
Abstract
The aim of this analysis is to identify latent subgroups of women based on substance use, exposure to violence, and risky sexual behaviors and quantify discrete stages of behavior change over time. Data comes from 317 women recruited from a Municipal Drug Court System in the Midwest. All participants were interviewed regarding their substance use and sexual behaviors, as well as their exposure to violence at baseline, a 4th-month follow-up, and an 8th-month follow-up. A latent transitional analysis (LTA), a longitudinal extension of a latent class analysis (LCA), was used to quantify discrete stages of behavior change. The results of our analyses revealed 4 distinct behavioral profiles in our sample: 1) women with high probabilities of risky sexual behaviors, exposure to violence, and crack/cocaine use, 2) women with a high probability of exposure to violence, and moderate sexual risk taking, 3) women characterized solely by a high probability of crack/cocaine use, 4) women with low probabilities of all factors. The proportion of women in latent statuses characterized by a high probability of crack/cocaine use did not substantially decrease over time. Women who experienced child sexual abuse, had a greater number of lifetime arrests, were older, and believed they had risky drug using behavior that needed changing at baseline were significantly more likely to be in higher-risk latent statuses. Targeted interventions tailored to crack/cocaine users, as well as a wide-spread need for trauma-informed interventions among females involved in the criminal justice system, are needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Females in the Criminal Justice System and Syndemic Theory
Currently, females have emerged as the fastest growing prison population, yet are under-represented in research (Welty et al., 2016; Millay, Satyanarayana, O’Leary, Crecelius, & Cottler, 2009). Females in the criminal justice system, including those in drug courts, have been shown to have comorbid issues such as exposure to violence and HIV/AIDS risk behaviors including multiple sex partners and unprotected sex (Festinger, Dugosh, Kurth, & Metzger, 2016; Morse, Silverstein, Thomas, Bedel, & Cerulli, 2015; DePesa, Eldridge, Deavers, & Cassisi, 2015; Cosden, Larsen, Donahue, & Nylund-Gibson, 2015; Meyer, Cepeda, Taxman, & Altice, 2015; Messina, Calhoun, & Braithwaite, 2014; Saxena, Messina, & Grella, 2014, Torchalla, Nosen, Rostam, & Allen, 2012; Millay et al., 2009). Specifically, female offenders have been reported to have substance use related problems at a higher rate than male offenders and nearly ten times higher than non-offending women (Saxena et al., 2014). Research by Cosden et al. (2015) found that a lifetime prevalence of comorbid trauma and substance use has been reported by 80–90% among in-treatment individuals.
In a recent meta-analysis by Gilbert et al. (2015), the relationship between substance use and violence was described as intricate and bidirectional. Moreover, females involved in the criminal justice system have been shown to be up to 15 times more likely than non-incarcerated females and almost twice as likely as incarcerated males to test positive for HIV (Meyer et al., 2015; Lichtenstein & Malow, 2010). The intersectionality of substance use, violence, and HIV/AIDS risk behaviors, termed the SAVA syndemic (Substance Abuse, Violence, HIV/AIDS), are known to be synergistic and mutually re-enforcing, and the most common pathway to initial criminal justice involvement among females, with the continuation of these issues linked with increased odds of recidivism in this population (Meyer et al., 2015; Abad et al., 2015; Meyer, Springer, & Altice, 2011; Lichtenstein & Malow, 2010; Singer, 2009; Singer, 2006).
Trans-theoretical Model Stages of Changes
A theoretical framework that has been widely used in understanding behavior change and may also help understand changes in addictive and co-occurring issues such as violence and HIV/AIDS risk behaviors is the Trans-theoretical model, simply known as the Stages of Change model (Serafini, Shipley, & Stewart, 2016; Proeschold-Bell et al., 2016; Gold et al., 2016; Abad et al., 2015; Prochaska, DiClemente, & Norcross, 1992). In this model, Prochaska et al. (1992) suggest that there are 4 stages of change through which individuals move to make changes in their behaviors: 1) the pre-contemplation stage, where individuals are unaware of the necessity to change, 2) the contemplation stage, where individuals are aware of behavior that needs to change but have not made any definitive decision to change, 3) the action stage, where individuals are considerably modifying their behaviors for up to 6 months and 4) the maintenance stage, where the prime focus is relapse prevention. Theories of health behavior change suggest that change occurs in stages; thus, new analysis techniques such as the latent transitional analysis (LTA), a longitudinal extension of a latent class analysis (LCA), can serve as a means to quantify discrete stages of behavior change, through the estimation of the probability of transitions among those in observed latent statuses (Cosden et al., 2015; Lanza & Collins, 2008; Lanza, Patrick, & Maggs, 2010).
A person-centered approach for modeling behavior profiles such as LTAs, classifies multiple dimensions of behavior to aggregate individuals with common behavioral patterns in each “latent status” (Rhoades, Greenberg, Lanza, & Blair, 2011). In LTA, latent statuses are referred to as “latent statuses” rather than “latent classes” because individuals may change membership in latent statuses over time, a contrast from the stagnant class memberships in LCA.22 Simply, this analysis is appropriate for answering questions regarding the behavioral profiles of individuals who are more likely to change over time (Roberts & Ward, 2011).
Gaps in Knowledge
Though women in the criminal justice system have the highest rates of substance use related problems, this high-risk group of women is often excluded from large-scale epidemiologic studies (Welty et al., 2016). Furthermore, within the literature on substance use and criminal justice-involved individuals, studies often do not decipher differences in types of substances used though it is evident that different drugs have different etiologies, for example, marijuana and crack/cocaine (Welty et al., 2016). Prior analyses among a sample of women in the criminal justice system have reported crack/cocaine as the most common drug of choice (DuBois, O’Leary, & Cottler, 2009). While exposure to violence has been traditionally categorized as physical or sexual assault, some studies have included emotional abuse as part of a comprehensive definition of violence and victimization (Meyer et al., 2011; Gilbert et al., 2015). Most importantly, Gilbert et al. (2015) noted that the lack of studies that delineate the effects of psychological violence from physical and sexual violence “have impeded research efforts.” Thus, this study aims to address this gap in the literature by not only including emotional abuse as part of the comprehensive definition of violence, but also delineating this type of victimization from physical and sexual assault.
In addition, extant literature has shown that women with history of childhood traumas, such as child sexual abuse (CSA) are at increased odds of victimization, substance use, and risky sexual behaviors in adulthood (Morse et al., 2015; Meyer et al., 2011, Millay et al., 2009). Research by Robertson, St. Lawrence, and McCluskey (2012) found that Drug Court participants perceived their risk of HIV/AIDS as low, though substance use and risky sexual behaviors are often co-occurring and synergistic. Lastly, female substance users involved with additional interventions such as case management have been shown to significantly reduce their substance use over time (Corsi et al., 2012).
Therefore, the aims of these analyses are to: 1) identify latent statuses of women based on substance use, exposure to violence, and risky sexual behaviors at baseline, 2) examine the proportion of women in each latent status at the baseline, 4-month follow-up, and 8-month follow-up and the probability of each transitioning to a lower-risk status over time, 3) assess the effect of intervention status on latent status transitions and 4) evaluate the association between socio-demographic characteristics, child sexual abuse, drug use perceptions, and initial latent status membership. We hypothesize that 1) several latent statuses of women will be identified, particularly a latent status characterized by a high probability of substance use, exposure to violence, and risky sexual behaviors, 2) individuals in latent statuses characterized by a high probability of crack/cocaine use will be less likely to transition to lower-risk statuses over time compared to those in statuses with low probabilities of crack/cocaine use, 3) women randomized to a peer partnered case management intervention (PPCMI) group will be more likely to transition to a lower risk status than those not in a case management in group, but a standard intervention (SI) group, and 4) women who report that they have risky drug using behaviors, have experienced child sexual abuse, are older, and have more lifetime arrests will have elevated odds of being in latent statuses categorized by high probabilities of substance use, exposure to violence, and HIV/AIDS risk compared to women without these characteristics.
Methods
Sisters Teaching Options for Prevention
Participants in this analysis were from the Sisters Teaching Options for Prevention project (STOP) (R01NR09180, PI: Cottler), a randomized controlled field study which aimed to reduce high-risk drug and sexual behaviors among females in drug court by using a two-arm behavioral intervention. Specifically, each woman received the standard intervention (SI) which consisted of the National Institute on Drug Abuse (NIDA) standard pre-and post-HIV test counseling (Johnson, Cottler, Abdallah, & O’Leary, 2011). Half of the participants were randomized to the Peer Partnered Case Management Intervention (PPCMI) in which they received up to 40 h of further assistance in accessing and utilizing needed health services, and had the social support of a peer mentor (Johnson et al., 2011). For participants assigned to the Standard Intervention, the 4-month follow-up period started after the completion of their baseline assessments, while this period started after the 10-week intervention for those in the PPCMI group. This study was approved by the Washington University of St Louis Institutional Review Board.
Outreach and Recruitment
Participants in the STOP study, who were drug court enrollees at a Municipal Drug Court System in the Midwest, were recruited by STOP research staff during court between the years 2005–2008. To be eligible for STOP, participants had to be present in court, be at least 18 years of age, have no known cognitive disability, and must have provided informed consent. Women who were interested and met the eligibility criteria for STOP were then scheduled for their initial baseline assessments. All participants were interviewed regarding their substance use and sexual behaviors, as well as their exposure to violence in the past 4 months at baseline and the 4 and 8-month follow-ups.
Measures
Validated measures such as the Washington University Risk Behavior Assessment (WU-RBA) and the Violence Exposure Questionnaire (VEQ) were used to assess participants’ behaviors and exposure to violence (Shacham & Cottler, 2010). The WU-RBA, which was adapted from NIDA’s Risk Behavior Assessment, assessed risky behavior including risky sexual and drug using behaviors, perceptions of various sexual and drug using behaviors, and socio-demographic information (Shacham & Cottler, 2010; Needle et al., 1995). The VEQ, adaped from the Conflict Tactic Scale, assessed various forms of current and past exposures to violence (Straus, 1979). Participants were also interviewed using the same assessments at the 4 and 8-month follow-up sessions.
Main Exposures
In this study, we assess factors such as the effect of the randomized intervention (PPCMI vs. SI) and socio-demographic factors such as: race (black vs. non-black), age (18–29 years of age vs. 30+), child sexual abuse (yes vs. no). A prior study on this sample provides evidence that having 4 or more arrests distinguished women at greater risk for victimization and HIV risk (Cottler, O’Leary, Nickel, Reingle, & Isom, 2014), therefore, we assessed number of lifetime arrests (categorized as 4+ life-time arrests vs. less than 4 life-time arrests). Additionally, we included a covariate of a potentially high-risk group of women: those who believed they had risky drug using behaviors that needed changing (believing you have risky drug using behaviors that need changing vs. no risky drug using behaviors that need changing).
Main Outcome-Substance Use, Violence, and HIV/AIDS Risk (Indicator Items)
Violence
Exposure to violence was assessed using the following questions: 1) “During the past 4 months, has anyone attacked you with a gun?”, 2) “During the past 4 months, has anyone pressured or forced you to participate in sexual acts against your will?”, 3) “During the past 4 months, has anyone abused you emotionally, that is, did or said things to make you feel very bad about your life?”, 4) “During the past 4 months, has anyone hurt you to the point that you had bruises, cuts, broken bones, or otherwise physically abused you?”, and 5) “During the past 4 months, has anyone attacked you with a knife, stick, bottle, or other weapon?”. Women who reported at least one of these instances were categorized as having experienced violence in the past 4 months; however, exposure to violence was categorized into two variables: 1) experienced emotional abuse and 2) being attacked with a weapon or experiencing physical and sexual abuse. These variables were created to assess whether latent statuses of women differed by types of violence experienced.
HIV/AIDS Risk
The HIV/AIDS risk items were: 1) having at least one risky partner, which is a partner who is an injection drug user or a recent partner who has other sexual partners simultaneously, 2) multiple sex partners, defined as having 2+ sex partners and 3) any unprotected sex (1+ reported unprotected sex acts), which included any unprotected oral, vaginal, or anal sex in the past 4 months.
Substance Use
Recent substance use was defined as using any substance (crack/cocaine, marijuana, stimulants, and heroin) at least one time in the past 30 days. From prior analyses, we know that in this sample, virtually all participants who used any substance used either crack/cocaine or marijuana almost exclusively (Jones et al., unpublished). Because crack/cocaine users have been shown to have worse outcomes in drug court, in this analysis, substance use was represented by two variables, 1) crack/cocaine use and 2) the use of other drugs (virtually all participants who used marijuana only).
Analysis
Analytical Technique
In this analysis, our indicator items (substance use, violence, and HIV/AIDS risk variables from which latent statuses are derived) reflect an overarching latent theme of the SAVA syndemic. The LTA model estimates three sets of parameters: latent status membership probabilities, transitional probabilities, and item-response probabilities (Lanza & Collins, 2008). The latent status membership probabilities estimate the proportion of individuals that are expected to belong to each latent status at each time period. The item-response probabilities estimate the agreement of the specific indicators of the latent variable and latent status membership, while the transitional probabilities estimate the probability of changing one latent status to another latent status at the next time period. Multinomial logistic regression was used to predict latent statuses at baseline, while intervention status was used to predict latent status changes over time.
Sample Size
Of the 319 participants in the STOP study at baseline, 261 women completed the 4-month follow-up interview, while 282 women completed the 8-month follow-up interview. The Proc LTA procedure allows for missing values in indicator items and analyzes the data under the missing at random assumption. However, this procedure does not allow for missing values in covariates, therefore, two participants who refused to report whether they experienced child sexual abuse were excluded. Thus, our final sample size consisted of 317 women at baseline, 259 at the 4-month follow-up and 280 at the 8-month follow-up. All analyses were conducted using SAS v.9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Descriptive Statistics of Sample and Indicator Items
Our sample consisted of a higher number of women who were black (71%) and were 30 years of age or older (73%) (Table 1). Many of the women in our sample experienced child sexual abuse (51%), were arrested 4 or more times (70%), while 46% believed they had risky drug using behaviors that needed changing. Half of the women were randomized to receive either the SI or the SI + PPCMI intervention. Descriptive analyses of our indicator items show that all items for risky sexual behaviors, violence, and substance use were substantially prevalent at baseline. However, all behaviors decreased over time (Table 2).
Model Fit
An initial LTA analysis, void of covariates, was modeled to examine the most appropriate number of latent statuses which produced the ideal model fit and parsimony (Table 3). A model with four latent statuses produced the best model fit statistics and was also the most interpretable. To avoid small cell sizes, latent statuses greater than four were not considered.
Item-Response Probabilities
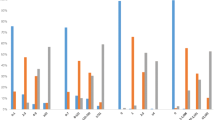
The item-response probabilities (Table 4) identified four distinct behavioral profiles (statuses) in the sample at baseline. These profiles were given labels congruent with the level of agreement with various indicators of the latent variable. Regarding the proportion of participants in the latent statuses (Fig. 1), 18% were in the High All group and the High Crack/Cocaine group at baseline, followed by 37% in the High Risky Sex and Violence group, and 27% in the Low All group. The proportion of those in the High All group reduced in size over time (16% at the 4-month follow-up, 15% at the 8-month follow-up), as well as the proportion of those in the High Risky Sex and Violence group (25% at the 4-month follow-up, 13% at the 8-month follow-up). The proportion of those in the Low All group increased in size over time (45% at the 4-month follow-up, 59% at the 8-month follow-up), however, the proportion of women in the High Crack/Cocaine group remained relatively stable over time (15% at the 4-month follow-up, 13% at the 8-month follow-up) (Fig. 1).

Prevalence of Latent Statuses Over Time (N = 317)
Latent Status Transitions
The results from the transitional probabilities, that is, the likelihood of a woman transitioning from one status to another at the next follow-up time, revealed that the many of the women were likely to remain in their prior status, particularly those in the High All and the High Crack/Cocaine groups (Table 5).
However, only 44% of the individuals in the High Risky Sex and Violence group at the 4-month follow-up were likely to remain in this status at the 8-month follow-up. The majority (54%) were likely to transition into the Low All group, while only 2% were likely to transition to the High All group (Table 5).
Correlates of Latent Statuses at Baseline
Using a multinomial logistic regression, significant differences among individuals in the latent statuses were evident (Table 6). Results revealed that those in the High All group and the High Crack/Cocaine group were significantly older than those in the Low All group (Adjusted Odds Ratio (AOR): High All group (.51), High Crack/Cocaine group (.21)), while those in the High Risky Sex and Violence group were nearly 1.92 times more likely to be younger than individuals in the Low All group. Childhood trauma also significantly differed by latent statuses, with those in the High All group and the High Risky Sex and Violence group being 2.62 and 3.07 times, respectively, more likely to experience child sexual abuse than those in the Low All group. Individuals in the High Crack/Cocaine group were as likely as those in the Low All group to experience child sexual abuse. Participants in all statuses were significantly more likely to believe they had risky drug using behaviors that needed changing compared to those in the Low All group (AOR: High All group (15.85), High Crack/Cocaine group (4.58), High Risky Sex and Violence group (2.90)). Individuals in the High Crack/Cocaine group also had significantly higher odds of being black and having 4 or more arrests (AOR 2.00, 2.49), individuals in the High All group also had increased odds of 4 or more arrests (AOR 3.34), however participants in the High All and Low All groups had decreased odds of being black compared to those in the Low All group.
Discussion
In this analysis, our first aim was to explore latent statuses of women based on substance use, victimization in adulthood (emotional, physical, or sexual abuse), and risky sexual behaviors at baseline. We hypothesized that several latent statuses of women would be identified, particularly a latent status characterized by a high probability of substance use, exposure to violence, and risky sexual behaviors. The results of this analysis supported this hypothesis as distinct behavioral profiles indicating a latent status characterized by a high probability of substance use, exposure to violence, and risky sexual behaviors (High All group), a latent status characterized by a high probability of crack/cocaine use only (High Crack/Cocaine group), a latent status characterized by a moderately high probability of emotional abuse and risky sexual behaviors (The High Risky Sex and Violence group group), and a latent status characterized by a low probability of substance use, exposure to violence, and risky sexual behaviors (Low All group) at baseline were observed.
Our second aim of this analysis was to examine the proportion of individuals in each latent status at the baseline, the 4-month follow-up, and the 8-month follow-up and the probability of transitioning to lower-risk statuses over time. We hypothesized that individuals in latent status characterized by a high probability of crack/cocaine use would be less likely to transition to lower-risk statuses over time compared to those in status with a low probability of crack/cocaine use. Our results also supported our hypothesis, though the proportion of those in the High Risky Sex and Violence group substantially decreased at every follow-up (37% at baseline to 13% at the 8-month follow-up), such substantial decreases in the High All group and the High Crack/Cocaine group were not evident. However, though a sizeable number of individuals in the High All group at baseline transitioned to a lesser-risk status, 88% of those in this latent status at the 4-month follow-up remained at the 8-month follow-up. This suggests that there may be a potential window of opportunity among those in High all group, whereas if change does not occur relatively soon, these individuals may need significantly more time to modify their behaviors. In contrast, nearly 30% of those who were in the High Crack/Cocaine group at baseline and 4-month follow-ups transitioned, and virtually all transitioned into the Low all group. The relatively stable proportion of individuals in the High Crack/Cocaine group over time presumably reflects the proportion of individuals relapsing, thus transitioning into this status at the various follow-up times. For example, nearly 10% of the women in the sizeable baseline the High Risky Sex and Violence group transitioned to the High Crack/Cocaine group by the 4-month follow-up. Moreover, the addictive nature of crack/cocaine suggests that the large reduction seen among those in the High Risky Sex and Violence group, the most transient status, may be attributed to their low probability of crack/cocaine use. These findings suggest that risky sexual behaviors may be easier modified than drug using behaviors in our sample.
We also aimed to assess the effect of intervention status on latent status transitions. However, there was no variation to be explained between the statuses, meaning that those in the standard intervention only were just as likely to transition to the low-risk status as those in the PPCMI intervention status. The lack of difference between the intervention groups may be attributed to suboptimal utilization of the case management intervention. In addition, research by DePesa et al. (2015) found that interventions to date tend to have small effects on risky sexual behaviors among female substance users.
Our last aim was to evaluate differences in the association between socio-demographic characteristics, child sexual abuse, drug use perceptions, and initial latent status membership. Our results supported our hypothesis that women who report that they have risky drug using behaviors, have experienced child sexual abuse, greater number of arrests, and older age would have elevated odds of being in statuses with higher probabilities of substance use, exposure to violence, and risky sexual behaviors compared to women who did not believe they had risky drug using behaviors that needed changing, did not experience child sexual abuse, had fewer arrests, or were younger.
Our analyses also suggest the need for trauma-informed interventions among females involved in the criminal justice system as other studies have concluded (Cosden et al., 2015; Messina et al., 2014; Saxena et al., 2014; Torchalla et al., 2012). Prior research has found that among individuals in substance use treatment, higher relapse rates were evident among women with a history of trauma due to emotional, physical, or sexual abuse compared to men who also experienced such trauma (Cosden et al., 2015). Trauma-informed interventions allow individuals to learn about how to recognize and manage the impact of trauma in their lives while in substance use treatment (Cosden et al., 2015). In our sample, child sexual abuse was a prime predictor of latent statuses characterized by risky sexual behaviors and victimization in adulthood, namely the High All and the High Risky Sex and Violence groups.
The complexity of the issues of SAVA and the hurdles such as unemployment and unstable housing that disproportionately plague the everyday of women in drug court may also play a significant role in the sub-optimal changes often seen (Morse et al., 2015). In qualitative studies of drug court enrollees, staff, community partners, as well as incarcerated females, participants consistently noted the difficulty for females to attain sobriety while facing issues related to domestic violence and the responsibilities of being the primary care-takers of children (Morse et al., 2015, Millay et al., 2009).
Limitations and Strengths
Proper interpretation of the results of this study cannot be made without addressing associated limitations. The main limitation of this study is that participants were not selected at random, thereby limiting the generalizability of our results. Also, reliance on self-report data on sensitive topics such as SAVA and child sexual abuse may lead to the underreporting of such issues. However, there are several strengths of this study including a relatively large sample size of a hard to reach and under-represented population, longitudinal data, and detailed items on SAVA. To our knowledge, this is the first study to explore and quantify sequential changes in risky sexual behavior, exposure to violence, and substance use among women involved in the criminal justice system.
Conclusion
The results of our analyses showed distinct behavioral patterns among women in drug court ranging from a high probability of substance use, exposure to violence, and risky sexual behaviors to low probabilities of these factors. Though the proportion of women in the lowest risk status (Low All group) increased substantially over time, the proportion of women in latent statuses characterized by a high probability of crack/cocaine use (High All and High Crack/Cocaine groups) did not substantially decrease over time. Our analyses suggest a wide-spread need for trauma-informed interventions among females involved in the criminal justice system, as well as targeted interventions tailored to crack/cocaine users. Our results also suggest that practical factors such as unstable housing, along with current victimization and risky sexual behaviors, should be assessed and addressed for optimal drug court outcomes among women. While few drug courts incorporate trauma-informed care, there is a dearth of studies that evaluate the results of these drug courts with the results of drug courts that do not include trauma-informed care. Future studies should assess the impact of trauma-informed care on drug court outcomes, as well as evaluate the impact of the SAVA syndemic on criminal justice outcomes.
References
Abad, N., Baack, B. N., O’Leary, A., Mizuno, Y., Herbst, J. H., & Lyles, C. M. (2015). A systematic review of HIV and STI behavior change interventions for female sex workers in the United States. AIDS and Behavior, 19(9), 1701–1719.
Cosden, M., Larsen, J. L., Donahue, M. T., & Nylund-Gibson, K. (2015). Trauma symptoms for men and women in substance abuse treatment: A latent transition analysis. Journal of Substance Abuse Treatment, 50, 18–25.
Corsi, K. F., Lehman, W. E., & Min, S. (2012). The feasibility of interventions to reduce HIV risk and drug use among heterosexual methamphetamine users. Journal of AIDS & Clinical Research, 01(S1). https://doi.org/10.4172/2155-6113.S1-010.
Cottler, L. B., O’Leary, C. C., Nickel, K. B., Reingle, J. M., & Isom, D. (2014). Breaking the blue wall of silence: Risk factors for experiencing police sexual misconduct among female offenders. American Journal of Public Health, 104(2), 338–344.
DePesa, N. S., Eldridge, G. D., Deavers, F., & Cassisi, J. E. (2015). Predictors of condom use in women receiving court-mandated drug and alcohol treatment: Implications for intervention. AIDS Care, 27(3), 392–400.
DuBois, J. M., O’Leary, C. C., & Cottler, L. B. (2009). The attitudes of females in drug court toward additional safeguards in HIV prevention research. Prevention Science, 10(4), 345–352.
Festinger, D. S., Dugosh, K. L., Kurth, A. E., & Metzger, D. S. (2016). Examining the efficacy of a computer facilitated HIV prevention tool in drug court. Drug and Alcohol Dependence, 162, 44–50.
Gilbert, L., Raj, A., Hien, D., Stockman, J., Terlikbayeva, A., & Wyatt, G. (2015). Targeting the SAVA (substance abuse, violence, and aids) syndemic among women and girls: A global review of epidemiology and integrated interventions. Journal of Acquired Immune Deficiency Syndromes, 69, S118–S127.
Gold, M. A., Tzilos, G. K., Stein, L. A. R., Anderson, B. J., Stein, M. D., Ryan, C. M., Zuckoff, A., & DiClemente, C. (2016). A randomized controlled trial to compare computer-assisted motivational intervention with didactic educational counseling to reduce unprotected sex in female adolescents. Journal of Pediatric and Adolescent Gynecology, 29(1), 26–32.
Johnson, S. D., Cottler, L. B., Abdallah, A. B., & O’Leary, C. C. (2011). History of sexual trauma and recent HIV-risk behaviors of community-recruited substance using women. AIDS and Behavior, 15(1), 172–178.
Lanza, S. T., & Collins, L. M. (2008). A new SAS procedure for latent transition analysis: Transitions in dating and sexual risk behavior. Developmental Psychology, 44(2), 446.
Lanza, S. T., Patrick, M. E., & Maggs, J. L. (2010). Latent transition analysis: Benefits of a latent variable approach to modeling transitions in substance use. Journal of Drug Issues, 40(1), 93–120.
Lichtenstein, B., & Malow, R. (2010). A critical review of HIV-related interventions for women prisoners in the United States. Journal of the Association of Nurses in AIDS Care, 21(5), 380–394.
Messina, N., Calhoun, S., & Braithwaite, J. (2014). Trauma-informed treatment decreases posttraumatic stress disorder among women offenders. Journal of Trauma & Dissociation, 15(1), 6–23.
Meyer, J. P., Cepeda, J., Taxman, F. S., & Altice, F. L. (2015). Sex-related disparities in criminal justice and HIV treatment outcomes: A retrospective cohort study of HIV-infected inmates. American Journal of Public Health, 105(9), 1901–1910.
Meyer, J. P., Springer, S. A., & Altice, F. L. (2011). Substance abuse, violence, and HIV in women: A literature review of the syndemic. Journal of Women's Health, 20(7), 991–1006.
Millay, T. A., Satyanarayana, V. A., O’Leary, C. C., Crecelius, R., & Cottler, L. B. (2009). Risky Business: Focus-status analysis of sexual behaviors, drug use and victimization among incarcerated women in St. louis. Journal of Urban Health, 86(5), 810–817.
Morse, D. S., Silverstein, J., Thomas, K., Bedel, P., & Cerulli, C. (2015). Finding the loopholes: A cross-sectional qualitative study of systemic barriers to treatment access for women drug court participants. Health & Justice, 3(1), 1–9.
Needle, R., Fisher, D. G., Weatherby, N., Chitwood, D., Brown, B., Cesari, H., Booth, R., Williams, M. L., Watters, J., Andersen, M., & Braunstein, M. (1995). Reliability of self-reported HIV risk behaviors of drug users. Psychology of Addictive Behaviors, 9(4), 242.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47(9), 1102.
Proeschold-Bell, R. J., Reif, S., Taylor, B., Patkar, A., Mannelli, P., Yao, J., & Quinlivan, E. B. (2016). Substance use outcomes of an integrated HIV–substance use treatment model implemented by social workers and HIV medical providers. Health & Social Work, 41(1), e1–e10.
Rhoades, B. L., Greenberg, M. T., Lanza, S. T., & Blair, C. (2011). Demographic and familial predictors of early executive function development: Contribution of a person-centered perspective. Journal of Experimental Child Psychology, 108(3), 638–662.
Roberts, T. J., & Ward, S. E. (2011). Using latent transition analysis in nursing research to explore change over time. Nursing Research, 60(1), 73.
Robertson, A. A., St. Lawrence, J. S., & McCluskey, D. L. (2012). HIV/STI risk behavior of drug court participants. Journal of Offender Rehabilitation, 51(7), 453–473.
Saxena, P., Messina, N. P., & Grella, C. E. (2014). Who Benefits from Gender-Responsive Treatment? Accounting for Abuse History On Longitudinal Outcomes for Women in Prison. Criminal Justice and Behavior, 41(4), 417–432.
Serafini, K., Shipley, L., & Stewart, D. G. (2016). Motivation and substance use outcomes among adolescents in a school-based intervention. Addictive Behaviors, 53, 74–79.
Shacham, E., & Cottler, L. (2010). Sexual behaviors among club drug users: Prevalence and reliability. Archives of Sexual Behavior, 39(6), 1331–1341.
Singer, M. (2006). A dose of drugs, a touch of violence, a case of AIDS, part 2: Further conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology, 34(1), 39–54.
Singer, M. (2009). Introduction to syndemics: A critical systems approach to public and community health. Hoboken: John Wiley & Sons.
Straus, M.A. (1979) Measuring Intrafamily Conflict and Violence: The Conflict Tactics (CT) Scales. Journal of Marriage and the Family, 41(1), 75
Torchalla, I., Nosen, L., Rostam, H., & Allen, P. (2012). Integrated treatment programs for individuals with concurrent substance use disorders and trauma experiences: A systematic review and meta-analysis. Journal of Substance Abuse Treatment, 42(1), 65–77.
Welty, L. J., Harrison, A. J., Abram, K. M., Olson, N. D., Aaby, D. A., McCoy, K. P., Washburn, J. J., & Teplin, L. A. (2016). Health disparities in drug-and alcohol-use disorders: A 12-year longitudinal study of youths after detention. American Journal of Public Health, 106(5), 872–880.
Acknowledgements
This study was funded by the Florida Education Fund (Jones), R01NR09180 (PI: Cottler), and partially funded by T32DA007292 (Jones AA, PI: Johnson, RM.). The authors want to acknowledge Dr. Catina O’Leary and Dr. Robert Crecilius for their essential role in the Sisters Teaching Options for Prevention (STOP) study. The authors also acknowledge all the staff and participants in STOP, the UF Department of Epidemiology, College of Medicine, College of Public Health and Health Profession.
This paper is a part of an unpublished doctoral dissertation authored by Acheampong Jones.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None to Declare.
Rights and permissions
About this article

Cite this article
Jones, A.A., Gerke, T., Striley, C.W. et al. One Step at a Time: A Latent Transitional Analysis on Changes in Substance Use, Exposure to Violence, and HIV/AIDS Risk Behaviors among Female Offenders. Am J Crim Just 43, 471–485 (2018). https://doi.org/10.1007/s12103-017-9419-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12103-017-9419-1