
Abstract
Syphilis was the first sexually transmitted disease to be diagnosed in childhood. Most developed countries controlled syphilis effectively after the 1950s and congenital syphilis became rare. Since the late 1990s there has been a resurgence of syphilis in developed and developing countries and the WHO estimates that at least half a million infants die of congenital syphilis every year. The earliest reference to the dental manifestations of congenital syphilis was by Sir Jonathan Hutchinson, Assistant Surgeon at The London Hospital in 1861. Three main dental defects are described in congenital syphilis; Hutchinson’s incisors, Moon’s molars or bud molars, and Fournier’s molars or mulberry molars. Although many physicians, dentists, and pathologists in developed countries will be aware of the dental features of syphilis, most will never have seen a case or made the diagnosis. The purpose of this article is to review some of the history of congenital syphilis, remind healthcare professionals of the features, and bring to their attention that the changes are still prevalent and that milder cases can be mistaken for other causes of hypoplasia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Most developed countries controlled syphilis effectively after the 1950s. Cases became rare, were limited to risk populations, were identified rapidly, treated effectively and spread minimised by contact tracing. Congenital syphilis, caused by vertical transmission during pregnancy, almost disappeared. Since the late 1990s there has been a resurgence of syphilis in the UK and elsewhere and the majority of cases have been in men who have sex with men [1]. In 2012 in the UK, of the 2978 cases diagnosed, 265 were in women and that number is relatively stable and falling slowly [1, 2]. However, approximately 5 % of pregnant women miss their antenatal screening tests, usually for cultural reasons, and congenital syphilis is now found again in the UK [1]. A similar resurgence has also been noted in Switzerland and several hundred cases are detected each year in the United States [3, 4]. Elsewhere in the world, congenital syphilis remains common and the WHO estimates that at least half a million infants die of congenital syphilis every year [5].
Although many physicians, dentists and pathologists in developed countries will be aware of the dental features of congenital syphilis, most will never have seen a case or made the diagnosis. The purpose of this article is to review some of the history of congenital syphilis and illustrate in detail the dental stigmata. It is salutary to review the appearances, see how variable they can be, and how easily misdiagnosed as other forms of enamel hypoplasia.
Syphilis was the first sexually transmitted disease to be diagnosed in children. Shortly after the first recorded outbreak in Europe, in 1497 Torella described some clinical manifestations of syphilis in infants [6]. The first detailed description of congenital syphilis dates back to the sixteenth century, by which time syphilis was epidemic in Western Europe [7]. This era of extremely high incidence and virulence was key to recognizing congenital syphilis as a sequela of maternal disease. The relationship was established in the late eighteenth century, aided by the establishment in 1781 of the ‘Hospice de Vaurigard’ in Paris where pregnant syphilitic women and their offspring were treated [7]. Their detailed descriptions were also important in differentiating congenital syphilis from gonorrhoea, which was also prevalent at the time and gave rise to ophthalmic diseases [7].
Transmission
In the sixteenth century, infants were thought to contract syphilis through suckling, either from a breast lesion or from the milk [7]. Paracelsus believed that “hereditary syphilis” was transmitted from infected father to son [7]. A few decades later, the surgeon Ambroise Pare proposed the converse, that the mother’s womb was the most likely site of infection [7]. In 1749, the Parisian surgeon Antoine Louis noted in his dissertation how a woman, infected by what was then termed ‘the venereal virus’, gave birth to a child showing signs of this illness and called it an acquired illness [7]. With the discovery of Treponema pallidum in 1905, it was confirmed that the organism was too large to be carried by spermatozoa and that direct infection of the foetus by the father could not occur [6]. The risk of transmission from infected mother to child was determined in the Oslo study of untreated syphilis, which concluded that 49 % of infants born to syphilitic mothers had congenital disease, of which 25 % had latent seropositive disease and 26 % were seronegative [8].
Clinical Features
According to a systematic review and meta-analysis by Gomez, a summary estimate of 66.5 % of pregnant women infected with syphilis report adverse pregnancy outcomes such as stillbirth, fetal loss, neonatal death, clinical evidence of syphilis, prematurity, and low birth weight [9]. Those not suffering stillbirth or neonatal death usually show no visible signs of the disease at the time of birth and some weeks may elapse before clinical features become evident [7]. The majority start to show some symptoms by 2 months after birth. Treponema pallidum crosses the placenta only after the 16th week of intrauterine life and it affects the facial structures and teeth according to the time of infection [10]. Early features include a diffuse maculopapular rash, periostitis (frontal bossing of Parrot), and rhinitis. The early skin inflammation can also give rise to the permanent radial scarring around mouth known as ‘rhagades’ [10, 11]. Other orofacial manifestations include atrophic glossitis, yellow discolouration of lips, and high narrow palatal vault [10].
In 1810, Bertin was the first to give a detailed description of the clinical features of congenital syphilis and to recognise the importance of bony lesions [6]. The bone deformities, mainly the characteristic ‘saddle nose’, frontal bossing and ‘sabre shin’ all result from periostitis and are detectable very early. Late features, manifesting at least 24 months after birth, comprise the Hutchinsonian triad of interstitial keratitis of the cornea, sensorineural hearing loss, and dental anomalies [12].
Dental Defects
The earliest reference to the dental manifestations of congenital syphilis was by Sir Jonathan Hutchinson, Assistant Surgeon at The London Hospital, England, in 1861 [12]. Dental defects are the most consistent clinical manifestation of syphilis and are pronounced in teeth, which calcify in the first year of life such as permanent incisors and first molars [10]. According to Putkonen (1962) who investigated 235 syphilis patients, 45 % with permanent incisors showed features of Hutchinson’s form. And 22 % with first permanent molars had Moon’s form. However, only 12 % showed cortical thickening related to periostitis on radiographs of the limbs [13]. Dental stigmata therefore have a diagnostic advantage over osseous deformities [11].
What has never been clear is the precise nature of the disruption to tooth crown formation caused by congenital syphilis, and the reason for its very short duration. In 1944, Bauer carried out an extensive investigation of tooth buds and jaws of foetuses, babies and children who succumbed to syphilis to demonstrate that the infected tooth buds were extensively infiltrated by Treponema pallidum spirochetes. He also confirmed that the number of the microorganisms reduced with advancing age [14].
Hutchinson’s Incisors
Sir Jonathan Hutchinson also noted that the dental defects were restricted to the permanent teeth. According to Hutchinson the colour of the teeth is also abnormal, the affected teeth being semi-translucent rather than the ivory colour of normal teeth [11, 12]. In incisors affected by congenital syphilis the incisal edge has been described as either notched or ‘screw driver shaped’. The bulbous crown is described as ‘barrel shaped’. In his original article, Hutchinson states; ‘The teeth are short and narrow. Instead of becoming wider as they descend from the gum, they are narrower at their free edges than at their crowns, their angles having been, as it were, rounded off. In the centre of their free edge is a deep vertical notch, made by the breaking away or non-development of the middle lobe of the tooth-crown. This notch taken together with the narrowness and shortness of the tooth, is the main peculiarity’ [12].
In 1884, Alfred Fournier further elaborated on this feature, stating that the central notch is not apparent when the teeth first erupt and also that, at least in that era, it was soon lost through wear. He also established that this feature was more common in the upper permanent central incisor than in other incisors. When the notch is not present and the barrel shaped tooth has a flat but narrow incisal edge, the term ‘screwdriver incisor’ is often used [11].
Moon’s Molars or Bud Molars
The first description of the characteristic defect of permanent first molars was given by Henry Moon, Dental Surgeon at Guy’s Hospital (1877) [15]. He described these teeth as being small and dome shaped, with cusps set closer together than normal. The crowns are widest at the base and the narrowest at the cusps, have no grooves running around the cusps and the crown surface is smooth. These teeth were later referred to as ‘Moon’s molars’ and in some cases as ‘bud molars’, the latter term aptly describing their morphology.
Fournier’s Molars or Mulberry Molars
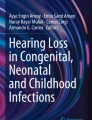
Fournier (1884) described a different form of permanent molar defect associated with congenital syphilis in which there is a deep groove around the base of each cusp caused by enamel hypoplasia. He described it as ‘a smaller tooth growing out of a larger one, a stump growing from a normal crown’ [16]. The defect is clearly very different from that described by Moon and probably results from infection at a slightly different time of development. Though the two defects are distinct, the terms have often been confused, even by the originator of the term mulberry molar, Karnosh, who proposed it to describe both types, though his illustration clearly shows Fournier molars [11, 17]. This defect can also be associated with other causes of severe enamel hypoplasia but is rarely as pronounced as is seen in congenital syphilis (Fig. 1).

Syphilitic teeth. Above a Moon’s molar and incisors with only the central incisors showing the typical notched form. Below Fournier or mulberry molars and a syphilitic canine. With kind permission from the odontological collection at the Hunterian Museum, Royal College of Surgeons of England, London
Syphilitic Canine
Several studies describe typical features of a syphilitic canine, but this defect is less frequently found than other incisor and molar defects. According to an archeological study, maxillary and mandibular canines are as distinctive in morphology as the upper central incisors and are bulbous column-like pegs with an occlusal notch and an elevated ring of enamel on the occlusal surface [18]. Jacobi further states that canines are visibly smaller and simpler than usual and exhibit no identifiable mesial canine ridge, distal accessory ridge, or dental tubercle. Canines exhibit linear enamel hypoplasia episodes on all surfaces. Fournier also described a similar groove around the tip of the upper or lower permanent canines [11].
Other Features and Significance
It is perhaps unfortunate that so much emphasis is placed on these highly characteristic dental malformations. Most published descriptions show them to the exclusion of other less specific hypoplastic defects. Typical dental features are present in at least 65 % of affected children, but others often show non-specific severe hypoplasia followed by rapid attrition and abrasion or milder pitting defects affecting the occlusal third of incisors and first permanent molars [19]. Marked linear horizontal banding of chronological hypoplasia is also sometimes present and treatment of the mother, effective or not, may modulate the appearances to a milder form, as has been seen since the introduction of antibiotic treatment. These non-specific changes are often ignored in the medical literature and are perhaps best described in the anthropological literature [18, 20] though in such cases the exact causes of all changes cannot be known. According to a study by Jacobi et al., individuals with dental signs of congenital syphilis are 2.5 times more likely to exhibit low to severe levels of linear enamel hypoplasia than those without, twice as likely to exhibit extremely severe hypoplasia, and 7.5 times more likely to exhibit pitting hypoplasia [18]. They further describe that the main dental stigmata are only the tip of the iceberg, representing perhaps one third of those with congenital syphilis and conclude that the extremely frequent and severe hypoplasia present in their series was largely attributable to congenital syphilis. There is a risk that mild changes mimic other more common causes of hypoplasia including the very variable presentation of molar-incisor hypomineralisation [21] and could easily be missed if congenital syphilis were not considered. Congenital syphilis never went away and, though uncommon, can still be relevant to diagnosis and its variability needs to be appreciated.
References
Recent epidemiology of infectious syphilis and congenital syphilis in England. In: Health protection report. 2013. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/336760/hpr4413_sphls.pdf. Accessed 5 Jan 2016.
Number and rates of selected STI diagnoses in the UK, 2009–2013. In: Public health England. 2015. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/437433/hpr2215_STI_NCSP_v6.pdf. Accessed 6 Jan 2016.
Meyer S, Trück J, Bosshard P, et al. Congenital syphilis in Switzerland: gone, forgotten, on the return. Swiss Med Wkly. 2012;. doi:10.4414/smw.2012.13325.
Syphilis, In: Sexually transmitted diseases surveillance. In: Centres for disease control and prevention. 2011. http://www.cdc.gov/std/stats11/syphilis.htm.
Eliminating congenital syphilis: A global health priority. In: Geneva World Health Organization.2005.http://www.who.int/reproductivehealth/publications/rtis/eliminating_congenital_syphilis.pdf.
Estreich S, Forster G. Sexually transmitted diseases in children: introduction. Sex Transm Infect. 1992;68(1):2–8. doi:10.1136/sti.68.1.2.
Lomax E. Infantile Syphilis as an Example of Nineteenth Century Belief in the Inheritance of Acquired Characteristics. J Hist Med Allied Sci. 1979;XXXIV(1):23–39. doi:10.1093/jhmas/xxxiv.1.23.
Gjestland T. The Oslo study of untreated syphilis: an epidemiologic investigation of the natural course of syphilitic infection based on a restudy of the Boeck-Bruusgaard material. Acta Derm Venereol (Stockh). 1955;35:1–368.
Gomez G, Kamb M, Newman L, Mark J, Broutet N, Hawkes S. Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ. 2013;91(3):217–26. doi:10.2471/blt.12.107623.
Leão J, Gueiros L, Porter S. Oral manifestations of syphilis. Clinics. 2006;61(2):161–6. doi:10.1590/s1807-59322006000200012.
Hillson S, Grigson C, Bond S. Dental defects of congenital syphilis. Am J Phys Anthropol. 1998;107(1):25–40. doi:10.1002/(sici)1096-8644(199809)107:1<25:aid-ajpa3>3.0.co;2-c.
Hutchinson J. Clinical lecture on heredito-syphilitic struma: and on the teeth as a means of diagnosis. Br Med J. 1861;1(20):515–7. doi:10.1136/bmj.1.20.515.
Putkonen T. Dental changes in congenital syphilis. Relationship to other syphilitic stigmata. Acta Derm Venerol. 1962;43:240–9.
Bauer W. Tooth buds and jaws with patients with congenital syphilis. Correlation between distribution of Treponema pallidum and tissue reaction. Am J Surg Pathol. 1944;20:297–319.
Moon H. On irregular and defective tooth development. Trans Odontol Soc GB. 1877;9:223–43.
Fournier A. Syphilitic teeth. Dent Cosmos. 1884;26:12–25.
Waldron T. Henry moon and his molars. Dent Hist. 2014;59:17–24.
Jacobi K, Cook D, Corruccini R, Handler J. Congenital syphilis in the past: slaves at Newton Plantation, Barbados, West Indies. Am J Phys Anthropol. 1992;89(2):145–58. doi:10.1002/ajpa.1330890203.
Fiumara N. Manifestations of late congenital syphilis. An analysis of 271 patients. Arch Dermatol. 1970;102(1):78–83. doi:10.1001/archderm.102.1.78.
Mayes, et al. Stigmata of congenital syphilis on a high status juvenile at Yuguë, Oaxaca, Mexico. Dent Anthropol. 2009;22:73–84.
Crombie F, Manton D, Palamara J, Zalizniak I, Cochrane N, Reynolds E. Characterisation of developmentally hypomineralised human enamel. J Dent. 2013;41(7):611–8. doi:10.1016/j.jdent.2013.05.002.
Acknowledgments
Our thanks are due to the Royal College of Surgeons of England for permission to reproduce photographs of specimens.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nissanka-Jayasuriya, E.H., Odell, E.W. & Phillips, C. Dental Stigmata of Congenital Syphilis: A Historic Review With Present Day Relevance. Head and Neck Pathol 10, 327–331 (2016). https://doi.org/10.1007/s12105-016-0703-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-016-0703-z