
Abstract
The aim of this study was to evaluate sphenoid sinus pneumatisation and its anatomical relation with adjacent neurovascular structures in Indian population. We performed a retrospective cross-sectional study, in which the pattern of sphenoid sinus pneumatization was studied on high-resolution computed tomography scans (n = 400), and association of the optic nerve, vidian canal and foramen rotundum along with related morphometric measurements were studied. Out of 400 CT scans, 60.5% were males. Majority had sellar type of pneumatization (89.5%) and single intersinus septum (68%). The most common configuration of relation of optic nerve canal was DeLano type 2 (34.75%). Vidian canal (VC) and Foramen rotundum (FR) were found dehiscent in 40.5% and 6.38% respectively. Average distance of FR from midline on right and left side was 16.3 ± 2.19 mm and 16.7 ± 2.23 mm respectively. Average distance of VC from midline on right and left side was 12.4 ± 5.84 mm and 12.4 ± 4.18 mm respectively. Average right FR to VC distance was 4.17 ± 2.16 mm and left FR to VC was 4.44 ± 2.20 mm. Anatomical variations of the sphenoid sinus are well known. In the present study, we have tried to highlight the importance of knowledge of various anatomical variations in relations to sphenoid sinus as they are critical in planning of surgery. Pre-operative radiological study and correlation is inevitable to assess type and extent of sinus pneumatisation, bony dehiscence and septal terminations to avoid injury to vital structures.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
Among paranasal sinuses, sphenoid sinus is the least accessible as is deeply situated in the skull. Its close relation to various important neurovascular structures like optic nerve, internal carotid artery, cavernous sinus, vidian nerve and maxillary nerve, renders this sinus a vital role. Due to its central location in the cranial base, it is an important structure in various ventral skull base surgeries. Anatomical variations in the sinus and related structures have been documented and radiological and surgical correlation of these variations is essential to prevent iatrogenic complications. In this study, we retrospectively studied anatomical variations of the sphenoid sinus and related neurovascular structures based on CT scan studies.
Methods
This cross-sectional retrospective study was done on Computed Tomography (CT) scans of Paranasal sinus which have been done from February 2018 to August 2019 at our institute. The ethical clearance for the study was taken from the institutional ethics committee. No patient was made to undergo CT scan for this study. All the CT scan which were earlier done were archived and were evaluated as per protocol. Exclusion criteria included patient age less than 18 years of age, diseases or fractures involving sphenoid sinus and post-operative cases, improper positioning of the patient. The evaluation and measurements of the CT sections were done under constant supervision of an experienced radiologist.
Following parameters were studied.
-
1.
Pneumatization of sphenoid sinus (SS): Classification by Hammer and Radberg was followed in this study [1]. In sagittal view, an imaginary vertical line was drawn through the tuberculum sellae and SS pneumatization was classified as 3 types (Fig. 1):
Fig. 1 
Sphenoid sinus pneumatisation patterns. a Conchal, b Presellar and c Sellar
-
(A)
Conchal—absent pneumatization
-
(B)
Presellar— pneumatization remains anterior to this line
-
(C)
Sellar—pneumatization extends beyond this line
-
2.
Inter sinus septum (ISS): presence or absence of single or multiple ISS and their termination at the optic canals (OC) or carotid canals (CC). This was studied in both axial and coronal views (Fig. 2).
Fig. 2 
Sphenoid sinus septum patterns. a Midline septum, b multiple septum c & d—Sphenoid septum attachment to optic nerve, E& F—Sphenoid septum attachment to carotid canal
-
3.
The relation of Optic nerve with Sphenoid Sinus: DeLano’s classification was followed in our study (Fig. 3) [2].
Fig. 3 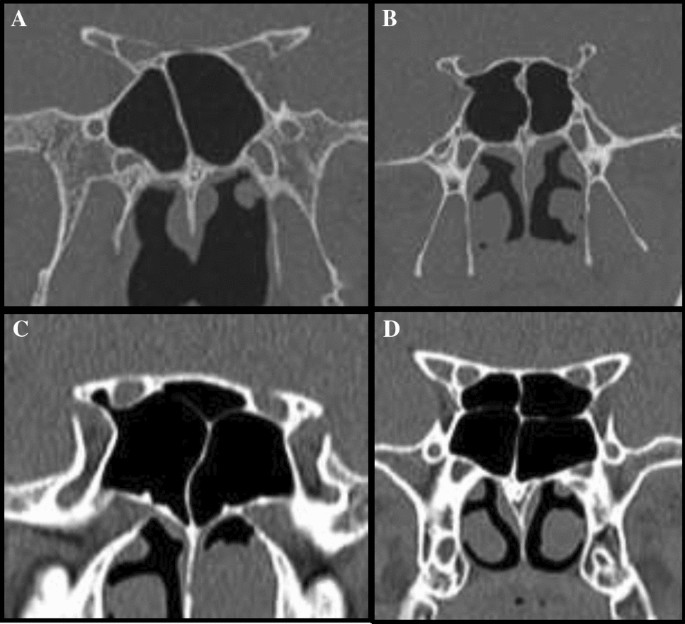
Optic nerve relation with sphenoid sinus—DeLano’s classification a DeLano type I—Optic nerve lying adjacent to lateral or superior wall of sphenoid sinus without impression on sinus wall, b DeLano type II—Optic nerve causing impression on lateral sphenoid sinus wall, c DeLano type III—optic nerve courses through the sphenoid sinus, d DeLano type IV—Optic nerve courses immediately lateral to posterior ethmoids and sphenoid sinuses
-
4.
Carotid canal Protrusion: Presence of more than 50% of the diameter of the Carotid Canal into the Sphenoid sinus was considered as a protrusion (Fig. 4).
Fig. 4 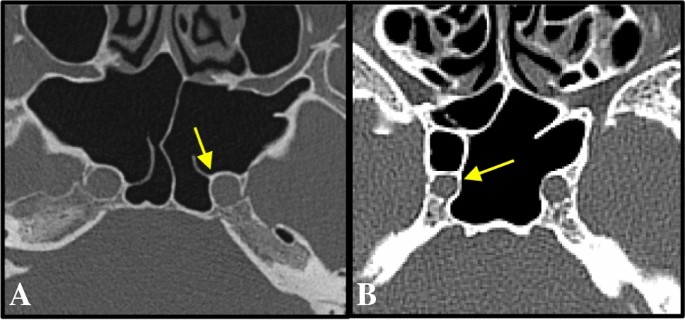
Protrusion of a Left and b Right carotid canal into sphenoid sinus
-
5.
Vidian canal (VC) dehiscence: Absence of visible bone density separating the sinus from the course of VC. Whenever a clear decision between a very thin bony wall and total dehiscence was not feasible, the results were accepted as dehiscence (Fig. 5).
Fig. 5 
a Vidian Canal Dehiscence and b Foramen rotundum dehiscence
-
6.
Maxillary Nerve (MN) dehiscence: Absence of visible bone density separating the sinus from the course of MN. Whenever a clear decision between a very thin bony wall and total dehiscence was not feasible, the results were accepted as dehiscence (Fig. 5).
-
7.
Several morphometric measurements were done in this study. An imaginary line was drawn in the midline, vertical to the rostrum (R) of sphenoid and linear distance was calculated from this line to VC and FR. Distance between FR and VC was also calculated. The distances were calculated on both left and right sides in millimetres (mm) (Fig. 6).
Fig. 6 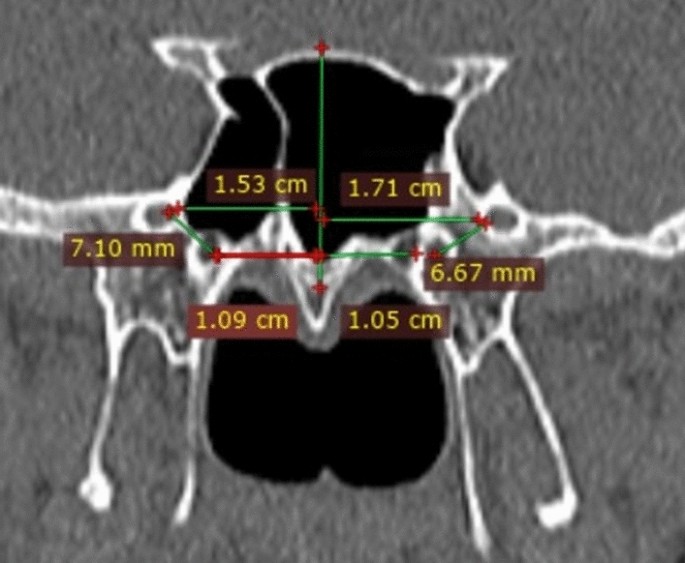
Measurement of Distance of FR and VC from midline






Results
Total 400 CT scans were studied in this study. The age range was found to be from 18 to 74 years and mean age was 35.15 years. 60.5% (242/400) cases were males. Among the types of pneumatisation of Sphenoid sinus, the most common type was Sellar type, found in 89.5% (358/400) cases. Out of 358, 215 were males and 143 were females. Next common type was Presellar in 10% (40/400) cases out of which 26 were males and 14 were females, followed by Conchal type in 0.5% i.e. 2 cases (01 male and 01 female). The Inter Sinus septum was single in 68% cases, whereas, in 32% i.e. 128 cases, ISS was multiple. In 167 (41.75%) cases, ISS was in the midline and in line with rostrum, but in 233 (58.25%) cases, it was attached to other structures. The most common attachment was to the optic nerve in 27% cases and in 22% cases attachment was to Carotid canal. Out of 400 cases, the most common configuration of the relation of optic nerve canal with sphenoid sinus was of DeLano type 2 (34.75%). The next most common relation was of DeLano type 1 in 33.25% cases, followed by type 4 in 16.75% cases and type 3 in 15.25% cases. Carotid canal protrusion was noted in 12.88% cases. Vidian canal (VC) was found dehiscent in 40.5% cases and dehiscence of Maxillary Nerve (MN) was noted in 6.38% cases. Average distance of FR from the midline on the right and left side was 16.3 ± 2.19 mm and 16.7 ± 2.23 mm respectively. Average distance of VC from the midline on the right and left side was 12.4 ± 5.84 mm and 12.4 ± 4.18 mm respectively. Average right FR to VC distance was 4.17 ± 2.16 mm and average left FR to VC distance was 4.44 ± 2.20 mm (Table 1).
Discussion
Anatomical relationships of various neurovascular structures are altered based on the degree of pneumatization of the sphenoid sinus. Previous study on SS pneumatization by Vaezi et al. has shown that more the extent of SS pneumatization, more the surgical access increases as does the distance between maxillary nerve and the vidian nerve [3]. Hammer and Radberg, in their study classified SS pneumatization in 3 types, sellar type being the commonest [1]. Incidence was reported to be 86%. Sellar type of SS pneumatization has been reported to be the most common in studies done in Asians, Malaysians and Croatians. These include studies by Vaezi et al. (73.8%), Tan et al. (55%), and Daniele et al. (77.3%), whereas Madiha et al. noted dominance of Presellar pneumatization in their study in Egyptian population [3,4,5,]–[6]. In present study, majority i.e. 89.5% cases had Sellar type of pneumatization. Sellar type has been reported to be technically less prone to surgical risk when compared to Presellar type.
Pattern of inter sinus septum is also highly variable, not reliable as a landmark to midline. In our study, in 41.75% cases it was present in the midline. This was in accordance with study by Lee et al., who reported 32% incidence of midline septum and Cho et al. who reported 30.5% incidence [7, 8]. However, in the present study, 58.25% cases showed a deviation of ISS from midline and its termination at other structure.
In our study, ISS terminating at ON was the commonest variation reported in 27% cases. The next common attachment of the septum was to CC in 22% cases. The findings in our study are similar to other studies. Cho et al. reported 20% incidence of ISS terminating at ON and 16% at CC [8]. Unal et al. reported 18% cases with septum ending at ON [9]. Cappabianca et al. showed ISS terminating at CC in 20% [10]. Such variations warn to be cautious while removal of the terminal septum as this variation can cause vision loss and life-threatening bleeding during surgery.
Variations involving the optic nerve are clinically very significant. DeLano et al. described the variations in relation of ON with SS into four types, and the most common configuration reported was type 1, reported in 76% cases [2]. Of the four types, type 3 and 4 have close relation of ON with SS and thus more critical for the risk of iatrogenic injury. Heskova et al. and Itagi et al. also reported type 1 as the most common relation, found in 61% and 60% respectively [11] [12]. In the present study, 34.75% cases showed DeLano type 2 relation and 33.25% cases showed DeLano type I relation.
Incidence of CC protrusion in the present study was 12.88%, which is slightly less when compared to other studies. Hewaidi et al. reported 41% protrusion, Tan et al. reported 67% protrusion and Nitinavakarn et al. found 10.2% CC protrusion [4, 13, 14]. Variability in anatomical relation of internal carotid artery with sphenoid sinus predisposes it to inadvertent injury during surgery leading to even life-threatening haemorrhage and their prevention solely lies in reading the scan thoroughly before operating.
Vidian canal dehiscence was noted in 40.5% cases in the present study. Dehiscence was reported in 37% cases by Hewaidi et al., in 37.5% cases by davoodi et al. and in 06% cases by Priyadarshini et al. [13, 15, 16]. Bony dehiscence may attribute to vidian neuralgia in cases of sinus infections or trans sphenoidal surgery and vidian neurectomy [17].
Maxillary nerve in foramen rotundum is another critical structure in relation with sphenoid sinus. It is an important surgical reference forming anatomical limit in approach to superior orbital fissure, cavernous sinus, and middle cranial fossa3. In the present study, FR was found deficient in 6.38% cases. Hewaidi et al. studied FR dehiscence in Libyans and reported 13% incidence [13]. Davoodi et al. reported 36.5% dehiscence in their study, whereas Priyadarshini et al. found dehiscent FR in 20% cases [15, 16]. In the presence of dehiscent FR, maxillary nerve is exposed and is prone to injury during surgery. Bony dehiscence also increases the susceptibility of nerve for neuritis in cases of sinusitis, leading to Trigeminal neuralgia [17].
In our study, parameters such as DeLano type I, maxillary nerve dehiscence, vidian canal dehiscence, distances between foramen rotundum and vidian canal show quite variability. A part of this can be explained by racial and genetic differences in population. Altitude has also been implicated as a factor affecting various anthropometric measurements. Asirdizer M et al. studied the possible effects of altitude and climate on the development of frontal sinus in adults and concluded that widths, antero-posterior lengths and volumes of frontal sinus were higher in a population living in colder climate and higher altitude [18]. Guglielmino-Matessi et al. also stated that climate could be a contributing factor affecting skull and anthropometric measurements [19]. These variations in the data can be partially explained by the fact that our institute caters to a heterogenous population of Himalayan and sub-Himalayan areas.
Also contributing to our results is the fact that whenever the presence of dehiscence was doubtful, we took it as dehiscence (mentioned in the methodology) consciously erring towards the higher side. All scans are evaluated with the help of a radiologist to minimise the chances of wrongful interpretation of the landmarks and measurements.
Various morphometric measurements which were done in the present study showed no age or gender related significance. There was no significant difference in the distances on the right and left side. Comparative studies have been tabulated [20,21,22,]–[23] (Table 2).
Conclusion
Anatomical variations of the sphenoid sinus are well known. In the present study, we have tried to highlight the importance of knowledge of various anatomical variations in relations to sphenoid sinus as they are critical in planning of surgery. Pre-operative radiological study and correlation is inevitable to assess type and extent of sinus pneumatisation, bony dehiscence and septal terminations to avoid injury to vital structures.
References
Hammer G, Rådberg C (1961) The sphenoidal sinus: an anatomical and roentgenologic study with reference to transsphenoid hypophysectomy. Acta radiol 56(6):401–422
DeLano MC, Fun FY, Zinreich SJ (1996) Relationship of the optic nerve to the posterior paranasal sinuses: a CT anatomic study. Am J Neuroradiol 17(4):669–675
Vaezi A, Cardenas E, Pinheiro-Neto C, Paluzzi A, Branstetter BF, Gardner PA et al (2015) Classification of sphenoid sinus pneumatization: relevance for endoscopic skull base surgery. Laryngoscope 125(3):577–581
Tan HKK, Ong YK (2007) Sphenoid sinus: an anatomic and endoscopic study in Asian cadavers. Clin Anat 20(7):745–750
Daniels DL, Mark LP, Ulmer JL, Mafee MF, McDaniel J, Shah NC et al (1998) Osseous anatomy of the pterygopalatine fossa. Am J Neuroradiol 19(8):1423–1432
Madiha AESRA (2007) Endoscopic anantomy of sphenoidal air sinus. Bull Alex Fac Med 43:1021–1026
Lee SK, Park YS, Cho JH, Park YJ, Kang JM, Jeon EJ et al (2004) Anatomic variations of sphenoid sinus and related neurovascular structures: a Study of CT Analysis. Korean J Otorhinolaryngol-Head Neck Surg 47(10):978–982
Cho JH, Kim JK, Lee JG, Yoon JH (2010) Sphenoid sinus pneumatization and its relation to bulging of surrounding neurovascular structures. Ann Otol Rhinol Laryngol 119(9):646–650
Unal B, Bademci G, Bilgili YK, Batay F, Avci E (2006) Risky anatomic variations of sphenoid sinus for surgery. Surg Radiol Anat 28(2):195–201
Cappabianca P, Cavallo LM, Esposito F, de Divitiis O, Messina A, de Divitiis E (2008) Extended endoscopic endonasal approach to the midline skull base : the evolving role of transsphenoidal surgery. Adv Tech Stand Neurosurg 33:151–199
Heskova G, Mellova Y, Holomanova A, Vybohova D, Kunertova L, Marcekova M et al (2009) Assessment of the relation of the optic nerve to the posterior ethmoid and sphenoid sinuses by computed tomography. Biomed Pap 153(2):149–152
Itagi RM, Adiga CP, Kalenahalli K, Goolahally L, Gyanchandani M (2017) Optic nerve canal relation to posterior paranasal sinuses in indian ethnics: review and objective classification. J Clin Diagnostic Res 11(4):01–3
Hewaidi G, Omami G (2008) Anatomic variation of sphenoid sinus and related structures in libyan population: CT scan study. Libyan J Med 3(3):128–133
Nitinavakarn B, Thanaviratananich S, Sangsilp N (2005) Anatomical variations of the lateral nasal wall and paranasal sinuses: a CT study for endoscopic sinus surgery (ESS) in Thai patients. J Med Assoc Thai 88(6):763–768
Davoodi M, Saki N, Saki G, Rahim F (2009) Anatomical variations of neurovascular structures adjacent sphenoid sinus by using CT scan. Pak J Biol Sci PJBS 12(6):522–525
Priyadarshini D, Prabhu LV, Kumar A, Pai MM, Dananjay KVN (2015) The anatomical variations in the neurovascular relations of the sphenoid sinus: an evaluation by coronal computed tomography. Turk Neurosurg 25(2):289–293
Chong VF, Fan YF, Lau DP, Chee LW, Nguyen TM, Sethi DS (2000) Imaging the sphenoid sinus: pictorial essay. Australas Radiol 44(2):143–154
Asirdizer M, Tatlisumak E, Bora A, Tarhan S, Yilmaz Ovali G, Hekimoglu Y et al (2017) The possible effects of altitude and climate on the development of the frontal sinus in adults. Int J Morphol 35(2):571–577
Guglielmino-Matessi CR, Gluckman P, Cavalli-Sforza LL (1979) Climate and the evolution of skull metrics in man. Am J Phys Anthropol 50(4):549–564
Mohebbi A, Rajaeih S, Safdarian M, Omidian P (2017) Seio esfenoidal, forame redondo e canal pterigoideo: estudo radiológico das relações anatômicas. Braz J Otorhinolaryngol 83(4):381–387
Awadalla AM, Hussein Y, Elkammash TH (2015) Anatomical and radiological parameters of the sphenoid sinus among egyptians and its impact on sellar region surgery diagnostic radiology, faculty of medicine. Suez Canal Univ Egypt J Neurosurg 30(1):1–12
Kasemsiri P, Solares CA, Carrau RL, Prosser JD, Prevedello DM, Otto BA et al (2013) Endoscopic endonasal transpterygoid approaches: anatomical landmarks for planning the surgical corridor. Laryngoscope 123(4):811–815
Yazar F, Cankal F, Haholu A, Kiliç C, Tekdemir I (2007) CT evaluation of the vidian canal localization. Clin Anat 20(7):751–754
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Thakur, P., Potluri, P., Kumar, A. et al. Sphenoid Sinus and Related Neurovascular Structures—Anatomical Relations and Variations on Radiology—A Retrospective Study. Indian J Otolaryngol Head Neck Surg 73, 431–436 (2021). https://doi.org/10.1007/s12070-020-01966-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-020-01966-y