
Abstract
Objective
To determine the weighted incidence of hearing impairment in a standardized population of at risk and not at risk neonates seeking care at a tertiary level hospital in India.
Methods
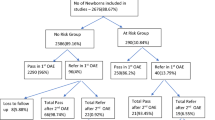
A prospective study of a nonrandomized cohort of 1769 neonates (1490: Not at risk; 279: At risk) from a total of 8192 neonates (6509: Not at risk; 1683: At risk) who sought care at St John’s medical College hospital from 1st September 2002 to 31st March 2006 were screened for hearing impairment using transient evoked otoacoustic emissions. Weighting was performed using the expected value of 10 % at risk and 90 % not at risk infants in a typical tertiary care level center in India derived from the National Neonatology and Perinatology database 2002–2003. Z test and 95 % confidence interval was used to determine the external validity of the results. P less than 0.05 was considered as statistically significant. The power of the study is 90 %.
Results
The incidence of hearing impairment in infants screened was 10 per 1769 infants screened (1490: Not at risk; 279: At risk) which is 5.65 per 1000 screened. 279 at risk infants were screened and 3 were detected to have hearing impairment which is an incidence of approximately 10.75 per 1000 screened. Of the 1490 not at risk infants screened 7 had hearing impairment that is 4.70 per 1000 screened. If this was extrapolated to a standardized population consisting of 10 % at risk and 90 % not at risk then the incidence would be 5.60 per 1000 screened with a 95 % confidence interval of 4.13–7.06. This narrow 95 % confidence interval with a p equal to 0.001 indicates that this value may be close to the caseload in a typical tertiary care center.
Conclusion
In this study the incidence of hearing impairment is 3 per 279 in at risk infants screened and 7 per 1490 in not at risk infants screened. The weighted incidence in a standardized population of neonates seeking care at tertiary level center in India is 5.60 per 1000 as per this study. This high incidence calls for all pediatricians to consider incorporating a basic hearing screen for all the neonates using cost effective and appropriate technology. Initial screening may be performed using behavioral observation techniques and confirmation by otoacoustic emissions.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Northern JL, Hayes D. Universal screening for infant hearing impairment: Necessary, beneficial and justifiable. Audiology Today, 1994; 6(3): 10–13.
Beatriz CWR. Parents of deaf children. In Prabhakar E, Claudia K, Sian T, (eds.). Listening to sounds and signs; Trends in deaf education and communication. 1st ed. Bangalore, Christoffel Blinden mission and Books for change, 1988; 14
Downs MA, Yoshinaga-Itano C. The efficacy of early identification and intervention for children with hearing impairment. Pediatr Clin North Am 1999; 46: 79–87.
Harrison M, Roush J, Wallace J. Trends in age of identification and intervention in infants with hearing loss. Ear Hear 2003; 24(1): 89–95.
Year 2000 position statement: Principles and Guidelines for Early hearing detection and intervention program. Jt Committ Infant Hearing Pediatr 2000; 106(4): 798–817.
National neonatal-perinatal database report 2002–2003, ICMR, New Delhi, NNPD nodal center at department of Pediatrics. All India Institute of Medical Sciences, 2005.
Report of the collaborative study on prevalence and etiology of hearing impairment. New Delhi, ICMR and department of Science, 1983, p. 16
Kacker SK. The scope of pediatric audiology in India. In Deka RC, Kacker SK, Vijayalakshmi B, eds. Pediatric audiology in India, 1st ed. New Delhi; Otorhinolaryngological Research Society of AIIMS, 1997; 20.
Geethachary. Analysis and final report of project on prevalence, causes and prevention of hearing impairment in rural Karnatak, Bangalore, 2002; 13. (Personal communication)
Mehl A, Thomson V. Newborn hearing screening: The Great Omission. Pediatrics 1998; 101: 34.
Cone-Wesson B, Vohr BR, Gorga MP, Norton SJ. Identification of neonatal hearing impairment: Infants with hearing loss. Ear Hear 2000; 21(5): 488–507
Hayes D, Hearing loss in infants with craniofacial anomalies, Otolaryngology. Head and Neck Surgery 1994; 110(1): 39–46.
Naulty CM, Weiss IP and Herer GR. Progressive sensorineural loss in survivors of persistent fetal circulation. Ear and Hearing 1986; 7: 74–77.
Hicks T, Fowler K, Richardson M, Dahle A, Adams L and Pass R. Congenital cytomegalovirus infection and neonatal auditory screening. Journal of Pediatrics 1993; 123: 779–782.
Arditi M, Mason E, Bradley J, Tan T, Barson W, Schultze G, Wald E et al. Three year multicenter surveillance of pneumococcal meningitis in children: Clinical characteristics and outcome related to penicillin susceptibility and dexamethasone use. Pediatrics 1998; 102: 1087–1097.
Vienny H, Despland PA, Lutschg J, Deonna T, Dutoit-Marco ML and Gander C. Early diagnosis and evolution of deafness in childhood bacterial meningitis: A study using brainstem auditory evoked potentials. Pediatrics 1984; 73: 579–586.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nagapoornima, P., Ramesh, A., Srilakshmi et al. Universal hearing screening. Indian J Pediatr 74, 545–549 (2007). https://doi.org/10.1007/s12098-007-0105-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-007-0105-z