
Abstract
Emerging adults’ religiosity has been consistently linked with less participation in sexual behaviors as supported by cognitive dissonance theory. However, this association may be different when examining centrality of religiosity of relationships (CRR), meaning participating in and discussing religiosity and spirituality with a current or anticipated romantic partner. The goal of this study is to examine the influence of CRR for emerging adults’ affectionate and sexual behaviors. Additionally, we test if the association between CRR and affectionate and sexual behaviors varies by gender, given males’ more positive attitudes towards sexual behaviors compared to females. Data for this study comes from 284 emerging adults, ages 18 to 29 (mean age = 20.9 years; 70.1% female) from an area in the Midwestern United States. Results illustrated that CRR is negatively associated with affectionate behaviors, intimate touching behaviors, oral sex behaviors, and sexual (vaginal) intercourse. Additionally, gender significantly moderated these relationships. Male participants reporting low levels of CRR conveyed significantly higher participation with these sexual behaviors compared to males reporting high levels of CRR, whereas CRR did not appear to significantly alter female participants’ engagement with these sexual behaviors. These findings provide some evidence that CRR contributes to males’ romantic development and that CRR may increase intimacy in females’ romantic relationships, which could promote sexual activity. Other implications for religious and sexual development are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Discussing and learning about religious beliefs as well as participating in religious activities and groups contributes to the sexual socialization of emerging adults, which are defined as those individuals who are between the ages of 18 and 29 (Arnett 2000; LeJeune et al. 2013). Consistently, studies have shown a negative correlation between religiosity and sexual behaviors, particularly among adolescents and emerging adults (Kirk and Lewis 2013; Young et al. 2015; Vasilenko and Lefkowitz 2014). However, most studies focus on individual religiosity with reliance on single-item measures (i.e., “How religious are you on a scale of 1 = not at all to 7 = very?”) to investigate the relationship between religiosity and sexual behaviors. Given the importance of forming romantic relationships during emerging adulthood (Arnett 2000), it is important to examine the significance of centrality of religiosity of relationships (CRR), meaning participating in and discussing religiosity and spirituality with one’s current or anticipated romantic partner, for emerging adults’ sexual development. Although emerging adults reporting high levels of religiosity are less likely to participate in sexual activities (Rostosky et al. 2003; Hull et al. 2011; Vasilenko and Lefkowitz 2014), the experience of religiosity with a potential or current romantic partner (i.e., a high level of CRR) may further inhibit participation in sexual behaviors (LeJeune et al. 2013).
According to cognitive dissonance theory (Festinger 1962), individuals want their behaviors to be consistent with their beliefs, meaning that religious individuals may participate in fewer sexual behaviors to be in concordance with their religious views. Individuals who experience high levels of religiosity in their current or anticipated romantic relationships may be even less likely to engage in sexual behaviors compared to individuals whom report lower levels of CRR. High levels of CRR reflect a dyadic focus on religiosity, which should prompt greater refrainment from sexual behaviors to be consistent with religious beliefs. Yet, there may be gender differences regarding the relationship between CRR and participation in sexual behaviors. For example, CRR may predict more declines in sexual behavior for women than men, as men are more comfortable engaging in sexual behaviors and usually desire sex more compared to women (Baumeister and Vohs 2004; Vohs et al. 2004). Therefore, the goal of this study is twofold. First, we examine the influence of CRR for sexual behaviors. Second, we test if gender may moderate this relationship, which allows us to see if the relationship between CRR and sexual behaviors is different based on gender.
Religiosity and Sexual Behaviors
The literature on sexual behaviors and religiosity for adolescents and young adults is relatively consistent, demonstrating a negative association between individual religiosity and sexual behaviors (Rostosky et al. 2003; Cotton et al. 2010; Hull et al. 2011). Primarily, researchers have provided empirical evidence that illustrates that increases in individual religiosity are associated with delayed sexual intercourse initiation for adolescents and emerging adults (Hardy and Raffaelli 2003; Vasilenko and Lefkowitz 2014). For example, Kirk and Lewis (2013) found that increases in individual religiosity were associated with fewer sexual partners and less premarital sexual activity. Rostosky et al. (2003) demonstrated that religiosity was linked to reductions in the likelihood of losing one’s virginity for both male and female adolescents. Besides the negative association between religiosity and sexual intercourse initiation, studies have also found a negative association between religiosity and general sexual behaviors. For instance, attending religious services, at least occasionally, was related to refraining from a variety of sexual behaviors, such as light (touching over one’s clothes) and heavy petting (touching under one’s clothes; Hull et al. 2011). Another study found that those who attended church more frequently were less likely to have experienced oral sex (Davidson et al. 1995). Yet, another explanation for why individuals refrain from sexual behaviors is because they are anxious about health risks, such as unplanned pregnancy or sexually transmitted infections, and some view certain sexual behaviors as unclean.
Subsequently, some studies have illustrated that participating in sexual intercourse is linked to declines in religiosity and church attendance. Vasilenko and Lefkowitz (2014) found that 6 months after first sexual intercourse, college students reduced their attendance in religious services, and 12 months after first sexual intercourse, participants reported declines in the importance of religiosity. For this specific study, attendance in religious services was measured using one item, which asked participants how often they went to religious services during the past 12 months. Importance of religion was measured using an established scale from Rohrbaugh and Jessor (1975), which is a 7-item measure that asks about the importance of various religious topics, such as prayer, help with personal problems, and influence on daily life. To elaborate on these findings to provide context for the current study, after losing one’s virginity, participants rated religiosity as less important for their daily lives.
Theoretically, the negative correlation between religiosity and sexual behaviors is consistent with cognitive dissonance theory (Festinger 1962). According to this theory, individuals seek consistency between their behaviors and their beliefs. Many religions, particularly in the United States, discourage sexual behaviors, especially sexual intercourse. For example, according to the Catholic faith, which represents approximately 20% of the U.S. population (Pew Research Center 2017), engaging in sex before marriage is highly discouraged. Thus, for many emerging adults, engaging in sexual intercourse and other sexual behaviors would promote psychological distress for those reporting high levels of religiosity since their behaviors would be discordant with their beliefs. Additionally during emerging adulthood, individuals are attempting to explore their identity (Arnett 2000), which may involve examining their religious and sexual identity. According to Arnett’s theory of emerging adulthood (2000), in order to promote identity development, emerging adults experience romantic relationships. Consequently, emerging adults may explore their religious and sexual identities through participation in romantic relationships. Therefore, participating in religious activities with potential or current romantic partners may be likely to influence participation in various sexual behaviors. For the current study, we focus on the religious experiences that an individual shares with a current or potential romantic partner, referred to as CRR.
Despite the findings regarding the negative association between sexual behaviors and religiosity for emerging adults, there are limitations to past studies that the current research can improve on. First, many studies focus on first sexual intercourse and risky sexual behaviors, as opposed to more general sexual behaviors that coincide with emerging adult development, such as kissing, intimate touching, and oral sex (Collins et al. 2009; Langlais et al. 2010). Also, studies examining sexuality and religiosity dichotomize sexual behaviors to whether or not participants engaged in the sexual behavior (i.e., “Yes” or “No”), rather than capture the frequency of participating in sexual behaviors. The current study examines a variety of sexual behaviors ranging in frequency, both within and outside committed romantic relationships. Second, past studies examining religiosity and sexual behaviors commonly used single-item measures of religiosity. For example, a single item such as “How religious do you consider yourself to be?” is asked with Likert scale responses (i.e., 1 = not at all, 7 = very much). Other studies have used proxy measures for religiosity, such as asking about the frequency of church attendance or prayer. An examination of dyadic religious activities and behaviors, particularly regarding sexual behaviors, is ostensibly absent in the literature. To build on these limitations, the current study uses the centrality of religiosity scale (Huber and Huber 2012) in the context of anticipated or current relationships in order to capture the influence of dyadic religious experiences for emerging adults’ participation in a variety of sexual behaviors.
Centrality of Religiosity
Centrality of religiosity is a precise measure of the importance of religious meanings for individuals’ religious experiences and identity (Huber and Huber 2012). Huber and Huber (2012) created the measure of centrality of religiosity, which identifies five dimensional measures to examine individual religiosity: intellect (e.g., How interested are you in learning more about religious topics?), ideology (e.g., To what extend do you believe that god or something divine exists?), public practice (e.g., How important is it for you to be connected to a religious community?), private practice (e.g., How often do you try to connect to the divine spontaneously when inspired by daily situations?), and experience (e.g., How often do you experience situations in which you have the feelings that you are touched by a divine power?). This scale is an in-depth examination of religiosity that has been used over 100 times in 25 different countries across the world, providing evidence of its validity (Stiftung 2009). Because this scale provides an in-depth, precise illustration of religiosity, this measure provides a framework for capturing CRR. For example, individuals may engage with these various dimensions of religiosity with their current or potential romantic partners, which should also impact religious development, and potentially sexual development.
In the current study, we adapted Huber and Huber’s (2012) centrality of religiosity scale to capture CRR. We define CRR as engaging in religious activities with potential or current romantic partners, such as attending religious services together, discussing religious topics together, reading holy texts together, and connecting with one another religiously. We use all items from Huber and Huber’s (2012) centrality of religiosity scale and apply them to a dyadic perspective, whether it’s a current or potential romantic partner. For example, “How often do you pray?” reads “How often do you pray with a potential or current romantic partner?” There is evidence that engaging in dyadic religious activities is beneficial for relationships. For instance, Fincham et al. (2011) found that couples who were actively engaged in their faith communities reported higher quality relationships. However, few studies have examined how engaging in dyadic religious activities influences participation in sexual behaviors. Although there is data that connects dyadic religiosity to first sexual intercourse (McCree et al. 2003; Steinman and Zimmerman 2004), emerging adults engage in other sexual behaviors, such as affectionate behaviors, which is characterized by kissing and making out, intimate touching behaviors, such as light and heavy petting, and oral sex behaviors. CRR is likely to have varied effects depending on the sexual behavior. For instance, engaging in religious activities with a potential or current romantic partner may increase intimacy promoting affectionate behaviors. Feeling close with a romantic partner is associated with more hand holding, hugging, and kissing (Sternberg and Weis 2006). On the other hand, experiencing high levels of religiosity in potential or current romantic relationships may assuage participation in more sexual behaviors, such as intimate touching and oral sex. Participating in these sexual behaviors may be inconsistent with their religious beliefs, which is congruent with cognitive dissonance theory. Therefore, we propose the following hypotheses:
Hypothesis 1a
Centrality of religiosity of relationships will be positively associated with affectionate behaviors (kissing and making out).
Hypothesis 1b
Centrality of religiosity of relationships will be negatively associated with sexual behaviors (intimate touching, oral sex, and sexual [vaginal] intercourse).
Gender and Sexual Behaviors
Although CRR is likely to be negatively associated with sexual behaviors, there may be gender differences regarding these effects. For instance, male emerging adults are more likely to describe that they engaged in sexual intercourse, whereas female emerging adults are less likely to describe participation in sexual intercourse, regardless if it is true (Gute et al. 2008). Additionally, males have more positive attitudes towards casual sex and sexual behaviors in general compared to women (Vohs et al. 2004; Petersen and Hyde 2011). Therefore, it may be likely that CRR would contribute less to males’ participation in sexual behaviors than females. Yet, it is important to note that as both men and women mature emotionally and intellectually, it is natural that many may lessen casual sexual encounters in order to avoid the dangers associated with casual sex, regardless of religiosity.
There is some evidence for gender differences regarding the association between sexual behaviors and religiosity. One study found that women were more likely to participate in regular religious practices than men and participation in these practices was significantly associated with delaying first sexual intercourse (Moreau et al. 2013). Young et al. (2015) found that highly religious males reported lower participation in sexual and oral intercourse and highly religious females reported lower participation in sexual, oral, and anal intercourse. Additionally, women who attend church more frequently were more likely to have fewer lifetime sex partners than men, and were more likely to view masturbation as unhealthy and as a sin compared to men (Davidson et al. 1995). Adolescent females who reported high levels of religiosity delayed losing their virginity relative to their non-religious peers, but this finding was not found for adolescent males (Rostosky et al. 2003). Again, it is also likely that these results may be an outcome of avoiding sexual behaviors due to the risks of unplanned pregnancies and sexually transmitted diseases. But for the current study we believe that the influence of religiosity may be gender specific, where CRR may exhibit greater influence on the sexual behaviors of female emerging adults than male emerging adults. Based on this information, we proffer the following hypotheses:
Hypothesis 2a
Gender will moderate the relationship between CRR and affectionate behaviors (kissing and making out).
Hypothesis 2b
Gender will moderate the relationship between CRR and sexual behaviors (intimate touching, oral sex, and sexual intercourse).
Methods
Participants
Data for this study comes from an online survey of emerging adults from a region in the Midwestern United States. Participants were recruited through advertisements on local Facebook pages associated with the city of recruitment, which resulted in a sample of 318 participants. Since the focus on the current study is emerging adults, 34 participants were dropped from the recruited sample as they were 30 years of age or older, resulting in a sample of 284 participants for the current investigation. Descriptive statistics for this sample are presented in Table 1. Participants were predominantly female (70.1%) and approximately 20.85 years old (Range: 18–29; SD = 1.88). Ethnic composition for participants was 93.0% White/Caucasian, 4.2% Hispanic, 1.4% Black/African American, 1.1% Asian/Pacific Islander, and 0.3% were American Indian. The average education for participants in the current study was a sophomore in college (Range: high school degree to graduate degree). These demographic statistics are representative of the area in which participants were recruited.
For the current study, 149 participants were single, 26 were casually dating, 90 were seriously dating, and 19 were married. For those in romantic relationships, the average length of relationship was 25.60 months (Range: 1–144 months; SD = 25.14). Additionally, we tested for significant differences between participants reporting on potential romantic partners and participants reporting on current romantic partners using independent t-tests. These tests are commonly used to see if there are significant differences across groups; in this case, there are two groups: single participants and partnered participants. Each analysis results in an F score; based on the size of this score, a probability (p-value) is simultaneously calculated, which would signify if there is a significant difference by group for a specific variable. Probabilities that are less than 5% (.05) are considered statistically significant. There were significant differences according to frequency of sexual behaviors. Participants in committed relationships were significantly more likely participate in kissing behaviors [F (2, 283) = 89.80, p < .001], intimate touching behaviors [F (2, 283) = 87.17, p < .001], oral sex behaviors [F (2,283) = 36.22, p < .001], and sexual (vaginal) intercourse [F (2, 283) = 60.77, p < .001]. However, there were no significant differences for any demographic variables or measure of religiosity. Because there were no differences for independent variables, we analyzed coupled and single participants together to increase power for analyses.
Procedures
Advertisements for the study were posted in local Facebook pages associated with the city of recruitment. These advertisements briefly described the goal of the study and the requirement for participation (participants had to be at least 18 years of age). At the end of the advertisement, a hyperlink was provided that directed interested participants to a webpage that displayed the informed consent form for this study. At the bottom of this page was a button that said “I Agree,” referring to the informed consent form. Informed consent was obtained from all individual participants included in this study. Selecting this option directed participants to the online survey, which was hosted by Qualtrics (2017). This online survey assessed CRR, frequency of engaging in affectionate behaviors, intimate touching behaviors, oral sex behaviors, and sexual (vaginal) intercourse as well as other items not pertaining to the current investigation. The survey took about 30 min to complete and participants were not compensated to complete the study. The current investigation was approved by the appropriate Institutional Review Board.
Measures
Centrality of Religiosity of Relationships (CRR)
CRR was measured using an adapted version of the centrality of religiosity scale (Huber and Huber 2012). This scale was composed of 15 items, such as “How often do you talk about religious issues with a current or potential romantic partner?” and “How interested are you in learning about religious topics with a current or potential romantic partner?” with responses ranging from 1 (Not at all) to 5 (Very much so). Prior to answering these questions, participants were asked to recall their current romantic partner, or a romantic partner with whom they would want to form a romantic relationship with. Although an option was provided that allowed participants to skip this section if they did not have a current relationship or a potential romantic partner, no participants selected that option. The scale demonstrated acceptable internal consistency (Cronbach’s alpha = .95) and the average level of CRR was 2.57 (Range: 1–5; SD = 1.02).
Sexual Behaviors
Sexual behaviors was captured through frequency measures of the following four behaviors: affectionate behaviors, intimate touching behaviors, oral sex behaviors, and sexual (vaginal) intercourse. Affectionate Behaviors was measured using two items: How often have you participated in the following behaviors?: Kissing (brief kissing on the lips; not French kissing or making out) and French kissing (making out). Intimate Touching Behaviors was measured using an average of four items: How often have you participated in the following behaviors?: Intimately touching over someone else’s clothes; being intimately touched over your clothes; intimately touching under someone else’s clothes; and being intimately touched under your clothes. Oral Sex Behaviors was measured using the average of two items: How often have you participated in the following behaviors?: Performing oral sex and receiving oral sex. Sexual Intercourse was measured using a single item, “How often have you engaged in vaginal intercourse?” Responses for all items ranged from 1 (never) to 6 (daily). Averages for each measure of affectionate and sexual behavior are presented in Table 1.
Control Variables
For all analyses, we controlled for age, education, sexual orientation, ethnicity, and relationship status as previously mentioned. Sexual orientation and ethnicity were both dichotomized for interpretation. For instance, sexual orientation was dichotomized as heterosexual = 1, other sexual orientation = 0; ethnicity was dichotomized as white = 1, other ethnicity = 0. Participants answered the following question regarding educational status, “What best describes your educational status?” with responses ranging from less than high school (1) to graduate degree (10).
Analytic Approach
Data was analyzed using multiple regression analyses. This approach allows us to investigate the relationship with multiple predictor variables for a dependent variable to see which variables contribute to changes in the dependent variable. This approach also provides the opportunity to control for various factors and to insure that changes in the dependent variable are a result of the predictor variables, rather than the control variables. Therefore, for each model, control variables were entered in Step 1 (age, education, sexual orientation, relationship status, and ethnicity) and independent variables were entered in Step 2 (CRR, gender, and CRR x gender). For the first hypothesis, only CRR was included as a predictor in Step 2. For the second hypothesis, CRR, gender, and the interaction of the two were included as predictors in Step 2. For these regression analyses, to determine if gender moderates the relationship between CRR and sexual behaviors, an interaction is used; if the interaction term is significant, than there are likely gender differences between CRR and sexual behaviors (Aiken and West 1991). For all models, changes in R 2 were measured from Step 1 to Step 2 to capture variance explained beyond the control variables, which is common in regression analyses (see Langlais and Schwanz 2017, for an example).
Results
Prior to conducting analyses for the current study, we examined mean differences by gender by conducting independent t-tests, as one of the goals of the study involved an examination of gender. Results of these analyses are presented in Table 1. There were no gender differences based on descriptive characteristics of the sample, including age, education, ethnicity, and relationship status. Additionally, individual religiosity and CRR did not vary by gender; however, for those in romantic relationships, perception of romantic partner’s religiosity varied. Male participants perceived their romantic partners to be more religious than female participants [F (2, 283) = 15.40, p < .001]. There were also significant gender differences according to affectionate and sexual behaviors. Female participants reported more frequent affectionate behaviors [F (2, 283) = 9.21, p < .01], intimate touching behaviors [F (2, 283) = 5.53, p < .05], and sexual (vaginal) intercourse [F (2, 283) = 6.47, p < .05] compared to male participants. There were no gender differences regarding oral sex behaviors.
The first hypothesis of the current study predicted that CRR would be positively associated with affectionate behaviors, but negatively associated with sexual behaviors. Results for this hypothesis are presented at the top of Table 2. CRR was not associated with affectionate behaviors, intimate touching, or sexual (vaginal) intercourse. However, CRR was negatively associated with oral sex behaviors. The variance explained by including CRR for each of these models ranged from 0% (affectionate behaviors and intimate touching behaviors) to 3.6% (oral sex behaviors).
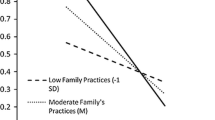
The second hypothesis predicted that gender would moderate the relationship between CRR and affectionate and sexual behaviors. Results for this hypothesis are presented in the bottom of Table 2. First, CRR and gender were negatively associated with affectionate behaviors, whereas the interaction of the two were positively associated with affectionate behaviors. According to this analysis, CRR was associated with fewer affectionate behaviors and men were less likely to engage in these behaviors than women. The significant interaction term illustrates that gender moderates the relationship between CRR and affectionate behaviors. This moderation is displayed in Fig. 1. Based on this figure, male and female participants report different amounts of affectionate behaviors according to CRR. Males reported relatively similar levels of affectionate behaviors regardless of CRR, whereas women who reported low levels of CRR reported fewer affectionate behaviors compared to women reporting high levels of CRR. The variance explained by adding the predictor variables in this model was 16.2%. In other words, CRR appears to explain 16.2% of participation in affectionate behaviors.

Interaction for centrality of religiosity of relationship and affectionate behaviors
Next, CRR and gender were negatively associated with intimate touching behaviors and oral sex behaviors. These results illustrated that CRR was associated with fewer sexual behaviors and that men were less likely to engage in these behaviors than women. Additionally, the interactions between gender and CRR for intimate touching (Fig. 2) and oral sex behaviors (Fig. 3) were significant. These interactions displayed a similar pattern. For male participants, high levels of CRR was predictive of fewer intimate touching and oral sex behaviors compared to male participants reporting low levels of CRR. Generally, CRR did not appear to alter females’ participation in intimate touching and oral sex behaviors. The variance explained by the predictor variables was 14.4% for intimate touching and 13.2% for oral sex behaviors.

Interaction for centrality of religiosity of relationship and intimate touching behaviors

Interaction for centrality of religiosity of relationship and oral sex behaviors
Next, CRR was negatively associated with sexual (vaginal) intercourse. Additionally, the interaction between gender and CRR was significant for sexual intercourse. The moderating effect of gender is displayed in Fig. 4. According to this model, male participants experiencing high levels of CRR reported lower levels of sexual intercourse compared to male participants reporting low levels of CRR. There appeared to be minimal differences concerning frequency of sexual intercourse among female participants reporting high and low levels of CRR. Although the projected scores of sexual intercourse are low, participants reported an average frequency of engaging in sex a few times a month, meaning that CRR didn’t appear to influence females’ participation in sexual intercourse, but did appear to prohibit males’ participation in sexual intercourse. The variance explained by the predictor variables in this model was 11.3%.

Interaction for centrality of religiosity of relationship and intimate touching behaviors
Discussion
The current study illuminates on the relationship between religiosity and sexual behaviors for emerging adults. Where previous studies focused primarily on individual religiosity, the current study adapted Huber and Huber’s (2012) centrality of religiosity scale in the context of romantic relationships to understand how CRR influences emerging adults’ participation in various sexual behaviors. According to Arnett’s (2000) theory of emerging adulthood, emerging adults are exploring their identity through participation in romantic relationships, which is likely to simultaneously impact sexual and religious identity development. The results of this study reveal a negative association between CRR and affectionate behaviors, intimate touching behaviors, oral sex behaviors, and sexual intercourse. However, these findings were different based on gender. CRR contributed more towards female participants’ participation in affectionate behaviors than male participants. For intimate touching behaviors, oral sex behaviors, and sexual intercourse, CRR contributed more towards male participants’ participation in these activities than female participants. In the following discussion, we will discuss the importance of CRR in terms of emerging adult development and implications for gender.
First, CRR influences sexual behaviors. The current study used a stringent measure of religiosity, which measured the importance and frequency of engaging in religious activities with potential and current romantic partners. Although the results for the first hypothesis demonstrated that CRR was not related to participation in affectionate and sexual behaviors, asides from oral sex behaviors, the results of the second hypothesis illustrated that CRR was negatively associated with affectionate and sexual behaviors. These findings are consistent with cognitive dissonance theory (Festinger 1962), which explains that individuals want their behaviors to be in accord with their thoughts and beliefs. In the context of this study, religious individuals are less likely to engage in sexual behaviors because it would be inconsistent with their cognitive processes, as sexual intercourse and other sexual behaviors are discouraged according to most religions in the United States (Benokraitis 2011). When individuals rate religiosity as important, either for their self or for the development of interdependence in their romantic relationships, sexual behaviors may seem less important or counterproductive to their religious development. In other words, participating in sexual behaviors may distract from religious identity development or the development of religiosity within a romantic relationship. Yet, it can be noted that avoidance of these sexual behaviors during this development period may also be attributed to anxieties of sexually transmitted infections, unplanned pregnancies, or other risks associated with sexual behaviors.
Additionally, if individuals report high levels of religiosity in their current or anticipated romantic relationships, they may seek a religious connection during the development of their romantic relationships rather than sexual compatibility. During emerging adulthood, there is a concerted focus on the development and maintenance of romantic relationships (Arnett 2000), which may not always involve exploration or participation in sexual behaviors (Langlais et al. 2010). Developing a religious connection with a romantic partner promotes relationship maintenance, which is important for emerging adults, as dyadic religiosity is linked to relationship stability and commitment (Lambert and Dollahite 2008; Ellison et al. 2010).
For the current study, gender played a significant role in how CRR influenced participation in various sexual activities. High levels of CRR was associated with more affectionate behaviors, especially for female participants. For sexual behaviors (intimate touching, oral sex, and sexual intercourse), CRR had varied effects for males, but not females. Male participants reported fewer sexual behaviors when they reported high levels of CRR, whereas CRR varied little in terms of frequency of sexual behaviors for female participants. Yet, for both genders, high levels of CRR was associated with decreased levels of sexual behaviors compared to participants reporting low levels of CRR.
Although we predicted gender to moderate the relationship between CRR and sexual behaviors, the direction of this influence was in a different direction than expected. Though males are more likely to report a positive attitude towards casual sex and sexual behaviors generally (Vohs et al. 2004; Petersen and Hyde 2011), results of the current study illustrated that male participants exhibited a negative attitude towards sexual behaviors when they reported high levels of CRR. This finding is consistent with cognitive dissonance theory, as male emerging adults may refrain from engaging in sexual behaviors in order to be consistent with their religious beliefs to prevent psychological distress. For males reporting high levels of CRR, discussing and participating in religious activities with potential or current romantic partners may contribute more significantly to individual and romantic development than participation in sexual behaviors. Male participants who seek religious compatibility in their romantic relationships may focus more on religious development than sexual development during emerging adulthood. Another explanation could be that as males mature emotionally and intellectually during this period, it may be likely that they avoid sexual encounters due to awareness of the risks associated with sexual behaviors.
On the other hand, female participants reported similar levels of intimate touching, oral sex behaviors, and sexual intercourse regardless of the reported level of CRR. Females in the current study did not appear to experience as much cognitive dissonance regarding sexual behaviors compared to males. There are a few explanations that may explain this finding. First, females often develop their religiosity earlier in life compared to males (Deaton 2009; Benokraitis 2011), meaning that by emerging adulthood females’ religious identity may already be formed. Therefore, females may focus more on sexual identity formation as opposed to religious identity formation during emerging adulthood. Second, female participants in this study reporting high levels of CRR may be in relationships with partners who are not religious. Individuals who are not religious, particularly males, engage in more sexual behaviors than those who report high levels of individual religiosity (Rostosky et al. 2003; Cotton et al. 2010; Hull et al. 2011). In these cases, females may find opportunities to talk about and experience religiosity with less religious potential or current romantic partners, but these partners may also encourage or seek more frequent sexual behaviors. Females in these situations may experience cognitive dissonance after participating in sexual behaviors that may impair psychological well-being. Future research is needed to examine reports of CRR from both partners in order to understand the relationship between dyadic religiosity and mental well-being. Third, female participants in this study may link engagement in sexual behaviors with CRR, as shared religiosity with a current or anticipated romantic partner may increase commitment (Lambert and Dollahite 2008; Ellison et al. 2010). Sharing religious views with potential or romantic partners may promote intimacy in romantic relationships, and this intimacy could encourage sexual activity. Thus, CRR may elevate relationship quality and interdependence during emerging adulthood, which could coincide with participation in sexual behaviors.
The findings of this study provide information that can be useful in understanding emerging adult development, particularly romantic development. As emerging adults begin to explore their identities through participation in romantic relationships, they simultaneously begin to explore religious and sexual behaviors with these romantic partners. The exploration of both of these behaviors reciprocally influence each other. Individuals who report lower levels of CRR may be at risk for unhealthy sexual behaviors. To promote healthy development, emerging adults may be encouraged to discuss and experience religious activities with potential and current romantic partners.
Limitations and Conclusions
Although this study advances knowledge concerning religiosity and sexual behaviors for emerging adults, it is not without its limitations. First, the demographics of this study is predominantly white women from a Midwestern area of the United States. Larger, more diverse samples would provide a better explanation for the influence of CRR for participation in sexual behaviors. Additionally, future studies should capture measures of CRR and frequency of sexual behaviors from both partners in a current or anticipated romantic relationship. Other measures of sexual behaviors, such as sexual attitudes and reasons for engaging in sexual behaviors may also provide more details about the relationship between CRR and sexual behaviors for emerging adults. Next, data was only collected at one single point in time. Future investigations should examine CRR and sexual behaviors longitudinally to elucidate the findings of the current study. Despite these limitations, this study was one of the first to examine the effects of CRR for affectionate and sexual behaviors in emerging adults. Results of the current study demonstrate that CRR contributes to the participation in affectionate and sexual behaviors. Consistent with cognitive dissonance theory, high levels of CRR was associated with less frequent sexual behaviors, and this finding was more significant for men than women in this study. This study expounds research on religious and sexual development of emerging adults.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Sage Publications.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480. https://doi.org/10.1037/0003-066X.55.5.469.
Baumeister, R. F., & Vohs, K. D. (2004). Sexual economics: Sex as female resource for social exchange in heterosexual interactions. Personality and Social Psychology Review, 8, 339–363. https://doi.org/10.1207/s15327957pspr0804_2.
Benokraitis, N. (2011). Marriages & families: Changes, choices, and constraints (8th ed.). Boston, MA: Pearson Publishing.
Collins, W. A., Welsh, D. P., & Furman, W. (2009). Adolescent romantic relationships. Annual Review of Psychology, 60, 631–652. https://doi.org/10.1146/annurev.psych.60.110707.163459.
Cotton, S., McGrady, M. E., & Rosenthal, S. L. (2010). Measurement of religiosity/spirituality in adolescent health outcomes research: Trends and recommendations. Journal of Religion and Health, 49, 414–444. https://doi.org/10.1007/s10943-010-9324-0.
Davidson, J. K., Darling, C. A., & Norton, L. (1995). Religiosity and the sexuality of women: Sexual behavior and sexual satisfaction revisited. Journal of Sex Research, 32, 235–243. https://doi.org/10.1080/00224499509551794.
Deaton, A. S. (2009). Aging, religion, and health. National Bureau of Economic Research (NBER), working paper no. 15271.
Ellison, C. G., Burdette, A. M., & Wilcox, W. B. (2010). The couple that prays together: Race and ethnicity, religion, and relationship quality among working-age adults. Journal of Marriage and Family, 72, 963–975. https://doi.org/10.1111/j.1741-3737.2010.00742.x.
Festinger, L. (1962). Cognitive dissonance. Scientific American, 207, 93–107. https://doi.org/10.1038/scientificamerican1062-93.
Fincham, F. D., Ajayi, C., & Beach, S. H. (2011). Spirituality and marital satisfaction in African American couples. Psychology of Religion and Spirituality, 3, 259–268. https://doi.org/10.1037/a0023909.
Gute, G., Eshbaugh, E. M., & Wiersma, J. (2008). Sex for you, but not for me: Discontinuity in undergraduate emerging adults’ definitions of “having sex”. Journal of Sex Research, 45, 329–337.
Hardy, S. A., & Raffaelli, M. (2003). Adolescent religiosity and sexuality: An investigation of reciprocal influences. Journal of Adolescence, 26, 731–739. https://doi.org/10.1016/j.adolescence.2003.09.003.
Huber, S., & Huber, O. W. (2012). The centrality of religiosity scale (CRS). Religions, 3, 710–724. https://doi.org/10.3390/rel3030710.
Hull, S. J., Hennessy, M., Bleakley, A., Fishbein, M., & Jordan, A. (2011). Identifying the causal pathways from religiosity to delayed adolescent sexual behavior. Journal of Sex Research, 48, 543–553. https://doi.org/10.1080/00224499.2010.521868.
Kirk, C. M., & Lewis, R. K. (2013). The impact of religious behaviors on the health and well-being of emerging adults. Mental Health, Religion & Culture, 16, 1030–1043. https://doi.org/10.1080/13674676.2012.730037.
Lambert, N. M., & Dollahite, D. C. (2008). The threefold cord: Marital commitment in religious couples. Journal of Family Issues, 29, 592–614. https://doi.org/10.1177/0192513X07308395.
Langlais, M. R., Kivisto, K. L., & Welsh, D. P. (2010). Communication and sexual behaviors within adolescent couples. Psi Chi Journal of Undergraduate Research, 15, 194–202.
Langlais, M. R., & Schwanz, S. J. (2017). Religiosity and relationship quality of dating relationships: Examining relationship religiosity as a mediator. Religions, 8, 187. https://doi.org/10.3390/rel8090187.
LeJeune, B. C., Zimet, G. D., Azzouz, F., Dennis Fortenberry, J., & Aalsma, M. C. (2013). Religiosity and sexual involvement within adolescent romantic couples. Journal of Religion and Health, 52, 804–816. https://doi.org/10.1007/s10943-011-9512-6.
McCree, D. H., Wingood, G. M., DiClemente, R., Davies, S., & Harrington, K. F. (2003). Religiosity and risky sexual behavior in African-American adolescent females. Journal of Adolescent Health, 33, 2–8. https://doi.org/10.1016/S1054-139X(02)00460-3.
Moreau, C., Trussell, J., & Bajos, N. (2013). Religiosity, religious affiliation, and patterns of sexual activity and contraceptive use in France. The European Journal of Contraception and Reproductive Health Care, 18, 168–180. https://doi.org/10.3109/13625187.2013.777829.
Petersen, J. L., & Hyde, J. S. (2011). Gender differences in sexual attitudes and behaviors: A review of meta-analytic results and large datasets. Journal of Sex Research, 48, 149–165. https://doi.org/10.1080/00224499.2011.551851.
Pew Research Center. (2017). Religious landscape study. Retrieved from http://www.pewforum.org/religious-landscape-study/.
Qualtrics. (2017). Qualtrics, Provo, UT, USA. http://www.qualtrics.com.
Rohrbaugh, J., & Jessor, R. (1975). Religiosity in youth: A personal control against deviant behavior. Journal of Personality, 43, 136–155. https://doi.org/10.1111/j.1467-6494.1975.tb00577.x.
Rostosky, S. S., Regnerus, M. D., & Wright, M. C. (2003). Coital debut: The role of religiosity and sex attitudes in the Add Health Survey. Journal of Sex Research, 40, 358–367. https://doi.org/10.1080/00224490209552202.
Steinman, K. J., & Zimmerman, M. A. (2004). Religious activity and risk behavior among African American adolescents: Concurrent and developmental effects. American Journal of Community Psychology, 33, 151–161. https://doi.org/10.1023/B:AJCP.0000027002.93526.bb.
Sternberg, R. J., & Weis, K. (2006). The new psychology of love. New Haven, CT: Yale University Press.
Stiftung, B. (2009). What the world believes: Analysis and commentary on the Religion Monitor 2008. Gutersloh: Verlag Bertelsmann-Stiftung.
Vasilenko, S. A., & Lefkowitz, E. S. (2014). Changes in religiosity after first intercourse in the transition to adulthood. Psychology of Religion and Spirituality, 6, 310–315. https://doi.org/10.1037/a0037472.
Vohs, K. D., Catanese, K. R., & Baumeister, R. F. (2004). Sex in ‘His’ versus ‘Her’ relationships. In J. H. Harvey, A. Wenzel, S. Sprecher, J. H. Harvey, A. Wenzel, & S. Sprecher (Eds.), The handbook of sexuality in close relationships (pp. 455–474). Mahwah, NJ: Lawrence Erlbaum Associates Publishers.
Young, M., Denny, G., Penhollow, T., Palacios, R., & Morris, D. (2015). Hiding the word: Examining the relationship between a new measure of religiosity and sexual behavior. Journal of Religion and Health, 54, 922–942. https://doi.org/10.1007/s10943-013-9777-z.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Langlais, M.R., Schwanz, S.J. Centrality of Religiosity of Relationships for Affectionate and Sexual Behaviors Among Emerging Adults. Sexuality & Culture 22, 405–421 (2018). https://doi.org/10.1007/s12119-017-9474-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12119-017-9474-2