
Abstract
Background and aims
Liver cancer is a detrimental complication in patients with chronic viral hepatitis and alcoholic or nonalcoholic fatty liver disease (NAFLD). However, metabolic risk factors underlying NAFLD usually cause substantial differences in their clinical outcomes. Recently, several studies have used a novel definition of metabolic dysfunction-associated fatty liver disease (MAFLD) to reassess patients with NAFLD and pointed out the importance of metabolic risk factors. Since patients with NAFLD, MAFLD, or metabolic syndrome (MetS) have different burden of metabolic risk factors, it is crucial to decipher the risk of developing hepatic complications in these populations.
Methods
Through a longitudinal nationwide cohort study, the risk of liver cancer was investigated in patients with MetS alone, NAFLD alone, overlap NAFLD/MAFLD, and coexisting MetS and NAFLD. The general characteristics, comorbidities, and incidence of liver cancer were also compared.
Results
Intriguingly, patients diagnosed with MetS alone did not have a significant risk of developing HCC compared to control individuals, while patients with NAFLD alone, NAFLD/MAFLD, and coexisting NAFLD and MetS exhibited 6.08-, 5.81-, and 15.33-fold risks of developing HCC, respectively. Apart from metabolic risk factors, renal function status and liver cirrhosis were the independent risk factors for the development of HCC among these groups.
Conclusion
Our data emphasize that metabolic dysfunction has a significant impact on hepatocarcinogenesis in patients with NAFLD. Moreover, coexisting multiple metabolic risk factors would dampen the risk of developing HCC in patients with NAFLD. Closely tracing HCC formation through laboratory examination or imaging is crucial in these patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common malignancy among all cancer types and causes one-third of cancer-associated deaths worldwide [1, 2]. Geographically, Asian countries such as China, Japan and Taiwan are endemic areas for liver cancers in comparison to Western countries, which could be explained by hepatotropic viruses such as hepatitis B and hepatitis C [3].
Apart from virus-derived HCC, nonalcoholic fatty liver disease (NAFLD) has become an emerging cause of HCC in Western and Asian countries. Based on community studies in Taiwan, the prevalence of NAFLD varied from approximately 11.5% to 57.8% [4, 5]. The current diagnostic criteria for NAFLD are established by excluding all known causes of hepatitis, such as viruses, toxic autoimmune disorders, or excessive alcohol consumption. It is not mandatory for the presence of metabolic risk factors in patients with NAFLD. Accordingly, serum biomarkers, imaging, and histopathological examinations are required to confirm this diagnosis [6]. Many epidemiological studies have demonstrated a steady increase in the incidence and prevalence of HCC in patients with NAFLD globally, and currently, NAFLD-derived HCC has become the third leading cause of HCC in the USA. It is anticipated that it will become the most common cause of HCC after two decades [7]. Another retrospective study in the UK that included 632 HCC cases demonstrated a similar trend: the incidence of NAFLD-derived HCC increased five times more than that of HCC derived from other causes of liver disease between 2000 and 2010 [8]. In Asian countries, lifestyle changes have led to gradually increasing numbers of NAFLD and nonalcoholic steatohepatitis (NASH), the most severe form of NAFLD-derived HCC [9]. A population-based cohort study conducted in Taiwan demonstrated that NAFLD is an important and easily ignored risk factor in Taiwan apart from virus-driven HCC [10].
Since patients with NAFLD have broad-spectrum diseases ranging from NAFLD or simple steatosis to nonalcoholic steatohepatitis, intra/extrahepatic complications and outcomes vary among patients with NAFLD [11]. Recently, metabolic dysfunction-associated liver disease (MAFLD), proposed by the international consensus, highlights the impact of several metabolic risk factors on the intra/extrahepatic complications and outcomes in patients with fatty liver diseases [6, 11,12,13]. In the current definition, MAFLD is diagnosed on the basis of the following criteria: patients with hepatic steatosis simultaneously presented with one or more following status: (1) overweight/obesity, (2) type 2 diabetes mellitus, or (3) at least two metabolic dysregulations (e.g., hypertension, dyslipidemia, and waist circumference ≥ 90 and 80 cm in men and women, respectively, and so on). According to the statistical results, the prevalence rate of MAFLD varies between 12 and 30% in different Asian countries [12, 14, 15]. Regarding MAFLD-derived complications, a population-based study from the USA showed an increased risk of all-cause mortality, especially in cardiovascular complications, and associated mortality was observed in patients with MAFLD, whereas this notion was not found in patients with NAFLD [16]. Additionally, MAFLD-derived HCC accounts for approximately 2% and 12.2% of all HCC cases in Japan and South Korea, respectively [17, 18].
Metabolic syndrome (MetS), a cluster of multiple metabolic risk factors, has also been considered as a predictor of NAFLD [9, 19] and recognized as a risk factor for the development of colon cancer, breast cancer, etc., despite the fact that the incidence of HCC in patients with MetS is still controversial. Intriguingly, a part of the patients with MAFLD did not meet the criteria for MetS because they only had fewer metabolic risk factors (less burden of metabolic dysfunction) than those with MetS according to the ATPIII MetS diagnostic criteria. It raised an interesting question on whether the severity of metabolic risk factors would affect the risk of developing HCC. Furthermore, it remains unclear whether the risk of HCC increased in the population with coexisting MetS and NAFLD compared to the population with less metabolic risk factors only (MetS alone) or fatty liver disease only (NAFLD alone). This study aimed to determine the risk of HCC among different groups consisting of patients with fatty liver disease or different severities of metabolic risk factors using a large longitudinal database.
Methods
Database description
The National Health Insurance (NHI) Program was established on March 1, 1995, and covers more than 99% of the 23.72 million people in Taiwan. The Longitudinal Health Insurance Database (LHID) of the NHI Research Database in Taiwan includes one million individuals randomly selected from the Registry for Beneficiaries, which contains the complete medical records of each case. Regarding disease coding, the LHID was released by the NHRI, and the institute provides detailed examinations of International Classification of Diseases, Ninth Revision (ICD-9-CM) codes. Additionally, this database has reported that there is no significant difference in age, sex, or health-care costs between the selected cohort in the present study and other cases enrolled in the NHI program.
Sampled participants and study design
Identification of the NAFLD group without metabolic risk factors (NAFLD alone)
The selection criteria of NAFLD group in NHIRD was used according to a previous literature [10]. Generally, we selected patients 18 years of age or older with a first diagnosis of NAFLD by using ICD-9-CM codes 571.40, 573.3, and 571.8 from the LHID. For exclusion criteria, individuals with other causes of hepatitis (ICD codes ICD-9-CM 303.9, 571.0–571.3, V11.3, and V79.1), those with viral hepatitis (070, 573.1, V02.6, and V05.3), those with human immunodeficiency virus infection and infectious hepatitis (042 and 573.2) and other causes such as toxic hepatitis (573.3), primary biliary cirrhosis (571.6) and autoimmune hepatitis (571.42) from these cohorts, or age less than 18 years old before the index dates were excluded. To augment the precision of diagnosis of NAFLD, the diagnostic codes mentioned above for NAFLD were confirmed at least three times during the period of this study. In addition, we excluded cases with missing age or sex information at baseline for meeting the current diagnostic criteria of NAFLD. Otherwise, all cases with any metabolic risk factors including hypertension, type 2 diabetes, obesity, and dyslipidemia were excluded. The index date for each NAFLD case was the date of diagnosis.
Identification of metabolic syndrome in the NHIRD
Metabolic syndrome (MetS) consists of increasing blood pressure/hypertension, dyslipidemia (increased triglycerides and lowered high-density lipoprotein cholesterol), elevated fasting glucose and central obesity. Since there is no ICD-9 CM code for MetS in the NHIRD, the identification of MetS in the NHIRD was used by combining all different disease codes below, which was also implemented by a previous study [20]. These disease codes contain (1) hypertension (ICD-9 codes 401–405), defined as a blood pressure ≥ 130/85 mmHg, (2) diabetes mellitus (DM; ICD-9 code 250.x) and insulin resistance (ICD-9 code 277.7), defined as a fasting plasma glucose ≥ 110 mg/dL, (3) coronary artery diseases (ICD-9 codes 414.0, 414.0x, 414.2, 414.3, 414.4, 414.8 and 414.9) and (4) hyperlipidemia (ICD-9 codes 272.0, 272.1, 272.2, 272.4 and 272.9), defined as fasting triglycerides ≥ 150 mg/dL. If the cases were coded with some disease codes before the index date, they were excluded from this study. The inclusion criterion of obesity was defined by the ICD9-CM code (278.0) [21]. The patients who received the following surgical approaches such as open gastroplasty (OP44.69), laparoscopic vertical banded gastroplasty (OP44.68), laparoscopic adjustable gastric band (OP44.95), and sleeve gastrectomy (OP43.89) were excluded from this study. Additionally, all disease codes of the cases enrolled in this study were identified at least three times within 1 year, which avoids miscoding.
Identification of the overlap of the NAFLD and MAFLD group
Since there was no direct ICD-9 CM code for the diagnosis of MAFLD in our database, the coexisting NAFLD and MAFLD group in this study was classified on the basis of the consensus guideline: the cases were diagnosed as (1) coexisting NAFLD and hypertension/hyperlipidemia, (2) NAFLD and type 2 diabetes, or (3) NAFLD and obesity. All ICD-9 CM codes were mentioned previously, and these codes were confirmed at least three times during the study period. Moreover, we excluded cases with missing age or sex information at baseline.
Study design, events, and comorbidities assessment
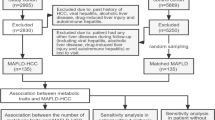
According to the method and ICD code for identification, our study group was defined as the cohort diagnosed with metabolic syndrome (MetS) and NAFLD together. The comparison groups were classified into four different populations: the population with either MetS or NAFLD or overlap NAFLD/MAFLD and the individuals without MetS and NAFLD (control population). The detailed design, inclusion and exclusion criteria and tracking time are described in Fig. 1. Follow-up was calculated in person-years for each patient until any hepatocellular carcinoma was diagnosed (ICD-9-CM codes: 155.0), the patient withdrew from the insurance system, or until the end of 2013. All comorbidities in this study were listed as below: COPD (ICD-9-CM codes 491, 492, 496), heart failure (ICD-9-CM code 428), stroke (ICD-9-CM codes: 430–438), thrombocytopenia (ICD-9-CM codes: 287.5), hyperbilirubinemia (ICD-9-CM codes: 782.4), cirrhosis of liver (ICD-9-CM codes: 571.5) chronic renal failure, (ICD-9-CM codes:585.9), end-stage renal disease/ESRD (ICD-9-CM codes:V45.11 and 585.6). Additionally, the comorbidities were also scored by the Charlson Comorbidity Index removing the parameters of metabolic syndrome (CCI_R).

The flowchart of study design from national health insurance database in Taiwan
Statistical analysis
The statistical software is the Statistical Product and Service Solutions 20th edition (Armonk, NY: IBM Corp.). Categorical variables were compared by the Chi-square or Fisher exact test, and continuous variables were compared by one-way ANOVA among these groups. The cumulative risk of hepatocellular carcinoma was demonstrated by Kaplan–Meier curves and verified by the log-rank test. p values less than 0.05 were regarded as statistically significant. The adjusted hazard ratios of hepatocellular carcinoma for the parameters were presented by applying the Cox regression hazard model.
Results
Initially, 9219 individuals were enrolled by the inclusion criteria. After excluding subjects based on certain criteria, the study arm in this study included a total of 6724 patients who had NAFLD and MetS. Regarding the demographic characteristics among all groups, there was no significant difference in the age and gender distribution, while in terms of the CCI-R scores, apparently, the study population that had MetS and NAFLD together had higher scores than those in the other populations. Otherwise, the incidence of most comorbidities, including liver cirrhosis, COPD, heart failure, stroke, thrombocytopenia, hyperbilirubinemia, chronic renal failure, and ESRD, was higher in the population with coexisting MetS and NAFLD than in those with MetS alone or control individuals (Table 1).
The mean follow-up was 7.16 years (SD = 8.69), 8.62 years (SD = 9.37), 6.17 years (SD = 4.82) and 8.29 years (SD = 9.48) in the study group (MetS and NAFLD), the patients with NAFLD alone, the patients with MetS alone and control individuals, respectively. Regarding the incidence of HCC, 2155, 901, 746, 140, and 96 cases were diagnosed with HCC in the NAFLD/MetS population, NAFLD alone population, NAFLD/MAFLD population, MetS alone population and control individuals during their tracing period, respectively. Since patients with MetS and NAFLD had the worst outcome than that in other groups, we examined the risk of developing HCC between these two factors–MetS and NAFLD. Table 2 reveals the hazard ratio of developing HCC as analyzed by the joint effect between NAFLD and MetS after adjusting for age, sex, other comorbidities, and CCI_R. Individuals with MetS and NAFLD exhibited a 15.33-fold increased risk (95% CI 12.08–18.24, p < 0.001) of developing HCC compared with the individuals without metabolic risk factors and NAFLD. Otherwise, among individuals with NAFLD alone, the aHR for HCC was a 6.08-fold increased risk in comparison with the control individuals (95% CI 4.91–7.62). This result emphasized that coexisting MetS in NAFLD patients dampens the risk of developing HCC. We also examined different components of MetS in the NHIR database to assess the impact of different metabolic risk factors on the incidence of HCC. Clearly, the aHR for HCC had a 3.4-fold, 7.26-fold, 2.64-fold, and 11.82-fold increase among groups with obesity, hypertension, dyslipidemia, and type 2 diabetes, respectively (Supplementary Table 1).
In Fig. 2, apparently, the mean time for developing HCC in individuals with MetS and NAFLD was 0.65 years (SD = 1.55), while this time in the groups with NAFLD alone, MetS alone and the reference group was 1.49 years (SD = 2.92), 5.38 years (SD = 3.94) and 4.35 years (SD = 3.94), respectively. According to the results of a previous epidemiological study, age was an important predisposing factor in the development of HCC in patients with NAFLD. Supplementary Table 2 demonstrates the distribution of HCC cases stratified by different age groups. In the groups whose ages were approximately 50–59, 60–69, and 70–79 years, the incidence rates of HCC were 35.09%, 41.25% and 31.98%, respectively. Approximately, 80% of HCC cases were observed in NAFLD and MetS individuals aged more than 50 years. Figure 3a shows that the incidence rate of developing HCC is significantly higher in patients with MetS and NAFLD aged more than 50 years than in the younger population (age less than 50 years).

Kaplan–Meier analysis of the cumulative risk of HCC among patients aged 20 and over stratified by different study groups with the log-rank test. Study cohort: with MetS, with NAFLD. Comparison cohort 1: Patients with NAFLD alone. Comparison cohort 2: Patients with MetS alone. Comparison cohort 3: Cases without NAFLD/MetS. Comparison cohort 4: Cases without NAFLD/MAFLD. Log-rank test: study cohort (patients with NAFLD and MetS) vs. Comparison Group 3 (patients without NAFLD/MetS): P < 0.001; Comparison Group 1 (Patients with NAFLD alone) vs. Comparison Group 3 (patients without NAFLD/MetS): P < 0.001; Comparison Group 2 (patients with MetS alone) vs. Comparison Group 3 (Patients without NAFLD/MetS): P = 0.894

Kaplan–Meier analysis of the cumulative risk of HCC among patients with NAFLD and MetS stratified by age (a) or obesity (b)
Table 3 reveals the HR of developing HCC among different populations after adjusting gender, age CCI_R and multiple comorbidities. Patients with coexisting MetS NAFLD had a 15.01-fold increased risk of HCC compared to the group without NAFLD and MetS, while the aHR only achieved a 2.40-fold increased risk of HCC in the patients with NAFLD and MetS compared to the patients with NAFLD only. Additionally, the presence of NAFLD had a 9.97-fold increased risk of developing HCC in the patients diagnosed of MetS compared to that in the group with MetS alone. In multivariable analysis, male gender, high CCI_R score, status of cirrhosis, renal function impairment had a significant impact on the incidence rate of HCC among these three comparisons. Since obesity is also a crucial factor in MetS, to investigate the effect of obesity on developing HCC in the population with MetS and NAFLD, different ICD9-CM codes and operative codes were utilized for subgroup analysis. In Fig. 3b, there was no significant difference in the incidence of HCC between the obese and nonobese groups of patients with NAFLD and MetS.
MAFLD has been proposed as an appropriate classification of fatty liver diseases [13]. In line with this, we examined the risk of developing HCC among the overlap NAFLD/MAFLD cases compared to NAFLD alone and control populations. As shown in Table 4, there was a 6.08-fold and 5.81-fold increased risk of developing HCC among patients diagnosed with NAFLD alone and NAFLD/MAFLD, respectively. Regarding the risk of liver cirrhosis, NAFLD alone and NAFLD/MAFLD cases had a 4.58-fold and 3.57-fold increased risk, respectively. Given that renal function has been shown to be an independent risk factor for developing HCC among our study populations, we stratified the overlap NAFLD/MAFLD populations by their renal function. As shown in Supplementary Table 3, patients with renal function impairment (mild to moderate) and end-stage renal disease presented with a higher risk of developing HCC or liver cirrhosis. Since there was a correlation between renal function and FIB-4 fibrotic score in the NAFLD population [22, 23], we also examined the association between renal function status and the risk of HCC and liver cirrhosis in patients with NAFLD/MAFLD. As shown in Supplementary Table 4, there was also a positive correlation between impairment of renal function and risk of developing these detrimental complications in patients with NAFLD/MAFLD.
Discussion
The current study utilized a large sample size and sufficient tracking time to elucidate the incidence of hepatic complications among populations with different severities of metabolic risk factors. We demonstrated that there was no statistical significance in the risk of developing HCC in patients with MetS alone compared to the control individuals, whereas the risks of developing HCC in patients with NAFLD alone and patients with coexisting NAFLD and MetS was higher than that in the control individuals, with aHR values of 6.08 and 15.33, respectively. Furthermore, the risk of developing cirrhosis of the liver or HCC among patients diagnosed with NAFLD alone and NAFLD/MAFLD was similar. Collectively, our data emphasize that metabolic risk factors are an important predisposing factor in patients with NAFLD for the development of HCC. Coexisting NAFLD in patients with multiple metabolic risk factors (Metabolic syndrome status) would dampen the risk of HCC compared to that in the MetS alone population.
MetS containing multiple metabolic risk factors, has been recognized as a common predisposing factor for ischemic heart disease, cerebrovascular diseases, and several malignancies [24, 25]. The systemic effect of MetS was proposed to occur through hyperinsulinemia, insulin resistance, chronic inflammatory cytokine production or apoptotic suppression. Insulin resistance causes metabolic stress and several systemic consequences in different tissues and organs, such as subcutaneous/visceral adipose tissues, liver, muscle, and pancreas [26, 27]. Accordingly, overnutrition causes lipid accumulation in muscle, liver, and adipose tissue, which drives lipotoxicity and insulin resistance. Subsequently, the chronic inflammatory response derived from inflammatory cytokines and innate and adaptive immune cells aggravates these consequences and forms a vicious cycle.
The risk of developing all kinds of cancer in MetS population has been considered and investigated. A meta-analysis of 38,940 patients with cancer demonstrated that MetS exhibited a 1.43-, 1.25- and 1.10-fold increased risk of developing liver cancer, colorectal cancer and bladder cancer, respectively [28]. Another meta-analysis that analyzed 18 cohorts and 1 case–control study also revealed that the relative risk of developing HCC in patients with MetS was 1.76 from 11 studies [29]. Although these data provided evidence regarding the positive association between MetS and the incidence of HCC, there are still several large sample size studies demonstrating no significant association between MetS and HCC [30,31,32]. The possible explanation for this difference could be considered that some previous studies did not entirely exclude NAFLD/NASH or hepatitis in their MetS cohorts, which might interfere with their results. Intriguingly, our results also indicated that patients diagnosed with MetS alone did not have a significantly greater risk of developing HCC compared to the control individuals, whereas the risk of developing HCC significantly increased in patients with NAFLD alone, NAFLD/MAFLD, and coexisting MetS/NAFLD. These data suggest that NAFLD could be a possible prerequisite in the MetS group during the development of HCC. Accordingly, it also points out that NAFLD-derived chronic hepatic inflammation would be a necessary step for hepatocarcinogenesis, while metabolic risk factors serve as aggravated factors for dampening this process.
Our study also demonstrated that patients with coexisting NAFLD/MAFLD or NAFLD alone had a similar trend in the risk for developing HCC or liver cirrhosis, whereas the risk for developing HCC in our NAFLD population with coexisting MetS was higher than that in patients with NAFLD/MAFLD or NAFLD alone. A possible explanation would be that more comorbidities were defined in our MetS population than in the MAFLD population. This also reflects that the different metabolic stresses aggravate the risk of developing HCC in the NAFLD population. Furthermore, several studies demonstrated patients with NAFLD alone did not have an increased risk for developing hepatic complications such as cirrhosis of liver [33, 34], which is different from the result in our study. The possible reason for this result could be considered that most NAFLD only cases in this study would be steatohepatitis patients or cases already had hepatic features such as elevated liver enzymes due to the method we used for defining NAFLD, which also means most of asymptomatic NAFLD cases (steatosis only) might be missed in this study.
During mean follow-up of 7.16–8.62 years, the mean time for HCC development in patients with NAFLD alone and coexisting NAFLD and MetS were 1.65 years and 0.65 year, respectively.(Fig. 2) This data demonstrated that most HCCs were found during the first 2 years in both cohorts. It was also anticipated that this time was shortened by approximately 0.65 years in patients with coexisting MetS and NAFLD, which could be explained by our MetS population had many predisposing factors for developing HCC such as hypertension, diabetes, and hyperlipidemia etc. Additionally, our NAFLD alone, MetS alone or coexisting NAFLD/MetS populations could visit hospital frequently due to hepatic manifestations or multiple comorbidities, which indirectly increase the chance for HCC identification. Collectively, even though there were still some bias in study population selection, these data supported the evidence that hepatic manifestation-metabolic risk factor could be an important predisposing factor for HCC formation either in the normal population or in the NAFLD population.
Obesity is an important metabolic risk factor and serves as a component of MAFLD or MetS. A meta-analysis reviewed 11 different cohort studies in Europe, the United States and Asia and revealed that overweight and obese status were significant risk factors for developing HCC [35]. Despite this evidence between obesity and HCC, some patients with NAFLD who had severe abnormalities in their metabolic profiles, such as lipids or glucose, did not present any overweight or obesity (lean NAFLD) [36,37,38]. In line with this, it is worth understanding the impact of obesity on the risk of HCC between normal weight group and obese populations among the patients with coexisting NAFLD/MetS. Our data indicated that this risk is similar between the two subgroups, which means that regardless of obese status, early recognition of HCC by imaging and tumor marker examination is required in NAFLD patients with metabolic risk factors. Furthermore, as shown in Supplementary Table 3, the subgroup analysis demonstrated that the aHR increased among the patients with overlap NAFLD/MAFLD with renal function impairment and ESRD. Accordingly, patients with worse renal function have a higher risk of developing HCC. Previously, few studies have demonstrated a positive correlation between renal function and FIB-4 fibrosis score. It is worth establishing a scoring system for these metabolic risk factors to predict the risk of hepatocarcinogenesis or liver cirrhosis.
There are several limitations and missing information in this study. First, the NHIR database does not contain detailed information for patients with MetS or NAFLD regarding smoking habits, body mass index, physical inactivity (sedentary lifestyle), waist circumference, central obesity and cytogenetic or molecular testing results for prognosis markers, which means some MetS cases with less severity could be missed. Alternatively, we used the obesity ICD9-CM code and relative surgical procedure codes, such as gastric bypass surgery, which was only performed in obese patients based on the criteria of the national health system in Taiwan. Second, our study lacked a detailed laboratory assessment for MetS and for NAFLD, including blood glucose, lipid data (triglyceride, cholesterol, HDL/LDL), biochemistry data, white blood cell counts, hemoglobin levels, and platelet values. Third, there were no imaging data, pathological severity scores, fibrosis status, or therapeutic strategies for the NAFLD population in this study, which means that few patients with early-stage NASH were still in our NAFLD population. However, due to the large sample sizes in this study, the results in this study still provide evidence of confidence in establishing the association between MetS, NAFLD, MAFLD, and HCC. Finally, this retrospective cohort study has relatively lower statistical quality and evidence than detailed registry studies, despite the strict ICD-9-CM coding.
Data availability
Not applicable.
Change history
16 February 2022
A Correction to this paper has been published: https://doi.org/10.1007/s12072-022-10308-9
References
Yang J, Zhang JX, Wang H, Wang GL, Hu QG, Zheng QC. Hepatocellular carcinoma and macrophage interaction induced tumor immunosuppression via Treg requires TLR4 signaling. World J Gastroenterol. 2012;18(23):2938–2947
Koulouris A, Tsagkaris C, Spyrou V, Pappa E, Troullinou A, Nikolaou M. Hepatocellular carcinoma: an overview of the changing landscape of treatment options. J Hepatocell Carcinoma. 2021;8:387–401
Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1
Chen CH, Huang MH, Yang JC, et al. Prevalence and risk factors of nonalcoholic fatty liver disease in an adult population of Taiwan: metabolic significance of nonalcoholic fatty liver disease in nonobese adults. J Clin Gastroenterol. 2006;40(8):745–752
Hsiao PJ, Kuo KK, Shin SJ, et al. Significant correlations between severe fatty liver and risk factors for metabolic syndrome. J Gastroenterol Hepatol. 2007;22(12):2118–2123
Kawaguchi T, Tsutsumi T, Nakano D, Torimura T. MAFLD: Renovation of clinical practice and disease awareness of fatty liver. Hepatol Res. 2021.
Neuschwander-Tetri BA. Hepatic lipotoxicity and the pathogenesis of nonalcoholic steatohepatitis: the central role of nontriglyceride fatty acid metabolites. Hepatology. 2010;52(2):774–788
Dyson J, Jaques B, Chattopadyhay D, et al. Hepatocellular cancer: the impact of obesity, type 2 diabetes and a multidisciplinary team. J Hepatol. 2014;60(1):110–117
Fan JG, Kim SU, Wong VW. New trends on obesity and NAFLD in Asia. J Hepatol. 2017;67(4):862–873
Lee TY, Wu JC, Yu SH, Lin JT, Wu MS, Wu CY. The occurrence of hepatocellular carcinoma in different risk stratifications of clinically noncirrhotic nonalcoholic fatty liver disease. Int J Cancer. 2017;141(7):1307–1314
Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209
Eslam M, Sarin SK, Wong VW, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. 2020;14(6):889–919
Wong VW, Lazarus JV. Prognosis of MAFLD vs. NAFLD and implications for a nomenclature change. J Hepatol. 2021.
Wei JL, Leung JC, Loong TC, et al. Prevalence and severity of nonalcoholic fatty liver disease in non-obese patients: a population study using proton-magnetic resonance spectroscopy. Am J Gastroenterol. 2015;110(9):1306–1314
Jeong EH, Jun DW, Cho YK, et al. Regional prevalence of non-alcoholic fatty liver disease in Seoul and Gyeonggi-do. Korea Clin Mol Hepatol. 2013;19(3):266–272
Kim D, Konyn P, Sandhu KK, Dennis BB, Cheung AC, Ahmed A. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J Hepatol. 2021.
Cho EJ, Kwack MS, Jang ES, et al. Relative etiological role of prior hepatitis B virus infection and nonalcoholic fatty liver disease in the development of non-B non-C hepatocellular carcinoma in a hepatitis B-endemic area. Digestion. 2011;84(Suppl 1):17–22
Hashimoto E, Tokushige K. Hepatocellular carcinoma in non-alcoholic steatohepatitis: growing evidence of an epidemic? Hepatol Res. 2012;42(1):1–14
Hamaguchi M, Kojima T, Takeda N, et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann Intern Med. 2005;143(10):722–728
Lee CY, Chen HC, Lin HW, et al. Blepharitis as an early sign of metabolic syndrome: a nationwide population-based study. Br J Ophthalmol. 2018;102(9):1283–1287
Chiou GJ, Huang DS, Hu FR, et al. Metabolic syndromes as important comorbidities in patients of inherited retinal degenerations: experiences from the nationwide health database and a large hospital-based cohort. Int J Environ Res Public Health. 2021;18(4):2065
Xu HW, Hsu YC, Chang CH, Wei KL, Lin CL. High FIB-4 index as an independent risk factor of prevalent chronic kidney disease in patients with nonalcoholic fatty liver disease. Hepatol Int. 2016;10(2):340–346
Sumida Y, Yoneda M, Tokushige K, et al. FIB-4 first in the diagnostic algorithm of metabolic-dysfunction-associated fatty liver disease in the era of the global metabodemic. Life (Basel). 2021;11(2):143
Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365(9468):1415–1428
Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL. Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Ther Adv Cardiovasc Dis. 2017;11(8):215–225
Williams KH, Shackel NA, Gorrell MD, McLennan SV, Twigg SM. Diabetes and nonalcoholic Fatty liver disease: a pathogenic duo. Endocr Rev. 2013;34(1):84–129
Morita M, Gravel SP, Chenard V, et al. mTORC1 controls mitochondrial activity and biogenesis through 4E-BP-dependent translational regulation. Cell Metab. 2013;18(5):698–711
Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. 2012;35(11):2402–2411
Ren H, Wang J, Gao Y, Yang F, Huang W. Metabolic syndrome and liver-related events: a systematic review and meta-analysis. BMC Endocr Disord. 2019;19(1):40
Ko S, Yoon SJ, Kim D, Kim AR, Kim EJ, Seo HY. Metabolic risk profile and cancer in Korean men and women. J Prev Med Public Health. 2016;49(3):143–152
Chen CT, Chen JY, Wang JH, et al. Diabetes mellitus, metabolic syndrome and obesity are not significant risk factors for hepatocellular carcinoma in an HBV- and HCV-endemic area of Southern Taiwan. Kaohsiung J Med Sci. 2013;29(8):451–459
Bitzur R, Brenner R, Maor E, et al. Metabolic syndrome, obesity, and the risk of cancer development. Eur J Intern Med. 2016;34:89–93
van Kleef L, Ayada I, Alferink L, Pan Q, de Knegt R. Metabolic dysfunction associated fatty liver disease improves detection of high liver stiffness: the rotterdam study. Hepatology. 2021.
Yamamura S, Eslam M, Kawaguchi T, et al. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD. Liver Int. 2020;40(12):3018–3030
Gupta A, Das A, Majumder K, et al. Obesity is independently associated with increased risk of hepatocellular cancer-related mortality: a systematic review and meta-analysis. Am J Clin Oncol. 2018;41(9):874–881
Pagadala MR, McCullough AJ. Non-alcoholic fatty liver disease and obesity: not all about body mass index. Am J Gastroenterol. 2012;107(12):1859–1861
Chon CW, Kim BS, Cho YK, et al. Effect of nonalcoholic Fatty liver disease on the development of type 2 diabetes in nonobese, nondiabetic Korean men. Gut Liver. 2012;6(3):368–373
Younossi ZM, Stepanova M, Negro F, et al. Nonalcoholic fatty liver disease in lean individuals in the United States. Medicine (Baltimore). 2012;91(6):319–327
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors made substantive intellectual contributions to this study to qualify as authors. CWY and YGC designed the study. CWC and CHC performed statistical analysis. An initial draft of the manuscript was written by YGC. WLC, CLH, CHC, and CWC redrafted parts of the manuscript and provided helpful advice on the final revision. All authors were involved in writing the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
Yu-Guang Chen, Chih-Wei Yang, Chi-Hsiang Chung, Ching-Liang Ho, Wei-Liang Chen and Wu-Chien Chien declare no competing financial interests.
Ethical approval
The study design, case enrollment and data analysis were approved by the Institutional Review Board (IRB) of Tri-Service General Hospital, Taiwan, Republic of China. The registration number is TSGH-IRB No. B-109–26.
Animal research
Not applicable.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Plant reproducibility
Not applicable.
Clinical trials registration
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chen, YG., Yang, CW., Chung, CH. et al. The association between metabolic risk factors, nonalcoholic fatty liver disease, and the incidence of liver cancer: a nationwide population-based cohort study. Hepatol Int 16, 807–816 (2022). https://doi.org/10.1007/s12072-021-10281-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12072-021-10281-9