
Abstract
Objectives
To field test the IAP2015 (Indian Academy of Pediatrics) charts in different socioeconomic classes; to compare standard deviation scores (Z-scores) of children’s height, weight and body mass index (BMI) for age as computed based on IAP2007 or WHO charts against the IAP2015 references.
Methods
A cross-sectional observational study was conducted in the district of Pune on apparently healthy 5–18 y old children from urban affluent, urban underprivileged and rural areas. Anthropometric measurements were performed and parameters were converted into Z-scores.
Results
Urban affluent children were tallest and heaviest whereas urban underprivileged children were shortest. Z-score comparison showed that all children were shortest on WHO references and taller as per IAP2007 references. BMI Z-score was higher on IAP2007 charts and lower on WHO references. Highest number of children were within the reference range on IAP2015 charts among urban affluent. More children were classified stunted on WHO references and least on IAP2007 references. WHO references overestimated wasting and as per IAP2007 charts, less number were wasted. Less number of children were classified as being obese/overweight by WHO and IAP2007 references.
Conclusions
IAP2015 charts are better representative of healthy children of current generation and may be used to prevent inappropriate classification in present scenario.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Growth charts are a diagnostic tool used for assessment of growth of a child, and are a barometer for the evaluation of a child’s well-being. This simple diagnostic tool may help in the early detection of medical and nutritional problems and thus may facilitate early intervention. The World Health Organization (WHO) growth standards were released in 2006 and are used for children less than 5 y of age [1]. Further, growth curves that were closely aligned to the WHO Child Growth Standards were published in 2007 and as such were suggested as a suitable complementary reference for use in school-aged children and adolescents; thus, these have been used in studies for assessment of growth [2]. However, for children between 5 and 18 y, country specific growth references are recommended which are generally updated every 10 y [3].
In 2007, the Indian Academy of Pediatrics (IAP) growth monitoring committee designed growth charts for 5–18 y old Indian children [4]. The data used to construct these charts were collected between 1988 and 1991 on affluent Indian children. The IAP updated the growth charts in 2015 [5]. The charts were based on studies in 14 Indian cities collected by nine research groups over the decade before the charts were published. The new charts exhibit a secular trend i.e. boys and girls were taller at a younger age. At 18 y, average height of boys was 2.8 cm higher and the 97th percentile was 5 cm higher; for girls, these figures were 0.8 cm and 2.6 cm respectively. To define overweight and obesity in children from 5 to 18 y of age, adult equivalent of 23 and 27 kg/m2 have been suggested. The IAP growth chart committee thus recommended that the revised growth charts be used for the assessment of height, weight and body mass index (BMI) for growth of 5–18 y old Indian children to replace the previous charts.
Although the new IAP2015 charts have been constructed robustly, there is lack of field-testing of the charts. There is little data on how the recent (2015) IAP growth charts perform in comparison with previous (2007) charts and how assessments of under or overweight and stunting and wasting would change with the use of new charts. Similarly, for clinicians/researchers who have been using the WHO charts, to understand the differences in interpretations when using the IAP2015 charts vs. the WHO charts is critical. It is also important to understand and quantify the magnitude of these differences so as to adequately identify/follow children at risk of under-nutrition or over-nutrition. Further, India has a large socioeconomic divide and rural and urban underprivileged children are more likely to be stunted or wasted while the urban affluent children are likely to have a higher prevalence of children with unhealthy weights. Thus field-testing the charts in various socioeconomic settings is important [6].
Taken together, it is critical to understand how interpretations of growth parameters would change with the use of the new IAP2015 charts in different socioeconomic classes. Thus, the aim of index study was to field test the new IAP2015 charts in different socioeconomic classes. The specific objectives were 1) to compare standard deviation scores (Z-scores) of children’s height-for-age, weight-for-age and BMI for age as computed based on the previous IAP2007 or WHO charts (2007) against the recent IAP2015 references in urban affluent and underprivileged and in rural children and 2) to compare prevalence of stunting and obesity as judged by the three references.
Material and Methods
The study design was cross-sectional and assessments were performed over a period of 6 mo (June 2016- Dec 2016) in Pune district of Maharashtra (Western India). The authors studied apparently healthy children between the ages of 5 to 18 y. Those children who were syndromic (assessed by trained medical personnel) or had growth related complaints and chronic health issues, were measured but not considered in the analysis. After permission was obtained for conducting the study from school authorities, written informed consent was taken from the parents and assent from the children (>7 y) before measurements were made. An ethical approval was obtained from the institutional ethics committee.
A total of 5 English medium schools from the city of Pune (urban affluent, annual fees Rs. 28,000 to 50,000), 5 Marathi medium urban schools (urban underprivileged, free education) and 5 Marathi medium schools from rural area (rural, free education), were randomly selected from Pune district of Maharashtra and invitations were sent to them for participation in the study. Total 7 schools agreed to participate in the study (2 from urban affluent, 3 from urban underprivileged and 2 from rural). Free education was considered as proxy for lower socio-economic status. Of the schools who gave permission, one school was chosen randomly from each group (urban affluent, urban underprivileged and rural underprivileged) and all children who gave consent from the school were measured.
Anthropometric measurements were performed by two study members who were trained for anthropometric assessment. Standing height was measured by Prestige Height Meter (Range 20–210 cm) (Accuracy 0.1 cm). The children were measured without footwear and with normal school clothes. Weight was measured using portable electronic weighing scale (Salter, India) (100 g). Instruments were calibrated daily and inter- and intra- observer coefficients of variation were both <0.01(1%) and there were no significant differences between observers. Data were entered in Microsoft excel 2010 and anthropometric parameters were converted to Z-scores using the WHO Anthroplus software and data from IAP2007 and 2015 charts. Children were classified as within the reference range, stunted, severely stunted, tall, severe underweight, underweight, overweight, wasted, severe wasted, obese as per definitions laid down by respective charts [2, 4, 5].
Data were analyzed using IBM SPSS 20 version software. Data are reported as mean ± SD. Differences between groups were tested by one way ANOVA and level of significance was set at p < 0.05.
Results
Of the 2175 children who were enrolled in the study, 8 were excluded as their height and weight were either below or above 5SD score [7]. A total of 2167 (1164 boys) children were included in the study and their data were analyzed. Based on the schools, 613 children (Boys = 301) belonged to urban affluent group, 1065 (Boys = 588) were urban underprivileged and 489 (boys = 275) were rural children. Table 1 illustrates the demographic and mean anthropometric characteristics of children as per socio-economic groups. The children from all groups were comparable in age (p-value >0.05).
The mean SD scores of children from different socio-economic groups based on the old (2007) and new IAP2015 charts as well as the WHO charts are illustrated in Table 2.
Among urban affluent children (Table 3), when WHO charts were used, more children were classified as stunted in comparison with IAP2015 and IAP2007 charts. Taller children were more as per IAP2007 charts. Highest percentage of children were classified as within the reference range for height on IAP2015 charts (94.4%) as compared to WHO (93.6%) and IAP2007 charts (93.1%). As per WHO charts, (low BMI) 12.6% children were underweight, 3.6% on IAP2015 and 0.5% on IAP2007 charts. Maximum percentage of children were classified as at being risk of overweight by the IAP2015 charts (15.3%) in relation to WHO (12.%) and IAP2007 charts (10.1%). Highest prevalence of obesity among urban affluent children was noted on IAP2015 charts (9.6%) in comparison to IAP2007 (8.3%) and WHO charts (6.5%).
Children belonging to underprivileged group from urban areas (Table 3) had high prevalence of stunting i.e., 25% as per WHO charts, followed by IAP2015 (14.8%) and IAP2007 charts (11.9%). Prevalence of tall stature was the same on all charts: IAP (1%), IAP2007 charts (1.2%) and WHO (0.8%). When BMI was assessed, 26.1% children were underweight as per WHO charts compared to IAP2015 (6.7%) and IAP2007 charts (1.2%). Higher number of children were overweight as per IAP2015 charts (7.1%) compared to IAP2007 charts (4.8%) and WHO (4.5%) charts whereas obesity was noted in 2.2% children on IAP2015, 1.6% on IAP2007 charts and 1.1% on WHO charts.
Among rural group of children (Table 3), WHO charts diagnosed most stunting (20.3%) compared to IAP2015 (10.8%) and IAP2007 charts (8.4%). IAP2015, WHO and IAP2007 charts classified equal children to be tall (0.6%). For BMI, prevalence of underweight was higher on WHO (29.7%) than IAP2015 (8.2%) and IAP2007 charts (0.4%). Overweight children were more on IAP2015 charts (6.3%) than WHO references (3.9%) and IAP2007 charts (3.9%). Obesity was comparable on all charts; IAP2007 (1.4%), WHO (1.2%) and IAP2015 (1.2%).
The percentage of tall, normal height and short children based on WHO, IAP2015 and IAP2007 charts in boys and girls is shown in Figs.1 and 2.

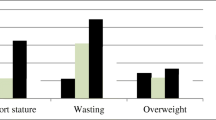
Boys anthropometric characteristics (underweight, normal weight, overweight and obese) assessed on WHO, IAP2015 and IAP2007 charts. UA Urban affluent; UU Urban underprivileged; RUR Rural

Girls anthropometric characteristics (underweight, normal weight, overweight and obese) assessed on WHO, IAP2015 and IAP2007 charts. UA Urban affluent; UU Urban underprivileged; RUR Rural
Discussion
Urban affluent children were tallest and heaviest, with the urban underprivileged group being the shortest; BMI was comparable in urban underprivileged and rural children. More number of children from all socioeconomic classes classified as short and thin as per WHO charts while the IAP2007 charts classified more children with tall stature and higher BMI.
On comparing the anthropometric Z-scores in the three socioeconomic groups using various charts (WHO, IAP2015 and IAP2007), the highest number of children from the urban affluent school were within reference range for height and highest percentage of children at risk of overweight and obesity were classified by IAP2015 charts. More number of children were classified as underweight by the IAP2015 than by the IAP2007 charts. WHO charts classified more children as short and underweight (and least overweight); IAP2007 charts showed the most number of tall children.
In the urban underprivileged and rural groups, slightly higher prevalence of stunting, underweight and overweight were noted when using the IAP2015 than the IAP2007. Maximum underweight was noted on the WHO (and minimum overweight) charts. If WHO charts were being used earlier, children from all groups would have a higher height and BMI percentile, less number would be short or underweight and a higher percentage would be found to be obese by IAP2015 charts. If the IAP2007 were being used, children would have lower height percentile (more short) and higher overweight prevalence with more short children being diagnosed.
The IAP2015 charts were made from data from 13 study groups from fourteen Indian cities. Out of 87,022 children, 33,148 children were randomly selected (including 18,170 boys and 14,978 girls). Thus, these charts have been developed from a large population of children from various parts of India, thus ensuring a good representation.
Secular trend in height, weight and BMI over a period of time is observed especially in countries in nutrition transition [8]. In developed countries (northern Europe), a secular trend in height was noted till the twentieth century and now has reached a plateau, however, the weight continues to rise, thus contributing to the epidemic of obesity [9]. Secular trend in growth is influenced by genetic potential and environmental factors such as poverty, social class, urban or rural residence, family size, education, etc. [10, 11]. Due to the nutrition transition in India, it has been necessary to update growth charts. Further, definition of obesity for Asian adults has been modified by WHO as a BMI of 23 for overweight and 27 for obesity. Adult equivalents of these values for 5–18 y old children have been implemented in IAP2015 charts.
Use of different growth references/charts results in different interpretations and prevalence of stunting, wasting etc. change as per the data used. Rosario et al. have shown that the Z-scores as per German Health Interview and Examination Survey for Children and Adolescents (KiGGS) references when compared to WHO and CDC references showed significant differences; the KiGGS references were generally higher especially at extreme percentiles [12]. Wilde et al. studied secular trends and compared WHO, references by Khadilkar et al. and Dutch references in a South Asian population residing in Netherlands and found a considerable discrepancy compared to WHO height for age references, the Khadilkar and Dutch references [13]. Orden et al. from Argentina, on comparison, have shown higher difference among WHO and national references in prepubertal period which decreased by 18 y and hence concluded that international references are of limited use as growth spurts between populations are different after the onset of puberty [14].
Studies from developing countries also go in hand with the current research. Zong et al. found a noticeable difference in height, weight and BMI SD scores among Chinese children when WHO and Chinese references were compared [15]. They attributed the difference to difference in ethnic backgrounds of the two reference populations and suggested that the references should be population specific. Mushtaq et al. from Pakistan have observed differences in Z-scores when WHO and CDC references were used and expressed the need for new references for their country based on a nationally representative sample [16].
The present study is the first of its kind where the IAP2015 charts have been field-tested. The strength of index study is that authors have studied children from three different socioeconomic classes and have made comparisons with the two commonly used references in India. However, the study has several limitations. The children studied were from one city and surrounding rural area. Also, data on puberty were not collected because of logistic reasons. Further, a study assessing children with growth disorders on various growth charts also needs to be performed.
Conclusions
The present field-testing study showed that assessment of stunting, wasting and overweight were as expected in urban affluent, urban underprivileged and rural children when using the IAP2015 references. Most children from the urban affluent school were within reference range for height; more children were classified as at risk of overweight. Higher prevalence of stunting and underweight were noted in the urban underprivileged and rural groups. Larger studies are required to confirm these observations.
References
WHO. Child growth standards. Acta Pediatr Suppl. 2006;450:5–101.
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660–7.
Buckler JM. Growth disorders in children, 1st ed. London: BMJ Publishing Group; 1994.
Agarwal DK, Agarwal KN, Upadhyay SK, Mittal R, Prakash R, Rai S. Physical and sexual growth pattern of affluent Indian children from 5-18 years of age. Indian Pediatr. 1992;29:1203–82.
Khadilkar V, Yadav S, Agrawal KK, et al. Revised IAP growth charts for height, weight and body mass index for 5- to 18-year-old Indian children. Indian Pediatr. 2015;52:47–55.
Rao S. Nutritional status of the Indian population. J Biosci. 2001;26:481–9.
Mansourian M, Marateb HR, Kelishadi R, et al. First growth curves based on the World Health Organization reference in a nationally representative sample of pediatric population in the Middle East and North Africa (MENA): the CASPIAN-III study. BMC Pediatr. 2012;12:149.
Cole TJ. The secular trend in human physical growth: a biological view. Econ Hum Biol. 2003;1:161–8.
Schmidt IM, Jørgensen MH, Michaelsen KF. Height of conscripts in Europe: is post-neonatal mortality a predictor? Ann Hum Biol. 1995;22:57–67.
Tanner JM. Growth as a measure of the nutritional and hygienic status of a population. Horm Res. 1992;38:106–15.
Cole TJ. Secular trends in growth. Proc Nutr Soc. 2000;59:317–24.
Rosario AS, Schienkiewitz A, Neuhauser H. German height references for children aged 0 to under 18 years compared to WHO and CDC growth charts. Ann Hum Biol. 2011;38:121–30.
de Wilde JA, van Dommelen P, van Buuren S, Middelkoop BJC. Height of south Asian children in the Netherlands aged 0–20 years: secular trends and comparisons with current Asian Indian, Dutch and WHO references. Ann Hum Biol. 2015;42:38–44.
Orden AB, Apezteguía MC. Weight and height centiles of Argentinian children and adolescents: a comparison with WHO and national growth references. Ann Hum Biol. 2016;43:9–17.
Zong XN, Li H. Construction of a new growth references for China based on urban Chinese children: comparison with the WHO growth standards. PLoS One. 2013;8:e59569.
Mushtaq MU, Gull S, Mushtaq K, et al. Height, weight and BMI percentiles and nutritional status relative to the international growth references among Pakistani school-aged children. BMC Pediatr. 2012;12:31.
Author information
Authors and Affiliations
Contributions
VK: Concept, design of the study, data analysis and manuscript draft; NL and AK: Data analysis and manuscript draft; SP: Data collection and analysis; SC: Data analysis and design of the study; RJ: Manuscript draft. AK and VK will act as guarantor for this paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Rights and permissions
About this article

Cite this article
Lohiya, N., Khadilkar, V., Pawar, S. et al. Field Testing of IAP2015 Charts. Indian J Pediatr 85, 723–728 (2018). https://doi.org/10.1007/s12098-018-2621-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-018-2621-4