
Abstract
Objective
The aim of this study was to investigate whether miR-15a has prognostic relevance in human gliomas.
Methods
The expression levels of miR-15a were analyzed in glioma surgical resection tissues by microarray and quantitative real-time PCR. Survival analysis by the Kaplan–Meier method was performed to assess prognostic significance.
Results
Downregulation of miR-15a was detected in most primary gliomas, which was confirmed by qRT-PCR analysis. Additionally, the down-regulation of miR-15a was significantly associated with the WHO grade (P = 0.003), the low KPS (P = 0.027), time to recurrence (P = 0.044) and the poor OS (P = 0.046). Using Kaplan–Meier analysis, a comparison of survival curves of low versus high expresser of miR-15a revealed a highly significant difference in OS (P = 0.001) and DFS (P = 0.006), which suggested that low expression of miR-15a is associated with a worse prognosis. Multivariate analyses showed that miR-15a expression was independent risk factors predicting OS [Hazard ratio (HR), 7.52; 95 % confidence interval (CI), 2.63–21.47; P = 0.002] and DFS [HR, 11.56; 95 % CI, 5.17–25.96; P < 0.001] in glioma.
Conclusions
These findings indicated for the first time that the expression of miR-15a is significantly correlated with prognosis in glioma patients, suggesting that the miR-15a may serve as independent prognostic marker.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glioma is the most common primary malignant brain tumor [1]. Gliomas account for approximately 80 % of primary malignancies of the brain, and result in more years of life lost than any other tumor [2]. Despite multimodal therapy, the disease remains one of the most lethal malignancies in humans, and the overall survival (OS) rate of high-grade gliomas is 40 % at 1 year, and the 5-year survival rate is less than 10 % [3], so, new approaches to improve the efficacy of anti-glioma treatments are urgently needed. Thus, new precise prognostic predictors and more effective therapies for glioma should be developed based on a better understanding of the molecular pathogenesis of glioma.
Previous reports have shown that expression of miRNAs is deregulated in various types of human cancers including breast cancer, colon cancer, lung cancer, pancreas cancer, and chronic lymphocytic leukemia [4–8]. Recently, a number of studies indicated that miRNAs are associated with the clinical features and outcomes of human glioma. For instance, miR-26a, miR-21, and miR-486 levels in glioma tissues correlate closely with clinical staging and inversely with disease prognosis and patient survival, respectively [9–12]. miR-15a, a recently described microRNA, has been proved to be associated with carcinogenesis and progression in various human malignancies such as multiple myeloma and renal tumor [13, 14]. However, the expression of miR-15a in glioma and its association with clinicopathologic characteristics and prognosis have not been reported yet.
In the present study, based on these various aspects of the miR-15a function, we evaluated the expression pattern of miR-15a in glioma specimens and paratumor tissues, and analyzed the relationship of miR-15a expression with glioma clinicopathologic characteristics and prognosis of patients.
Materials and methods
Patients and tissue samples
The study was approved by the ethics committee of The First People’s Hospital of Jingmen. Briefly, fresh clinical glioma specimens were obtained from 128 patients who underwent surgery between October 2000 and September 2003. None of the patients has received radiotherapy or chemotherapy prior to surgery. Twenty-one normal brain tissue samples were taken from patients who underwent surgery for reasons other than malignancy such as cerebral trauma which served as the control. Histomorphology of all the specimens was confirmed by the Department of Pathology, The First People’s Hospital of Jingmen. Grading of the specimen was done based on WHO classification (Grade I–IV). Specimens were put immediately into liquid N2 after surgical resection for 10 min, then into a −70 °C ultra-freezer for mRNA isolation. In the follow-up period, OS was measured from diagnosis to death or last follow-up. Patients’ clinical information, such as age, sex, Karnofsky performance score (KPS) and WHO grade, was collected and stored in a database. There were 66 cases, 11 cases, and 55 cases who received radiotherapy, chemotherapy, and radiotherapy and chemotherapy, respectively. Follow-up information of all eligible patients was updated every 3 months by telephone visit and questionnaire letters. OS was calculated from the date of initial surgical operation to death. Patients who died of diseases not directly related to glioma had been excluded from this study. Death of participants was ascertained by reporting from the family and verified by review of public records.
RNA extraction from surgical resection tissue and quantitative real-time PCR (qRT-PCR)
Total RNA was purified from all the 128 glioma tissues and 21 control brain tissues as recommended by the manufacturer using Trizol reagent (Invitrogen, Carlsbad,CA, USA). Only those total RNA samples with OD A260/A280 ratio close to value of 2.0, which indicates that the RNA is pure, were subsequently analyzed. Real-time absolute quantification was utilized to insure the quality of samples. The miR-15a-specific cDNA were synthesized from total RNA using gene-specific primers according to the TaqMan MicroRNA assay protocol (Applied Biosystems, Foster City, CA, USA). The reverse transcription products were then amplified and detected by real-time PCR using Taqman MicroRNA Assay (Applied Biosystems) specific for hsa-miR-15a. RNU6B was used as an internal control. The following primers were used: miR-15a 5′-GCTAGCAGCACATAATGGTTTGTG-3′ (forward); 5′-GTGCAGGGTCCGAGGTATTC-3′ (reverse); and RNU6B 5′-CTCGCTTCGGCAGCACA-3′ (forward); 5′-AACGCTTCACGAAT TTGCGT-3′ (reverse). The internal control 18 s rRNA primers were 5′-CGCCGCTAGAGGTGAAATTC-3′ and 5′-TTGGCAAATGCTTTCGCTC-3′. Each sample was examined in triplicate and the raw data were presented as the relative quantification of miR-15a expression evaluated by the comparative cycle threshold (CT) method, normalized with respect to RNU6B. Relative expression of miR-15a was calculated by 2−ΔΔCT method. Mean normalized miR-15a expression ± standard deviation (SD) was calculated from triplicate analysis. Real-time PCR was performed using an ABI 7500 system (Applied Biosystems) and comparative 2−ΔΔCT analysis was performed using SDS 2.2.2 software (Applied Biosystems).
miRNA microarray assay and data analysis
Microarray was executed in six glioma surgical resection tissues and six non-neoplastic tissues paired with glioma. The Affymetrix miRNA 3.0 Technology platform was used, which contains 1,733 mature human miRNAs. Total RNA was exerted gradually by poly(A) tailing, biotin labeling, hybridization, washing, staining, and scanning with Affymetrix Scanner 3000 (Affymetrix) according to the manufacturer’s guidelines.
Expression Console software (version 1.3.1, Affymetrix) was used to analyze array images to get raw data and then offered RMA normalization. Next, Genespring software (version 12.5, Agilent Technologies) was used in the following data analysis. Probes that, at least one group out of all samples, have flags in “P” were chosen for further data analysis. Differentially expressed miRNAs were then identified through fold change and P value comparison. The stringent threshold set for up and down-regulated genes was a fold change ≥2.0 and p value ≤0.05. Unsupervised hierarchical clustering was performed to show the distinguishable miRNA expression pattern among samples.
Follow-up
None of the patients suffered major perioperative complications, and all were discharged from the hospital. Survival time is defined as the date of last follow-up since surgery or the date of death. All patients were followed up for 5 years. The closing date for follow-up was August 31st, 2013, and if the follow-up was incomplete, patients or their families were contacted by telephone thereafter. The median follow-up time was 42.8 months (range 5.6–62.3 months).
Statistical analysis
All statistic analyses were performed using SPSS version13.0 software (SPSS Inc., Chicago, USA). The measurement data were analyzed by one-way ANOVA. Randomized block design ANOVA was used to analyze the statistical difference among different tissue types. Associations between miR-15a expression and clinicopathological characteristics were analyzed by Mann–Whitney test or Kruskal–Wallis test. Survival curves were plotted using the Kaplan–Meier product-limit method, and differences between survival curves were tested using the log-rank test. Cox’s proportional hazards model was used to identify the factors that have significantly independent influence on survival. Statistical significance was set at P < 0.05.
Results
MiRNAs profiling in glioma surgical resection tissues and qRT-PCR
To identify miR-15a expression alterations in glioma tissues and non-neoplastic tissues, we performed miRNA microarray analysis in six glioma surgical resection tissues and six non-neoplastic tissues. Among the 26 differentially expressed miRNAs, miR-15a, was down-regulated (Fig. 1).

Differentially expressed miRNAs in glioma tissues. Color gradation indicates the relative expression level of miRNAs from low expression (green) to high expression (red). NT, paratumor; T, tumor
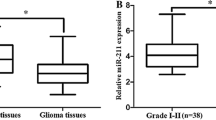
To validate the miRNA expression changes on the miRNA microarray, we employed qRT-PCR to measure the levels of miR-15a in 128 glioma surgical resection and 21 non-neoplastic tissues. We first determined the mRNA expression of miR-15a normalized to RNU6B by quantitative real-time PCR. Results showed that the relative expression of miR-15a in glioma was 2.73 ± 0.96 (mean ± SD), which was significantly lower compared with 7.42 ± 1.68 in normal brain tissues (P < 0.001). To facilitate further analysis, we defined glioma specimens with miR-15a levels less than mean expression level (2.73) as low miR-15a expression group, while specimens with miR-15a levels no less than mean level were defined as high miR-15a expression group. Consistent with the results by miRNA microarray, qRT-PCR confirmed the down-regulation of the miR-15a in glioma surgical resection (p < 0.05) (Fig. 2).

a miR-15a relative expression in glioma and paratumor was analyzed by qRT-PCR. The relative amount of miR-15a mRNA in glioma was lower than in the corresponding paratumor tissue, the difference were statistically significant (**P < 0.001). b The electrophoretogram of qRT-PCR of miR-15a from paired glioma tissues and paratumor tissues, RNU6B was used as an internal control. NT paratumor, T tumor
Correlation of miR-15a expression and clinicopathological features in glioma
When comparing the miR-15a status with clinicopathological variables, we found significant positive correlations between miR-15a expression and WHO grade (P = 0.003), KPS (P = 0.027), time to recurrence (P = 0.044), and survival (P = 0.046) (Table 1).
Relationship between miR-15a and OS and DFS of glioma patients
To investigate the prognostic value of miR-15a for glioma, we performed univariate survival analysis of miR-15a expression and factors including age, gender, location, tumor size, WHO grade, KPS, surgery, adjuvant treatment, time to recurrence, and survival in patients with glioma. In the univariate Cox proportional hazard regression model analysis shown in Table 2, WHO grade (P = 0.007), KPS (P = 0.025), time to recurrence (P = 0.031), survival (P = 0.004), and expression of miR-15a (P = 0.001) were significantly associated with OS. The WHO grade (P = 0.009), time to recurrence (P = 0.017), survival (P = 0.028), and expression of miR-15a (P = 0.006) were significantly associated with disease-free survival (DFS). Consequently, patients with tumors with high expression of miR-15a had a better prognosis than those with tumors having low miR-15a expression. The log-rank test showed that the OS time of patients with glioma was significantly different between the group with high miR-15a expression and the low miR-15a group (P = 0.007) (Fig. 3a). In patients with glioma, the low miR-15a expression group had shorter DFS time, whereas, the high miR-15a expression group had better survival (Fig. 3b).

Survival curves of 128 patients with glioma. a overall survival; b disease-free survival of patients with tumors with low or high expression levels of miR-15a
To further investigate whether the expression of miR-15a is an independent prognostic factor for glioma, we performed a multivariate Cox regression analysis of OS and DFS (Table 3). The expression of miR-15a (P = 0.002), WHO grade (P = 0.016), KPS (P = 0.001), time to recurrence (P = 0.003), and survival (P = 0.046) showed a significant association with OS. The expression of miR-15a (P < 0.001), WHO grade (P = 0.011), KPS (P = 0.002), time to recurrence (P = 0.040), and survival (P = 0.003) showed a significant association with DFS. These results showed that the expression of miR-15a was an independent prognostic factor for glioma.
Discussion
MiRNAs (known as a class of small, non-coding RNAs) play a pivotal role in the development of the malignant phenotype of glioma cells, including cell survival, proliferation, differentiation, tumor angiogenesis, and stem cell generation. Discoveries of the biological significance of miRNAs dysregulation in glioma cells not only fill some disconnected gaps between previously identified, but disconnected, mechanistic components underlying the pathogenesis of the disease, but also provide a model system through which the role of miRNA in tumorigenesis and cancer progression can be better understood.
In the present study we focus on investigating the correlation between the expression of low level of miR-15a and prognosis. The main findings of our study are as follows. First, there was high expression of miR-15a in non-neoplastic brain tissues, but decreased expression of miR-15a was observed in the glioma tissues; second, the decreased expression level of miR-15a was both associated with WHO grade, KPS, time to recurrence, and survival of glioma patients. These results imply that miR-15a may function as a tumor suppressor in glioma though the underlying mechanism of this relationship has not been well characterized.
Moreover, it has been increasingly revealed that abnormalities in the expression level of particular miRNAs might represent a new class of benchmarks indicative of the presence and progression of glioma tumors, and therefore might be of prognostic value. In this study, the prognosis of glioma patients with low expression level of miR-15a was poor, and univariate and multivariate Cox regression analysis indicated that low expression level of miR-15a was significant prognostic factors for a poor OS and DFS of glioma patients. Our data suggest that miR-15a may serve as markers for poor prognoses. Why does the miR-15a has such a strong effect on prognosis? The possible mechanisms responsible for this association are as follows. First, miR-15a inhibits NF-κB pathway, because block aberrant NF-κB activity plays a pivotal role in promoting glioma cell invasion and migration [13, 15–17]; second, miR-15a exerts antiangiogenic activity during tumor progression [13]. Accumulated evidence has shown that high vascular density, glomeruloid vessels in particular, and pro-angiogenic factor upregulation are indicative of poor prognosis for patients with gliomas [18]; Third, miR-15a may implicate in inducing tumor apoptosis [19, 20]. Most importantly, the underlying molecular mechanism may ultimately help in the development of innovative therapeutic strategies against glioma.
In conclusion, our data reveal that it might be an intrinsic regulator of tumor progression and a potential prognostic factor for this dismal disease. miR-15a can also be used in the adjuvant treatment decision and this could have great clinical value.However, the biological functions of miR-15a and its role as a tumor suppressor are worth to be further investigated.
References
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007;114:97–109.
Schwartzbaum JA, Fisher JL, Aldape KD, Wrensch M. Epidemiology and molecular pathology of glioma. Nat Clin Pract Neurol. 2006;2:494–503.
Ohgaki H, Dessen P, Jourde B, Horstmann S, Nishikawa T, Di Patre PL, et al. Genetic pathways to glioblastoma: a population-based study. Cancer Res. 2004;64:6892–9.
Harquail J, Benzina S, Robichaud GA. MicroRNAs and breast cancer malignancy: an overview of miRNA-regulated cancer processes leading to metastasis. Cancer Biomark. 2012;11(6):269–80.
Rossi S, Di Narzo AF, Mestdagh P, Jacobs B, Bosman FT, Gu-stavsson B, et al. microRNAs in colon cancer: a roadmap for discovery. FEBS Lett. 2012;586(19):3000–7.
Solomides CC, Evans BJ, Navenot JM, Vadigepalli R, Peiper SC, Wang ZX. MicroRNA profiling in lung cancer reveals new molecular markers for diagnosis. Acta Cytol. 2012;56(6):645–54.
Ali S, Saleh H, Sethi S, Sarkar FH, Philip PA. MicroRNA profiling of diagnostic needle aspirates from patients with pan-creatic cancer. Br J Cancer. 2012;107(8):1354–60.
Moussay E, Wang K, Cho JH, van Moer K, Pierson S, Paggetti J, et al. MicroRNA as biomarkers and regulators in B-cell chronic lymphocytic leukemia. Proc Natl Acad Sci USA. 2011;108(16):6573–8.
Han L, Yue X, Zhou X, Lan FM, You G, Zhang W, et al. MicroRNA-21 expression is regulated by beta-catenin/STAT3 pathway and promotes glioma cell invasion by direct targeting RECK. CNS Neurosci Ther. 2012;18:573–83.
Wang YY, Sun G, Luo H, Wang XF, Lan FM, Yue X, et al. MiR-21 modulates hTERT through a STAT3-dependent manner on glioblastoma cell growth. CNS Neurosci Ther. 2012;18:722–8.
Huse JT, Brennan C, Hambardzumyan D, Wee B, Pena J, Rouhanifard SH, et al. The PTEN-regulating microRNA miR-26a is amplified in high-grade glioma and facilitates gliomagenesis in vivo. Genes Dev. 2009;23:1327–37.
Zhang J, Han L, Ge Y, Zhou X, Zhang A, Zhang C, et al. miR-221/222 promote malignant progression of glioma through activation of the Akt pathway. Int J Oncol. 2010;36:913–20.
Roccaro AM, Sacco A, Thompson B, Leleu X, Azab AK, Azab F, et al. MicroRNAs 15a and 16 regulate tumor proliferation in multiple myeloma. Blood. 2009;113(26):6669–80.
von Brandenstein M, Pandarakalam JJ, Kroon L, Loeser H, Herden J, Braun G, et al. MicroRNA 15a, inversely correlated to PKCα, is a potential marker to differentiate between benign and malignant renal tumors in biopsy and urine samples. Am J Pathol. 2012;180(5):1787–97.
Liang F, Zhang S, Wang B, Qiu J, Wang Y. Overexpression of integrin-linked kinase (ILK) promotes glioma cell invasion and migration and down-regulates E-cadherin via the NF-κB pathway. J Mol Histol. 2014;45(2):141–51.
Parmaksız G, Czabanka M, Vinci M, Vajkoczy P. Antiangiogenic therapy inhibits the recruitment of vascular accessory cells to the perivascular niche in glioma angiogenesis. J Vasc Res. 2014;51(2):102–9.
Bow H, Hwang LS, Schildhaus N, Xing J, Murray L, Salditch Q, et al. Local delivery of angiogenesis-inhibitor minocycline combined with radiotherapy and oral temozolomide chemotherapy in 9L glioma. J Neurosurg. 2014;120(3):662–9.
Louis DN. Molecular pathology of malignant gliomas. Annu Rev Pathol. 2006;1:97–117.
Hao M, Zhang L, An G, Meng H, Han Y, Xie Z, et al. Bone marrow stromal cells protect myeloma cells from bortezomib induced apoptosis by suppressing microRNA-15a expression. Leuk Lymphoma. 2011;52(9):1787–94.
Tang R, Li L, Zhu D, Hou D, Cao T, Gu H, et al. Mouse miRNA-709 directly regulates miRNA-15a/16-1 biogenesis at the posttranscriptional level in the nucleus: evidence for a microRNA hierarchy system. Cell Res. 2012;22(3):504–15.
Acknowledgments
We are very grateful to Dr. Dong Liu and Dr. Jie Zhang for their excellent technical support.
Conflict of interest
The authors declare that they have no conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
T. Xie and P. Liu contributed equally to this study.
Rights and permissions
About this article

Cite this article
Xie, T., Liu, P., Chen, L. et al. MicroRNA-15a down-regulation is associated with adverse prognosis in human glioma. Clin Transl Oncol 17, 504–510 (2015). https://doi.org/10.1007/s12094-014-1265-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-014-1265-8