
Abstract
Lung cancer remains the most commonly diagnosed cancer worldwide and the leading cause of cancer-related mortality. More than 80 % of all newly diagnosed cases of lung cancer are non-small cell lung cancer (NSCLC). Despite recent advances, 40 % of patients still have advanced disease at the moment of diagnosis. Clinical information, pathological diagnosis and molecular assessment are needed to guide the systemic therapy, whereas discussion within an experienced team is key to adequately select the most appropriate multidisciplinary strategies. The purpose of this article is to provide updated recommendations for the management of these patients.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, responsible for approximately 1.3 million deaths every year [1]. In females, incidence rates are generally lower than men but, worldwide, lung cancer is now the four most frequent cancer of women and the second most common cause of death from cancer. According to recent data, the estimated incidence in Spain is 23,211 cases (11.8 % of all cancers), the estimated mortality is 20,327 cases (19.5 % of all cancers) and the 5-year prevalence is 24,404 cases (4.6 %). Although tobacco use is the most well-established risk factor and responsible for 85 % of cases in Western countries, an estimated 10–35 % of lung cancers worldwide occur in never-smoker patients.
Diagnosis
Pathologic diagnosis is generally made according to the World Health Organization (WHO) classification. The new International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society/European Respiratory Society lung adenocarcinoma classification provides, for the first time, standardized terminology for lung cancer diagnosis in small biopsies and cytology and use of this classification is strongly advised [2].
A limited diagnostic workup is also recommended to preserve as much tissue as possible for further molecular assessments. Evidence-based recommendations for molecular testing in lung cancer have been reviewed by SEOM-SEAP [3] (Spanish Society of Medical Oncology–Spanish Society of Pathology) and the IASLC (Table 1) [4].
Staging
After the initial diagnosis, accurate staging is crucial for determining the appropriate approach and for tailoring therapy to each individual patient. In NSCLC patients the following staging workup is strongly recommended [5].
-
Complete history, including smoking history, comorbidities, family history, and physical examination.
-
Standard laboratory tests, including hematology, renal and hepatic function.
-
Computerized tomography (CT) scan of the chest and upper abdomen.
-
Magnetic resonance imaging (MRI) or CT-scan of the brain if there are neurologic symptoms
-
Bone scan in the presence of bone pain, elevated serum calcium, or elevated alkaline phosphatase levels.
-
In the presence of pleural or pericardial effusions, or a single metastatic lesion, cytological or histological confirmation should be recommended to confirm stage IV disease.
For patients with potentially radical treatment, the following recommendations should be considered:
-
Whole-body FDG-positron emission tomography (PET) CT-scan shows high accuracy to detect mediastinal involvement and distant metastasis, and can avoid unnecessary thoracotomies.
-
Invasive mediastinal staging [endobronchial ultrasound-guided fine-needle aspiration (EBUS-FNA), endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA)] or mediastinoscopy, is recommended in patients with PET-positive mediastinal or hilar LNs. In patients with PET-negative LNs, invasive staging is recommended in CT enlarged mediastinal LNs (>1.5 cm) and in patients with central tumors.
-
MRI or CT-scan of the brain may be considered.
Staging system
Non-small cell lung cancer is staged according to the UICC system (7th edition), grouped into stage categories (Tables 2, 3) [6].
Treatment
Stage I–II
In patients with stage I–II NSCLC a multidisciplinary evaluation by a tumor committee board is recommended to establish the best strategy for patient management.
Surgery remains the cornerstone treatment for stage I–II NSCLC for patients willing to accept the risks of this procedure.
-
A careful preoperative physiologic assessment will be useful to identify those patients who are at increased risk of post-operative complications following standard lung cancer resection.
-
In functionally fit patients with stage I–II disease, anatomical surgical resection is recommended (lobectomy with lymphadenectomy). More limited resections (segmentectomy and wedge resection) tend to be associated with an increased risk of local recurrence [7]. The optimum extent of resections for small lesions (<2 cm), adenocarcinoma in situ and minimally invasive adenocarcinoma, are the subject of ongoing investigation. Randomized trials are yet to solve the controversial issue of node sampling versus systematic nodal dissection [8].
-
Either open thoracotomy or video-assisted thoracoscopy (VATS) access can be used [9].
Radical radiotherapy or stereotactic radiotherapy (SABR) can be considered in patients unfit for surgery.
-
At present, the results from the use of SABR are promising in patients with tumors not-centrally located and with a size <5 cm who are unfit for surgery. Prospective trials of SABR versus primary resection in surgery-fit patients are now underway.
-
There is no indication for post-operative radiotherapy (PORT) in patients with completely resected N0 or N1 disease. Post-operative radiotherapy may be considered after adjuvant chemotherapy in selected patients with stage IIIAN2, although its precise contribution is yet to be defined. Post-operative radiotherapy may be indicated after incomplete surgery.
Nearly half of those patients who undergo surgical resection for early-stage NSCLC will later develop recurrent disease. The efficacy of adjuvant chemotherapy after surgical resection in early-stage is now well established [10, 11]. Adjuvant cisplatin-based chemotherapy is recommended in completely resected fit patients with stage II–III NSCLC. Most studies to date have used a two-drug combination with cisplatin. Efficacy of adjuvant chemotherapy in stage IB remains controversial, and adjuvant chemotherapy is not currently recommended in stage IA disease.
Therefore, the recommendations for adjuvant chemotherapy according to pathologic stage in early-stage NSCLC are as follows:
-
Adjuvant chemotherapy is not recommended in stage IA disease.
-
Four cycles of adjuvant cisplatin-based chemotherapy (a doublet combination) is recommended in completely resected fit patients with pathologic stage II–III.
-
Cisplatin-based chemotherapy may be considered in selected patients with stage IB disease.
In tumor-tissue specimens from resected patients, numerous molecular markers have been examined to address whether they may play a role in deciding which patients would be best treated with adjuvant chemotherapy and which drugs should be used. None of the markers analyzed to date, including immunohistochemistry staining for Excision Repair Cross Complementation Group 1 (ERCC1) have been prospectively validated in large cohorts and they should, therefore, not guide the indication for adjuvant therapy nor the choice of therapy [12].
Targeted agents should, at present, not be used in the adjuvant setting [13].
Stage III treatment
Stage III NSCLC treatment remains a very complex and controversial area due to the heterogeneity of different clinical, pathological and prognosis conditions, with presentations that range from apparently resectable tumors, to unresectable bulky ipsilateral multistation or contralateral nodal disease. Given the fact that definitive treatment recommendations may be difficult to make in this setting, patients must be referred to an expert multidisciplinary team for evaluation before any definitive treatment is decided (Fig. 1).

Treatment algorithm for stage III
Due to this substantial heterogeneity, stage III NSCLC has been classified into six subsets (Table 4).
Stage IIIAN2
-
For those incidental N2 metastases found on final pathology examination of the resection specimen, adjuvant chemotherapy should be given. PORT in pN2 patients has been shown to result in no clear difference in overall survival, but a small reduction in local recurrence. This issue is currently being prospectively studied in the LUNG-ART trial.
-
In those N2 (single station) metastases recognized intraoperatively, considered as technically resectable, primary lung resection as well as mediastinal lymphadenectomy must be completed, followed by adjuvant chemotherapy +/− PORT
-
Those non-bulky N2 patients (defining bulky as lymph nodes >2 cm in short-axis diameter, as measured by CT, groupings of multiple smaller lymph nodes, or involvement of >2 lymph node stations) can benefit from multimodality approach including surgery. Several small and early phase III trials have shown a significant improvement in survival for those patients treated with induction chemotherapy followed by surgery vs surgery alone. However, no standard induction chemotherapy regimen has emerged, and there is considerable variability in preferred regimens in routine practice. Two phase III trials completed in Europe and North America, addressing the potential benefit of adding surgery in the context of induction regimen (QT, QT/RT). Although in both trials surgery did not improve the outcome compared to thoracic radiotherapy, it may have a role in specific subsets of patients with clinically proven stage IIIA-N2 (downstaging, lobectomy) [14, 15].
-
The final subgroup of those bulky N2 disease are not candidates for surgery, and they are treated with the same combined proposals as stage IIIB
Stage IIIB
-
In PS 0–1 patients with stage IIIB or stage IIIA–N2 subset 4, several meta-analyses and phase III trials have showed that adding sequential or concomitant chemotherapy to radiotherapy alone improved survival [16].
Table 4 Subtyping of stage III disease -
In patients with good performance status and without significant weight loss, concurrent chemoradiotherapy at systemic doses is superior to sequential radiochemotherapy, but at the cost of manageable increased acute esophageal toxicity [17].
-
The addition of systemic chemotherapy to concurrent chemoradiotherapy, either as induction or as a consolidation has failed to improve survival rates compared to concurrent chemoradiotherapy [18, 19].
-
Cisplatin-based schedules are preferred. The most commonly used drugs together with cisplatin are etoposide (at full systemic dose) and vinorelbine (at reduced dose).
Stage IV
-
Two-drug, platinum-based chemotherapy combined with docetaxel, gemcitabine, paclitaxel, pemetrexed or vinorelbine prolongs survival, improves quality of life and controls symptoms in patients with good performance status. Non-platinum combination chemotherapy can be considered in patients who are not fit to receive platinum agents [20] (Figs. 2, 3).
Fig. 2 
Treatment algorithm for stage IV first-line therapy. *Criteria for treatment with bevacizumab + chemotherapy: non-squamous NSCLC, no clinically significant hemoptysis, no therapeutic anticoagulation and no medically uncontrolled hypertension. †There is evidence of superior efficacy and reduced toxicity for cisplatin/pemetrexed in patients with non-squamous histology, in comparison to cisplatin/gemcitabine [23]. ‡In two recent studies, maintenance therapy with pemetrexed (only in non-squamous histology) [24, 25] or erlotinib [26] increased survival in patients who has not progressed after 4 cycles of a platinum-based doublet
Fig. 3 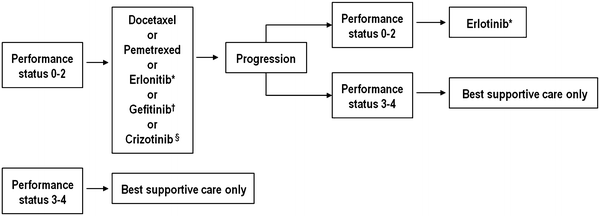
Treatment algorithm for Stage IV: second and third-line therapy. *Patients with a performance status of 3 were included in the National Cancer Institute of Canada-Clinical Trials Group (NCIC-CTG) trial BR.21. Erlotinib may be considered for PS 3 patients. †Only for patients harboring activating EGFR mutations. §Only for patients harboring ALK rearrangement
-
Several meta-analyses have showed higher RRs for cisplatin combinations when compared with carboplatin combinations. The overall survival (OS) was significantly superior for cisplatin in the subgroup of non-squamous tumors and in patients treated with third-generation regimens [21]
-
Timing and duration of palliative first-line treatment Chemotherapy should be initiated while the patient is in good performance status. Treatment should be stopped after no more than four cycles in patients not responding to therapy; in responding patients no more than six cycles are recommended.
-
The addition of bevacizumab to chemotherapy can be indicated in performance status 0–1 patients with non-squamous histology, except for patients with clinically significant haemoptysis, therapeutic anticoagulation or medically uncontrolled hypertension [22].
-
There is evidence of superior efficacy and reduced toxicity for cisplatin/pemetrexed in patients with non-squamous histology, in comparison to cisplatin/gemcitabine [23].
-
In two recent studies, maintenance therapy with pemetrexed (in patients with non-squamous histology who did not progress after 4 cycles of a platinum-based doublet with or without pemetrexed) [24, 25] or erlotinib (in patients with any histology who achieved stable disease after 4 cycles of a platinum-based doublet) [26] increased survival.
-
Therefore, platinum-based chemotherapy is the preferred option for elderly patients with PS 0–1 and adequate organ function [27], while a single-agent approach might remain the recommended treatment of elderly unfit or comorbid patients, who are more likely to present with more treatment-related adverse events.
-
In patients with performance status of 2, single-agent chemotherapy represents an option. Platinum-based combinations may be also considered as an alternative [28].
-
Second-line systemic treatment with docetaxel, erlotinib or pemetrexed (only in non-squamous histology) improves disease-related symptoms and survival.
-
Treatment with erlotinib may be recommended as third-line therapy for patients with performance status of 0–3 who have not received prior erlotinib or gefitinib [29].
-
Poor PS (PS 3–4) patients should be offered best supportive care in the absence of tumors with activating (sensitizing) EGFR mutations.
-
Resection of single metastases can be considered in selected cases.


Epidermal growth factor receptor (EGFR) mutations occur in about 10 % of NSCLC cancers from Western population [30]. Anaplastic lymphoma kinase (ALK) rearrangements are present in approximately 2–7 % of advanced NSCLC [31].
Epidermal growth factor receptor mutations are more common in females and never-smokers with adenocarcinoma tumor histology; however, a significant proportion of patients with these clinical characteristics do not harbor an EGFR mutation.
Patients with ALK rearrangements are also more frequent in non-smoker patients.
-
The use of diagnostic molecular studies, specifically for EGFR-activating mutations and ALK rearrangements as part of routine pathologic evaluation of lung cancer [4]
-
EGFR mutation/ALK rearrangement testing should be ordered at the time of diagnosis for patients presenting with advanced-stage disease who are suitable for therapy or at time of recurrence or progression in patients who originally presented with lower-stage disease, but were not previously tested
-
In patients with known EGFR-sensitive mutations and stage IV NSCLC, first-line therapy with an EGFR tyrosine kinase inhibitor (erlotinib or gefitinib) is recommended based on superior response rates, progression-free survival and toxicity profiles compared with platinum-based doublets [32–36].
Crizotinib is a dual ALK and Met inhibitor under study in patients with advanced NSCLC expressing the EML4-ALK fusion gene [37].
In a recent study crizotinib, as compared with chemotherapy, prolonged progression-free survival, increased response rates, and improved the quality of life in patients with advanced, previously treated ALK-positive tumors [37].
-
Patients with NSCLC harboring an ALK rearrangement should be considered for crizotinib, during the course of their disease [38].
Follow-up
After curative-intent therapy
-
In patients who have undergone curative-intent surgical resection, it is suggested that chest CT be performed every 6 months for the first 2 years after resection and every year thereafter (Grade 2C)
-
For patients who have undergone curative-intent therapy, routine surveillance with PET imaging, abdominal ultrasonography or biomarker testing is not recommended
After advanced disease
-
The optimal approach to post-treatment management of patients with NSCLC, including the role of radiological evaluation, is controversial, with very limited literature available.
-
Owing to the aggressive nature of this disease, generally close follow-up, at least every 6 weeks after the first-line therapy, is advised but should also depend on individual re-treatment options.
-
Given the clear benefits of second-line therapy in patients who presented an initial response to first-line chemotherapy and maintained a good PS, radiological follow-up should be considered every 6–12 weeks to allow for an early initiation of second-line therapy.
References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30.
Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International Association for the Study of Lung Cancer/American Thoracic Society. European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6:244–85.
Garrido P, de Castro J, Concha Á, Felip E, Isla D, López-Ríos F, et al. Guidelines for biomarker testing in advanced non-small cell lung cancer. A National Consensus of the Spanish Society of Medical Oncology (SEOM) and the Spanish Society of Pathology (SEAP). Clin Transl Oncol. 2012;14:338–49.
Lindeman NI, Cagle PT, Beasley MB, Chitale DA, Dacic S, Giaccone G, et al. Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol. 2013;8:823–59.
De Leyn P, Lardinois D, Van Schil P, Rami-Porta R, Passlick B, Zielinski M, et al. European trends in preoperative and intraoperative staging: ETS guidelines. J Thorac Oncol. 2007;2:357–61.
Goldstraw P, editor. IASLC staging manual in thoracic oncology. Florida: Editorial Rx Press; 2009.
Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60:615–22.
Darling GE, Allen MS, Decker PA, Ballman K, Malthaner RA, Inculet RI, et al. Randomized trial of mediastinal lymph node sampling versus complete lymphadenectomy during pulmonary resection in the patient with N0 or N1 (less than hilar) non-small cell carcinoma: results of the American College of Surgery Oncology Group Z0030 Trial. J Thorac Cardiovasc Surg. 2011;141:662–70.
Cao C, Manganas C, Ang SC, Peeceeyen S, Yan TD. Video-assisted thoracic surgery versus open thoracotomy for non-small cell lung cancer: a meta-analysis of propensity score-matched patients. Interact Cardiovasc Thorac Surg. 2013;16:244–9.
Arriagada R, Bergman B, Dunant A, Le Chevalier T, Pignon JP, Vansteenkiste J. The International Adjuvant Lung Cancer Trial Collaborative Group: Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med. 2004;350:351–60.
Pignon JP, Tribodet H, Scagliotti GV, Douillard JY, Shepherd FA, Stephens RJ, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552–9.
Friboulet L, Olaussen KA, Pignon JP, Shepherd FA, Tsao MS, Graziano S, et al. ERCC1 isoform expression and DNA repair in non-small cell lung cancer. N Engl J Med. 2013;368:1101–10.
Goss GD, Lorimer I, Tsao MS, O’Callaghan CJ, Ding K, Masters GA et al. A phase III randomized, double-blind, placebo-controlled trial of the epidermal growth factor receptor inhibitor gefitinb in completely resected stage IB-IIIA non-small cell lung cancer (NSCLC): NCIC CTG BR.19. J Clin Oncol 2010; 28(Suppl): LBA7005.
Albain KS, Swann RS, Rusch VW, Turrisi AT 3rd, Shepherd FA, Smith C, et al. Radiotherapy plus chemotherapy with or without surgical resection for stage III non-small-cell lung cancer: a phase III randomised controlled trial. Lancet. 2009;374:379–88.
van Meerbeeck JP, Kramer GW, Van Schil PE, Legrand C, Smit EF, Schramel F, et al. Randomized controlled trial of resection versus radiotherapy after induction chemotherapy in stage IIIA-N2 non-small cell lung cancer. J Natl Cancer Inst. 2007;99:442–50.
Pignon JP, Stewart LA. Randomized trials of radiotherapy alone versus combined chemotherapy and radiotherapy in stages IIIa and IIIb non-small cell lung cancer: a meta-analysis. Cancer. 1996;77:2413–4.
Aupérin A, Le Péchoux C, Rolland E, Curran WJ, Furuse K, Fournel P, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non–small-cell lung cancer. J Clin Oncol. 2010;28:2181–90.
Vokes EE, Herndon JE 2nd, Kelley MJ, Cicchetti MG, Ramnath N, Neill H, et al. Induction chemotherapy followed by chemoradiotherapy compared with chemoradiotherapy alone for regionally advanced unresectable stage III non-small cell lung cancer: cancer and Leukemia Group B. J Clin Oncol. 2007;25:1698–704.
Hanna N, Neubauer M, Yiannoutsos C, McGarry R, Arseneau J, Ansari R, et al. Phase III study of cisplatin, etoposide, and concurrent chest radiation with or without consolidation docetaxel in patients with inoperable stage III non-small cell lung cancer: the Hoosier Oncology Group and U.S. Oncology. J Clin Oncol. 2008;26:5755–60.
Peters S, Adjei AA, Gridelli C, Reck M, Kerr K, Felip E, et al, On behalf of the ESMO Guidelines Working Group. Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2012; 23(Suppl 7):vii56–64.
Ardizzoni A, Boni L, Tiseo M, Fossella FV, Schiller JH, Paesmans M. et al Cisplatin-versus carboplatin-based chemotherapy in first-line treatment of advanced non-small-cell lung cancer: an individual patient data meta-analysis. J Natl Cancer Inst. 2007;99:847–57.
Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small cell lung cancer. N Engl J Med. 2006;355:2542–50.
Scagliotti GV, Parikh P, von Pawel J, Biesma B, Vansteenkiste J, Manegold C, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naïve patients with advanced-stage NSCLC. J Clin Oncol. 2008;26:3543–51.
Paz-Ares L, de Marinis F, Dediu M, Thomas M, Pujol JL, Bidoli P, et al. Maintenance therapy with pemetrexed plus best supportive care versus placebo plus best supportive care after induction therapy with pemetrexed plus cisplatin for advanced non-squamous non-small cell lung cancer: a double-blind, phase 3, randomised controlled trial. Lancet Oncol. 2012;13:247–55.
Ciuleanu T, Brodowicz T, Zielinski C, Kim JH, Krzakowski M, Laack E, et al. Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care for non-small-cell lung cancer: a randomised, double-blind, phase 3 study. Lancet. 2009;374:1432–40.
Cappuzzo F, Ciuleanu T, Stelmakh L, Cicenas S, Szczésna A, Juhász E, et al. Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2010;11:521–9.
Quoix E, Zalcman G, Oster JP, Westeel V, Pichon E, Lavolé A, et al. Carboplatin and weekly paclitaxel doublet chemotherapy compared with monotherapy in elderly patients with advanced non-small-cell lung cancer: IFCT-0501 randomised, phase 3 trial. Lancet. 2011;378:1079–88.
Lilenbaum R, Mauro M, Pereira JR, Barrios CH, De Albuquerque Ribeiro R, de Mendonça Beato CA et al. A randomized phase III trial of single agent pemetrexed (P) versus carboplatin and pemetrexed (CP) in patients with advanced non-small cell lung cancer (NSCLC) and performance status (PS) of 2. J Clin Oncol. 2012;30:abstr 7506.
Shepherd FA. Rodrigues Pereira J, Ciuleanu T, Tan EH, Hirsh V, Thongprasert S et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353:123–32.
Rosell R, Moran T, Queralt C, Porta R, Cardenal F, Camps C, et al. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361(10):958–67.
Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363(18):1693–703.
Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–57.
Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. West Japan Oncology Group. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11(2):121–8.
Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al. North-East Japan Study Group. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362(25):2380–8.
Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–46.
Han JY, Park K, Kim SW, Lee DH, Kim HY, Kim HT, et al. First-SIGNAL: first-line single-agent IRESSA versus gemcitabine and cisplatin trial in never-smokers with adenocarcinoma of the lung. J Clin Oncol. 2012;30(10):1122–8.
Shaw AT, Yeap BY, Solomon BJ, Riely GJ, Gainor J, Engelman JA, et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. Lancet Oncol. 2011;12:1004–12.
Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó L, Ahn MJ, et al. Crizotinib versus Chemotherapy in Advanced ALK-Positive Lung Cancer. N Engl J Med. 2013;368(25):2385–94.
Andre F, Grunenwald D, Pignon JP et al. Survival of patients with resected N2 non-small-cell lung cancer: evidence for a subclassification and implications. J Clin Oncol 2000;18:2981–9.
Conflict of interest
The authors declare that they have no conflict of interest relating to the publication of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Appendix: Clinical Guideline Working Group on behalf of the Spanish Society of Medical Oncology (SEOM) Executive Committee 2011–2013
Appendix: Clinical Guideline Working Group on behalf of the Spanish Society of Medical Oncology (SEOM) Executive Committee 2011–2013
Juan Jesús Cruz, Pilar Garrido, Agustí Barnadas, Pablo Borrega, Francisco Javier Barón, Elvira del Barco, Rocio García-Carbonero, Jesús Garcia-Mata, Encarnación Gonzalez, Pilar Lianes, Antonio Llombart y Fernando Rivera.
Rights and permissions
About this article
Cite this article
Camps, C., Felip, E., García-Campelo, R. et al. SEOM clinical guidelines for the treatment of non-small cell lung cancer (NSCLC) 2013. Clin Transl Oncol 15, 977–984 (2013). https://doi.org/10.1007/s12094-013-1085-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-013-1085-2