
Abstract
Objectives
Semiquantitative evaluation of tracer uptake in basal ganglia is superior to visual assessment of images in dopamine transporter (DAT) scintigraphy especially in follow-up of the patients. Manual drawing of regions of interest (ROIs) in two-dimensional (2D) transaxial slices of the single photon emission computed tomography (SPECT) datasets leads to a large inter- and intra-reader variability, while being time consuming. Our aim was to investigate a technique that extracts 3D ROIs in a fully automated fashion and thus might provide reproducible user-independent results allowing better follow-up control and large-scale clinical studies.
Methods
The highest activity of 123IFP-CIT is expected in the basal ganglia. The proposed method (Spectalyzer) uses the following steps to localize this maximum and extract the ROIs in 3D: (1) Dithers the SPECT volume to obtain a 3D volume with binary only. (2) Models the obtained point distributions as two multivariate Gaussian distributions and estimated their parameters using the expectation maximization algorithm. (3) Using the original SPECT activity values, thresholding is performed using a fixed percentage of maximum activity as a parameter to obtain the 3D ROIs. (4) A reference volume in the occipital region is automatically found based on the location of the two ROIs. (5) From the 3D ROIs, statistical information like mean and median activity and the volume is extracted, relative to the activity in the reference region. The resulting values are compared with values from manual 2D ROIs. Further validation is performed by means of an anthropomorphic striatal phantom.
Results
The method was evaluated on 12 SPECT volumes including anthropomorphic striatal phantoms. In all cases the two basal-ganglia were successfully localized and the 3D ROIs estimated, with perfect reproducibility. The obtained values for the mean activity showed the same trend with the values obtained manually and also with the results of the 2D semiautomatic software, but without the substantial inter- and intra-reader variations.
Conclusions
The proposed method is successful in finding the 3D ROIs and performing the subsequent measurements automatically. It is proposed as an automatic reproducible approach for semiquantitative analysis of DAT scintigraphy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Structural and functional neuroimaging has a dramatic impact on differential diagnosis in patients with movement disorders [1] and has reportedly a significant value to cost effectiveness in patient management [2]. Functional imaging of the dopamine transporter (DAT) with 123-I-labelled radioligands defines integrity of the dopaminergic system and has its main clinical application in patients with mild, incomplete, or uncertain parkinsonism and in the differential diagnosis of movement disorders. Imaging with single photon emission computed tomography (SPECT) ligands for DAT (FP-CIT, β-CIT, IPT, TRODAT) provides a marker for presynaptic neuronal degeneration. The main pathophysiological feature in Parkinson’s syndromes is a severe degeneration of dopaminergic neurons in the substantia nigra, resulting in a loss of DATs in the striatum. Reduction of striatal radiotracer uptake correlates with disease severity, in particular bradykinesia and rigidity. Monitoring of disease progression assists in clinical trials of potential neuroprotective drugs and is of great importance in the differential diagnosis of movement disorders. Due to the degeneration of dopaminergic cells, resulting in a loss of DAT, DAT imaging may be found abnormal in idiopathic Parkinson’s disease (PD), multiple system atrophy (MSA), progressive supranuclear palsy (PSP), corticobasal degeneration (CBD) and dementia with Lewy bodies (DLB) but does not allow differentiation between these disorders. A normal scan suggests rather other pathologies such as essential tremor (ET), vascular parkinsonism, drug-induced parkinsonism, or psychogenic parkinsonism. Therefore, DAT imaging is clinically important in the differential diagnosis between degenerative Parkinson’s syndromes (PD, MSA, PSP, CBD, DLB) showing loss of DAT and non-degenerative Parkinson’s syndromes (e.g. vascular or medication induced Parkinson’s syndromes) as well as ET that show normal DAT density. Furthermore, DAT imaging is used for the early diagnosis of Parkinson’s syndromes as dopamine loss is seen even in the earliest clinical presentations of the disease [3, 4]. It was reported that DAT imaging can even be used as a predictor for the diagnosis of preclinical cases of parkinsonism by visualizing nigrostriatal degeneration preclinically [5]. Additional applications are the characterizing of dementia with parkinsonian features showing abnormal results in DLB and normal DAT density in Alzheimer’s disease [6, 7]. The presence of DATs can be exploited to image the nigrostriatal neuron viability/density. In patients with parkinsonian syndrome (PS) the reduction of DAT binding occurs in the putamen and caudate nucleus.
Usually with SPECT, the binding of radiotracers in certain brain areas is assessed by manual positioning of regions of interest (ROIs). The quantification of radiotracer binding in the striatum is determined by the ratio of specific binding of the tracer in the striatum and non-specific binding in another brain area. However, several methods are used for measurement of striatal tracer uptake, e.g. to set oval ROIs on somewhere in bilateral striatal regions with optional size, or to make irregularly shaped ROIs by means of fusion imaging with either magnetic resonance imaging (MRI) or computed tomography (CT). On the other hand, ROIs, which represent the uptake of the non-specific region, are sometimes selected in the occipital lobe, frontal lobe or cerebellum. To apply oval ROIs is a simple and easy procedure, but it can be arbitrary, especially when the uptake is faint. Furthermore, such manual positioning of ROIs for the quantification of radiotracer uptake is time consuming and is limited by a large investigator-dependent intra- and inter-individual variability. To perform fusion imaging and trace the striatal region on the images might be more correct and objective, but other imaging data such as CT or MRI are needed. We therefore evaluated a new fully automatic 3D semiquantitative procedure to more easily and objectively estimate the uptake of striatal regions of 123IFP-CIT (DaTSCAN) in patients with suspicion of Parkinson’s syndrome and ET and evaluate the method by comparing it to manually defined 2D ROIs as well as phantom studies. This software tool can be used for fully automated and standardized processing, evaluation and finally documentation of DaTSCAN SPECT scans.
Materials and methods
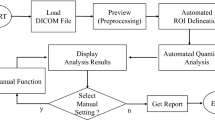
The proposed software (Spectalyzer, developed by Rene Donner) uses the following steps to localize these maxima and extracts the ROIs in 3D:
-
1.
Two activity maxima are assumed to be present in the brain volume and the expectation maximization (EM) algorithm is run to fit two Gaussian distributions to the activity volume. After localizing the two activity maxima in a neighbourhood of the centre of the found Gaussian distributions, one ROI per hemisphere is extracted by thresholding at a fixed percentage of the activity maximum. For this ROI the mean and median activities are computed.
-
2.
The distance from centre of the basal ganglia to the posterior border of the brain was divided by three, and in the third posterior part a large circular background was placed; median count of this region is assumed as the activity of the background.
-
3.
From the 3D ROIs statistical information like mean and median activity and the volume is extracted, relative to the activity in the reference region. The resulting values are compared with values from manual 2D ROIs and also further semiautomatic 2D measurement with commercially available software (BRASS, Hermes). Further validation was performed by means of an anthropomorphic striatal phantom. The input data are already reconstructed transaxial slices of the striatal SPECT study.
The software is written in Matlab R2009b (The Mathworks, Inc., Natick, MA, USA) using its functions of Image Processing Toolbox Version 6.4 and can be easily run in an ordinary computer with Windows software.
The underlying assumption of our approach is that the basal ganglia represent the maximal tracer uptake in the DaTSCAN, which is also the implicit assumption that medical experts make when interpreting DaTSCAN. Additionally, the overall activity distribution on the whole brain is expected to be approximated by a mixture of two multi-variate Gaussian distributions, whose means have to lie within the capture range of the two local basal ganglia maxima. The capture range of a local maximum is defined by the set of points in space which will lead to the local maximum when used as starting points of a gradient ascent search on the activity level. As our results show these assumptions are fulfilled by all the investigated test data sets from different centres.
Finally, the data analysis involves the fully automatic localization of the basal ganglia and a reference region in the occipital region, yielding a relative activity measure for each basal ganglion. The occipital region was chosen as reference region because it is least affected by neurodegenerative PSs due to its very low dopamine receptor density compared with that of the striatum.
To perform the localization step, the mean values of the two Gaussian distributions need to be estimated. This can be performed by EM that yields the means and covariance matrices with maximum likelihood of explaining the data. For each of the estimated means, the local maximum corresponding to the basal ganglion in question is found by performing a gradient ascent search on the activity (Fig. 1).

3D localization of basal ganglia and reference region. Axes represent number of pixels. Blue right basal ganglion, green left basal ganglion, red reference region
To obtain a more flexible measurement than the single values as by other methods, border definition for ROIs were set to 90, 80 and 70% of maximum activity. The median is computed for each of these regions, resulting in median values of the basal ganglia with different thresholds of 70–90% of the maximum activity, respectively (Fig. 2).

Basal ganglia to occipital ratio for left and right side. Each circle represents the ratio in a respective threshold
The median value of the reference region provides the reference value against which the calculated values of the basal ganglia were compared (Fig. 1).
The approach was evaluated on 12 data sets obtained from multiple centres including three anthropomorphic striatal phantom measurements. The acquisition parameters were defined to be the same in all centres. A dual-head gamma camera (GE, Hawk Eye, Haifa, Israel/Siemens, e.cam, USA) was used with fan beam collimator and acquisition was done in every 3° in a 360 arc. Time per view was 30 s and images were stored in a 128 × 128, word mode matrix. Images were reconstructed by iterative reconstruction (8 iterations, 2 subsets). Chang’s method (μ = 0.11 cm−1) was used for attenuation correction. The data set of each of the nine patients and of the three anthropomorphic striatal phantoms (one normal and two abnormal) were manually analysed twice by the same investigator. Furthermore, these data sets were automatically assessed by the present proposed 3D method (Spectalyzer) and also by commercially available software (BRASS, Version 3.5, Hermes, Sweden).
A number is assigned to each patient and the name of the patient is cleared from the data for protection of privacy. All patients were informed and gave their written consent for the study.
Results
We studied nine patients as well as three phantoms (1 normal and two abnormal phantoms). Three methods of manual ROI, BRASS and Spectalyzer were applied for calculation of striatum to occipital activity ratio. In each method, radiotracer activity in striatum as well as in occipital region was measured and the ratio of striatum to occipital region (St/Oc) was recorded. For manual method two sets of drawing was used and the mean activity was recorded. One of the patients was excluded due to the fact that BRASS software was unable to define the striatum. In another patient, Spectalyzer was unsuccessful in defining the occipital area. Ten images were analysed.
Descriptive analysis showed that the mean St/Oc ratio was 3.4(±0.56) in the right and 3.5(± 0.5) in the left for manual method. Using BRASS software the mean ratio was 2.8(±0.46) and 2.9(±0.51) for the right and left striatum, respectively. Using “Spectalyzer” the ratio was calculated with three thresholds of 70, 80 and 90% of maximum activity for border definition. The mean ratio was 3.3(±0.42), 3.6(±0.47) and 3.9(±0.5) for the 70, 80 and 90%, respectively, in the right striatum. For the left striatum, the ratio was 3.3(±0.5), 3.6(±0.47) and 3.8(±0.51), respectively, for 70, 80 and 90%.
Using Kolmogorov–Smirnov test, normal distribution of the data in the studied group was confirmed (P > 0.4) in all sets. The relationship between St/Oc ratio between different methods was investigated using Pearson product–moment correlation coefficient. Preliminary analysis was performed to ensure no violation of the assumptions of normality, linearity and homoscedasticity. There was a strong positive correlation between the St/Oc ratio in “manual method” compared with “Spectalyzer” with all thresholds (r > 0.72, n = 10, P < 0.02). Also correlation between “Spectalyzer” and BRASS software was strong and significant (r > 0.89, n = 10, P < 0.001).
One-way repeated measures ANOVA was conducted to compare mean ratios in manual, BRASS and “Spectalyzer” (80% threshold) methods. The measures and standard deviations are presented in Table 1. The ratio was significantly different between different techniques [Wilks’ λ = 0.0.04, F[2, 7] = 92.54, P < 0.001, partial η 2 = 0.96].
As expected increasing the thresholds of border definition from 70 to 90% of maximum activity in “Spectalyzer” results in increasing of St/Oc ratios (Fig. 2).
Further analysis showed that the mean St/Oc ratio was significantly lower in BRASS method compared with manual or Spectalyzer (P < 0.02), but there was no significant difference between manual and Spectalyzer. This is due to the different calculation methods used; BRASS subtracts the values of background activity from basal ganglia and then divides by the background, whereas the manual method and Spectalyzer divide the mean/median activity in the basal ganglia to the background (Fig. 3).

Scatter plot of striatum to occipital ratio in Manual vs BRASS (triangles, solid trend line), Spectalyzer vs BRASS (open circles, dashed trend line) and Manual vs Spectalyzer (solid circles, trend line: dashed and points) methods
Mean running time for Spectalyzer using a usual laptop computer (Siemens, Fujitsu, 2 GHz) was 42 s.
Discussion
DaTSCAN is a commonly used investigation method in the differential diagnosis of movement disorders as well as in clinical trials. In this manuscript, a new fully automated tool for the processing, evaluation and documentation of DaTSCAN is presented.
In SPECT the radiotracer binding in certain regions of the brain is usually assessed by manual positioning of ROIs. Usually, for quantification a ratio analysis of specific radiotracer binding in a certain brain region to a non-specific binding area is performed. The disadvantages of this method are twofold: it is investigator-dependent and time consuming. Therefore, a fully automated technique for semiquantitative evaluation of the DaTSCAN results will be very useful.
It is known that quantification is mandatory to assess striatal DAT binding [8]. On the other hand, the different calculation methods and also different reconstruction process algorithms affect the quantification output. These effects include scatter, partial volume effect and attenuation. Different approaches, such as with Monte Carlo simulation, have been applied to overcome these issues [9, 10].
In our approach, the software uses already reconstructed transaxial data. Therefore, the different reconstruction algorithms by various manufacturers should be kept in mind in order to compare the results of studies obtained from different centres.
Moreover, our method is user-independent, because the ROIs are found fully automatically in a 3D manner. There is therefore no intra- or interobserver variability and furthermore our method is time-saving. This program can easily run on a PC computer and it takes less than a minute for each analysis.
Additionally, the curves with different maximum expectation enable the clinician to be quickly aware of possible artefacts which would yield to a truncation of the curve shape. A limitation of the study is that the algorithm actually encloses the whole striatal area and does not delineate caudate from putamen. From previous studies it is known that reductions in tracer uptake are not homogeneous within the striatum. Particularly in LBD and PD, a significant decreased tracer uptake in posterior putamen and caudate but a normal tracer uptake in the anterior putamen [11] was found.
Fusion imaging, performing additional CT or MR imaging, is helpful to more accurately define the striatal region when manually positioning the ROIs. Nevertheless this method is elaborate and expansive. With our proposed fully automated approach, 3D ROIs are positioned fully automatically without the need to perform additional processing, leading to a high cost-effectiveness and significant time saving.
The SPECT studies used in the evaluation of the proposed software tool were obtained from different centres using different cameras. Nevertheless, the proposed technique was successful in exactly finding the required 3D ROIs and performing subsequent activity measurements showing that the software tool can be used by different centres without any special preparations. Experiences from different participating centres share the feasibility and user-independent reproducible semiquantitative results in the analysis of DAT studies. Activity maxima in DaTSCAN of the basal ganglia are found automatically by the programme without additional required MRI or CT and the result can easily be read on a curve.
The usual manual positioning of ROIs in 2D SPECT slices for the quantification of dopamine uptake is time-consuming and limited by inter- and intra-individual variability of the investigator. Spectalyzer programme is easy to apply and shows a very high reproducibility with no need to adopt the received data or to perform further manual analysis. Furthermore, the programme can be directly applied with routinely received SPECT datasets. No training for users is required and also no additional MRI or CT data are needed as a template. The Spectalyzer method is successful in finding 3D ROIs and in performing subsequent activity measurement automatically. The activity distribution can be easily read on a curve which is processed automatically leading to a quick understanding of the results by the clinician. Moreover, the method is user-independent and was successfully compared with manually obtained values in the same subjects as well as to an anthropomorphic striatal phantom showing reproducible results.
Limitations of the study: Spectalyzer has a limitation of inability to differentiate between the head of caudate and putamen. Another limitation of our study was absence of final clinical diagnosis in patients. Further study in a large group of patients and correlation with final clinical diagnosis will better clarify the accuracy of Spectalyzer.
Conclusion
We introduced Spectalyzer which is an automatic, highly reproducible and observer-independent software for 3D region of interest determination in DAT scan. We suggest this new technique as an alternative approach for semiquantitative analysis of DAT scintigraphy. With respect to reproducibility and observer independency, it may play an important role either in comparing serial images of a patient or in clinical trials.
References
Booij J, Speelman JD, Horstink MW, Wolters EC. The clinical benefit of imaging striatal dopamine transporters with [123I]FP-CIT SPECT in differentiating patients with presynaptic parkinsonism from those with other forms of parkinsonisms. Eur J Nucl Med. 2001;28:266–72.
Van Laere K, Everaert L, Lieven A, Gonce M, Vandenberghe W, Vander Borght T. The cost effectiveness of 123I-FP-CIT SPECT imaging in patients with an uncertain clinical diagnosis of parkinsonism. Eur J Nucl Med. 2008;35:1367–76.
Booij J, Tissingh G, Winogrodzka A, vam Royen EA. Imaging of the dopaminergic neurotransmission system using single-photon emission tomography and positron emission tomography in patients with parkinsonism [review]. Eur J Nucl Med. 1999;26:171–82.
Marshall V, Grosset D. Role of dopamine transporter imaging in routine clinical practice [review]. Mov Disord. 2003;18:1415–23.
Wolters EC, Francot C, Bergmans P, Winogrozka A, Booij J, Berendse HW, et al. Preclinical (premotor) Parkinson’s disease. J Neurol. 2000;247(Suppl 2):II103–9.
Walker Z, Costa DC, Walker RW, Shaw K, Gacinovic S, Stevens T, et al. Differentiation of dementia with Lewy bodies from Alzheimer’s disease using a dopaminergic presynaptic ligand. J Neurol Neurosurg Psychiatry. 2002;73:134–40.
McKeith I, O’Brian J, Walker Z, Tatsch K, Booij J, Darcourt J, et al. Sensitivity and specificity of dopamine transporter imaging with 123-I-FP-CIT SPECT in dementia with Lewy bodies: a phase III, multicentre study. Lancet Neurol. 2007;6:305–13.
Tatsch K, Asenbaum S, Bartenstein P, Catafau A, Halldin C, Pillowsky LS, et al. European Association of Nuclear Medicine procedure guidelines for brain neurotransmission SPET using 123I-labelled dopamine transporter ligands. Eur J Nucl Med. 2002;BP29:30–5.
Cot A, Falcón C, Crespo C, Sempau J, Pareto D, Bullich S, et al. Absolute quantification in dopaminergic neurotransmission SPECT using a Monte Carlo-based scatter correction and fully 3-dimensional reconstruction. J Nucl Med. 2005;46:1497–504.
Beekman FJ, de Jong HWAM, Geloven S. Efficient fully 3-D iterative SPECT reconstruction with Monte Carlo-based scatter compensation. IEEE Trans Med Imaging. 2002;21:867–77.
Colloby SJ, Williams ED, Burn DJ, Lloyd JJ, McKeith IG, O’Brien JT. Progression of dopaminergic degeneration in dementia with Lewy bodies and Parkinson’s disease with and without dementia assessed using 123I-FP-CIT SPECT. Eur J Nucl Med Mol Imaging. 2005;32:1176–85.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mirzaei, S., Zakavi, R., Rodrigues, M. et al. Fully automated 3D basal ganglia activity measurement in dopamine transporter scintigraphy (Spectalyzer). Ann Nucl Med 24, 295–300 (2010). https://doi.org/10.1007/s12149-010-0353-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-010-0353-2