %) showed abnormal findings. Sixteen patients had Ga scintigraphy and no patient showed positive Ga uptake in the LV. Two patients had myocardial biopsy. One patient showed positive and another patient showed nonspecific findings. There were two diabetic patients and 4 patients being treated with corticosteroids. However, the mean fasting serum glucose level was within the normal range [15]. The fasting serum glucose levels at the time of the PET scan were under 120 mg/dL except for one patient with diabetes. The diabetic patient showed a higher fasting serum glucose level, 178 mg/dL, but the 18F-FDG PET image quality was good and was suitable for the analysis.
Blood sample data
Among 59 sarcoidosis patients, 53 had IRI data and 54 had FFA data. Blood samples were insufficient to measure IRI in 6 patients and FFA in 5 patients. FFA values were significantly increased after UFH administration in all 59 patients (P < 0.0001) (Table 3). IRI did not significantly increase after UFH administration (P = 0.072). No patients had any side effects from UFH.
JMHW diagnostic criteria
Among 59 patients, 27 met the 1993 JMHW diagnostic criteria for cardiac sarcoidosis. The remaining 32 did not meet the diagnostic criteria.
18F-FDG PET or PET/CT findings
Among a total of 59 patients, 35 (59.3 %) showed some abnormal uptake in the RV and/or LV wall. With respect to the RV wall, 13 (22.0 %) showed abnormal 18F-FDG uptake. One patient showed only RV wall 18F-FDG uptake without any LV wall uptake (Fig. 1). All patients who had RV 18F-FDG uptake showed a non-diffuse pattern.

Frequency of right and left ventricular wall involvement. Fifty-nine % of patients showed abnormal uptake in the ventricular wall. RV 18F-FDG uptake in suspected cardiac sarcoidosis was less frequent than was LV involvement. LV left ventricle, RV right ventricle, 18 F-FDG 18F-fluorodeoxyglucose
The number of LV-involved segments was 4.8 ± 2.3 in patients with RV 18F-FDG uptake, which was significantly higher than in patients without RV uptake, 1.8 ± 2.2 (P < 0.0001) (Fig. 2).

Total number of segments. LV involvement was broader in patients with RV 18F-FDG uptake than in patients without RV 18F-FDG uptake. LV left ventricle, RV right ventricle, 18 F-FDG 18F-fluorodeoxyglucose
Patients with RV uptake more frequently met the diagnostic criteria of JMHW guidelines (84.6 %) uptake than did patients who did not have RV uptake (34.8 %, P = 0.0033) (Fig. 3a). Patients with LV 18F-FDG uptake also more frequently met the diagnostic criteria of JMHW guidelines than did patients without LV 18F-FDG uptake (63.6 vs. 8.3 %, P < 0.0001) (Fig. 3b).

Relationships between 18F-FDG uptake and JMHW diagnostic criteria. Patients with RV 18F-FDG uptake in suspected cardiac sarcoidosis more frequently met the 1993 JMHW diagnostic criteria for cardiac involvement of sarcoidosis than did patients without RV 18F-FDG uptake (a). Patients with LV uptake also showed the same tendency (b). 18 F-FDG 18F-fluorodeoxyglucose, RV right ventricle, JMHW Japanese Ministry of Health and Welfare
Among 27 patients who met the JMHW diagnostic criteria, 25 (92.6 %) showed some abnormal uptake in cardiac lesions. With regard to LV-involved segments in patients who met the JMHW diagnostic criteria, 11 patients with RV 18F-FDG uptake showed significantly higher numbers of LV-uptake segments than did patients without RV 18F-FDG uptake (n = 16) (5.3 ± 2.1 vs. 3.3 ± 2.0, P = 0.02) (Fig. 4).

Representative case of 63-year-old male. Maximum intensity projection view of 18F-FDG PET (a), axial view at cardiac level (b), horizontal long-axis view at upper ventricle level (c), short-axis view at mid ventricle level (d) are shown. 18F-FDG PET shows significant focal accumulation in right ventricular wall (SUVmax 12.3), anteroseptal wall (SUVmax 12.3), and inferior wall (SUVmax 6.7). In addition, there are multiple lymph node uptakes in supraclavicular, mediastinum, hilar, and abdominal regions (a)
Excluded patients with LV diffuse 18F-FDG uptake
Among 17 excluded patients with LV diffuse 18F-FDG uptake, 1 patient met the diagnostic criteria of JMHW diagnostic guidelines. However, no excluded patients showed abnormal RV 18F-FDG uptake.
Perfusion findings
For the perfusion analysis, 22 patients (39.3 %) showed some perfusion abnormalities. All patients with an abnormal perfusion scan demonstrated a positive 18F-FDG PETscan.
Comparison of the patient characteristics among 18F-FDG uptake patterns Background and clinical data were compared among patients without myocardial 18F-FDG uptake, with only LV uptake, and with RV uptake (Table 4). There were no significant differences in age and gender among the 3 groups. The frequency of echocardiography was higher in patients with positive RV uptake than it was for those with negative 18F-FDG uptake. The frequency of perfusion abnormalities and of meeting JMHW criteria was higher in both LV only 18F-FDG-positive uptake and RV positive uptake patients than they were in patients without 18F-FDG uptake. However, there was no significant difference between the patients with only LV uptake and patients with RV uptake.
Discussion
We have reported the frequency and patterns of RV 18F-FDG uptake in patients with suspected cardiac sarcoidosis. RV 18F-FDG uptake was less frequent than was LV uptake, but patients who had RV 18F-FDG uptake showed higher numbers of LV 18F-FDG-positive segments than did patients without RV involvement. Patients with RV 18F-FDG uptake more frequently met the JMHW diagnostic criteria for cardiac involvement of sarcoidosis than did patients without RV 18F-FDG uptake. Patients with positive LV 18F-FDG uptake also more frequently met the diagnostic criteria of JMHW guidelines than did those without 18F-FDG uptake in the LV.
RV 18F-FDG uptake
RV 18F-FDG uptake in patients with suspected cardiac sarcoidosis was found less frequently in this study than was LV involvement (22.0 vs. 57.6 %, respectively). There have been very limited reports regarding RV 18F-FDG uptake in suspected cardiac sarcoidosis, and the frequency of RV 18F-FDG uptake has not been well reported. Previous studies have reported cardiac sarcoidosis in the RV region less frequently than in the LV region [7, 16]. Previous autopsy reports showed RV region involvement in 36–39 % of patients with sarcoidosis [7, 8]. The frequency of RV 18F-FDG uptake in this study is similar to but slightly lower than that found in previous autopsy studies. This difference may be associated with individual patients’ backgrounds. In fact, most of the patients in the current study did not have heart failure and possibly had less advanced cardiac damage or injury. In addition, some autopsy cases involved active inflammatory lesions and fibrosis. 18F-FDG accumulates in inflammatory lesions but not in fibrosis [17]. These properties may account for the differences between our present data and those from previous autopsy studies.
A more recent study from Blankstein et al. reported that 11 of 118 patients (9.3 %) with suspected cardiac sarcoidosis showed RV uptake [18]. The frequency of RV uptake of the previous study was lower than that of the current study. The difference between the two studies may be in patient backgrounds. The previous study included patients with suspected cardiac sarcoidosis without biopsy-proven extra-cardiac sarcoidosis. Therefore, some patients may not have had either cardiac sarcoidosis or sarcoidosis. This circumstance may have contributed to the low frequency of RV positive 18F-FDG uptake in the previous study.
RV 18F-FDG uptake and LV lesions
In the present study, patients with RV 18F-FDG uptake in suspected cardiac sarcoidosis showed broader LV regional uptake, and more frequently met the JMHW diagnostic criteria for cardiac involvement of sarcoidosis than did patients without RV 18F-FDG uptake. UCG abnormality was more frequent in patients with RV uptake than it was in those without 18F-FDG uptake. In patients who met the JMHW diagnostic criteria, those with RV involvement also showed significantly greater LV involvement than did those without RV lesions. Two previous autopsy studies reported the frequency of LV and RV chamber involvement in cardiac sarcoidosis [7, 8]. However, these studies did not evaluate the association between RV sarcoid lesions and LV sarcoid lesions. In the autopsy cases, patients who died from cardiac sarcoidosis more frequently had RV regional involvement than did those who died from another cause [8], possibly implying that RV involvement occurs in the advanced stages of sarcoidosis. Thus, the current data may be in line with previous data and may provide further insight into RV 18F-FDG uptake and its association with a broader distribution of sarcoid lesions in the LV. This possibility requires further study.
RV physiological uptake
18F-FDG PET is the diagnostic tool used to detect cardiac involvement in patients with sarcoidosis [5, 17, 19–22]. However, diffuse LV wall 18F-FDG uptake sometimes makes it difficult to distinguish between active inflammation caused by cardiac sarcoidosis and physiological uptake. On the other hand, the physiological 18F-FDG uptake in the RV is usually less prevalent and less intense than that in the LV [23]. Therefore, it is not difficult to detect abnormal inflammatory uptake in the RV. In fact, in the current study, we were able to evaluate RV 18F-FDG uptake in patients who had LV diffuse physiological 18F-FDG uptake. Increased RV 18F-FDG accumulation has also been reported in the context of RV pressure overload due to valvular heart disease or pulmonary hypertension [24, 25]. In those situations, the uptake might be diffuse. In our study, patients with valvular heart disease were excluded, and none of the patients with diffuse RV uptake had suspected pulmonary hypertension. Therefore, patients with non-diffuse RV uptake were strongly suspected of having active inflammation due to the involvement of sarcoidosis.
Treatment decision making
In our institution, patients suspected of having sarcoidosis with focal 18F-FDG uptake but who do not meet the criteria are carefully followed up on using 12-lead ECG, Holter ECG, and UCG without steroid treatment since there is no established evidence of the advantage of steroid therapy for this patient population. Further studies are needed to assess treatment options.
Limitations
In this study, 18F-FDG uptakes were not compared with other pathological findings. It is not feasible to perform endomyocardial biopsies on all suspected regions. In addition, myocardial biopsy tends to have lower sensitivity in the diagnosis of cardiac sarcoidosis [8, 26, 27]. In the current study, all patients had at least biopsy-proven extra-cardiac sarcoidosis, and we defined cardiac involvement based on the widely accepted 1993 JMHW guidelines [6]. We also do not have enough data about prognosis yet, so we cannot discuss the relationship between RV uptake and prognosis.
The present study had methodological limitations. Twenty-two patients were evaluated using PET/CT and the remaining 37 patients were evaluated using PET. PET/CT has better spatial resolution than does PET. However, we defined as positive an obvious focal uptake that was higher than that for a normal liver, thereby allowing us to accurately detect abnormal regional uptake using PET as well as previous studies have done [4, 10, 20].
Conclusions
RV 18F-FDG involvement was associated with broader LV regional involvement and more closely met the diagnostic criteria for suspected cardiac sarcoidosis. RV 18F-FDG uptake is a hallmark of active and broad cardiac involvement of sarcoidosis in patients with suspected cardiac sarcoidosis.
RV 18F-FDG uptake might be useful in diagnosing cardiac involvement of sarcoidosis.
References
Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Eng J Med. 2007;357:2153–65.
Rybicki BA, Major M, Popovich J Jr, Maliarik MJ, Iannuzzi MC. Racial differences in sarcoidosis incidence: a 5 year study in a health maintenance organization. Am J Epidemiol. 1997;145:234–41.
O’Regan A, Berman JS. Sarcoidosis. Ann Intern Med. 2012;156(9):ITC5-1, ITC5-2, ITC5-3, ITC5-4, ITC5-5, ITC5-6, ITC5-7, ITC5-8, ITC5-9, ITC5-10, ITC5-11, ITC5-12, ITC5-13, ITC5-14, ITC5-15; quiz ITC5-16.
Manabe O, Ohira H, Yoshinaga K, Sato T, Klaipetch A, Oyama-Manabe N, et al. Elevated F-fluorodeoxyglucose uptake in the interventricular septum is associated with atrioventricular block in patients with suspected cardiac involvement sarcoidosis. Eur J Nucl Med Mol Imaging. 2013;40:1558–66.
Ohira H, Tsujino I, Yoshinaga K. (1)(8)F-fluoro-2-deoxyglucose positron emission tomography in cardiac sarcoidosis. Eur J Nucl Med Mol Imaging. 2011;38:1558–66.
Youssef G, Leung E, Mylonas I, Nery P, Williams K, Wisenberg G, Beanlands RS, et al. The use of 18F-FDG PET in the diagnosis of cardiac sarcoidosis: a systematic review and metaanalysis including the Ontario experience. J Nucl Med. 2012;53:241–8.
Roberts WC, McAllister HA Jr, Ferrans VJ. Sarcoidosis of the heart. A clinicopathologic study of 35 necropsy patients (group 1) and review of 78 previously described necropsy patients (group 11). Am J Med. 1977;63:86–108.
Tavora F, Cresswell N, Li L, Ripple M, Solomon C, Burke A. Comparison of necropsy findings in patients with sarcoidosis dying suddenly from cardiac sarcoidosis versus dying suddenly from other causes. Am J Cardiol. 2009;104:571–7.
Hiraga H, Hiroe M, Iwai K. Guidelines for diagnosis of cardiac sarcoidosis: study report on diffuse pulmonary diseases (in Japanese). Tokyo: The Japanese Ministry of Health and Welfare; 1993. p. 2.
Ishimaru S, Tsujino I, Takei T, Tsukamoto E, Sakaue S, Kamigaki M, et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur Heart J. 2005;26:1538–43.
Ohira H, Tsujino I, Ishimaru S, Oyama N, Takei T, Tsukamoto E, et al. Myocardial imaging with 18F-fluoro-2-deoxyglucose positron emission tomography and magnetic resonance imaging in sarcoidosis. Eur J Nucl Med Mol Imaging. 2008;35:933–41.
Ishida Y, Yoshinaga K, Miyagawa M, Moroi M, Kondoh C, Kiso K, et al. Recommendations for F-fluorodeoxyglucose positron emission tomography imaging for cardiac sarcoidosis: Japanese Society of Nuclear Cardiology Recommendations. Ann Nucl Med. 2014;28(4):393–403.
Laffon E, Adhoute X, de Clermont H, Marthan R. Is liver SUV stable over time in (1)(8)F-FDG PET imaging? J Nucl Med Technol. 2011;39:258–63.
Machac J, Bacharach SL, Bateman TM, Bax JJ, Beanlands R, Bengel F, et al. Positron emission tomography myocardial perfusion and glucose metabolism imaging. J Nucl Cardiol. 2006;13:e121–51.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004;27(Suppl 1):S5–S10.
Habersberger J, Manins V, Taylor AJ. Cardiac sarcoidosis. Intern Med J. 2008;38:270–7.
Manabe O, Oyama-Manabe N, Ohira H, Tsutsui H, Tamaki N. Multimodality evaluation of cardiac sarcoidosis. J Nucl Cardiol. 2012;19:621–4.
Blankstein R, Osborne M, Naya M, Waller A, Kim CK, Murthy VL, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol. 2014;63:329–36.
Ohira H, Tsujino I, Sato T, Yoshinaga K, Manabe O, Oyama N, et al. Early detection of cardiac sarcoid lesions with (18)F-fluoro-2-deoxyglucose positron emission tomography. Intern Med. 2011;50:1207–9.
Okumura W, Iwasaki T, Toyama T, Iso T, Arai M, Oriuchi N, et al. Usefulness of fasting 18F-FDG PET in identification of cardiac sarcoidosis. J Nucl Med. 2004;45:1989–98.
Yamagishi H, Shirai N, Takagi M, Yoshiyama M, Akioka K, Takeuchi K, et al. Identification of cardiac sarcoidosis with (13)N-NH(3)/(18)F-FDG PET. J Nucl Med. 2003;44:1030–6.
Tahara N, Tahara A, Nitta Y, Kodama N, Mizoguchi M, Kaida H, et al. Heterogeneous myocardial FDG uptake and the disease activity in cardiac sarcoidosis. JACC Cardiovasc Imaging. 2010;3:1219–28.
Lobert P, Brown RK, Dvorak RA, Corbett JR, Kazerooni EA, Wong KK. Spectrum of physiological and pathological cardiac and pericardial uptake of FDG in oncology PET-CT. Clin Radiol. 2013;68:e59–71.
Maurer AH, Burshteyn M, Adler LP, Steiner RM. How to differentiate benign versus malignant cardiac and paracardiac 18F FDG uptake at oncologic PET/CT. Radiographics. 2011;31:1287–305.
Kluge R, Barthel H, Pankau H, Seese A, Schauer J, Wirtz H, et al. Different mechanisms for changes in glucose uptake of the right and left ventricular myocardium in pulmonary hypertension. J Nucl Med. 2005;46:25–31.
Doughan AR, Williams BR. Cardiac sarcoidosis. Heart. 2006;92:282–8.
Kim JS, Judson MA, Donnino R, Gold M, Cooper LT Jr, Prystowsky EN, Prystowsky S. Cardiac sarcoidosis. Am Heart J. 2009;157:9–21.
Acknowledgments
The authors thank Hidehiko Omote, RT; Ken-ichi Nishijima, PhD; Daiske Abo, MSc; Kumi Ajiki, and Eriko Suzuki for their support for this study. This study was supported in part by grants from the Ministry of Education, Science and Culture Japan (Category B, No. 23390294, Category Young Investigator, No. 23790826), Hokkaido Heart Association for Research (H-23) (Sapporo, Japan), Adult Vascular Disease Research Foundation (#H22-23) (Kyoto, Japan), and North-Tech Research Foundation (#H23-S2-17, Sapporo, Japan). Dr. Yoshinaga is supported by the Imura Clinical Research Award (Adult Vascular Disease Research Foundation).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Manabe, O., Yoshinaga, K., Ohira, H. et al. Right ventricular 18F-FDG uptake is an important indicator for cardiac involvement in patients with suspected cardiac sarcoidosis. Ann Nucl Med 28, 656–663 (2014). https://doi.org/10.1007/s12149-014-0860-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-014-0860-7