
Abstract
There are various surgical techniques for cochlear implantation, classical one being mastoidectomy and posterior tympanotomy which has some disadvantages and complications like extensive bone work, violation of mastoid air cell system and fear of injury to vital structures like facial nerve. To minimize these problems, various modifications in cochlear implantation surgery has been done which includes introduction of Veria technique which also has certain disadvantages like extensive dissection and prolonged surgical time. In this article we are introducing an innovative technique of cochlear implantation where we have modified the pre-existing Veria technique that has been described in detail in the coming sections. Total 9 cases have been done so far with this modified Veria technique. This technique includes postaural approach with minimal soft tissue and bone work, making the cochlear implantation simple, easily doable, with less operating time, with minimal morbidity, faster healing due to smaller incision and avoiding facial nerve injury.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
The most common sensory deficit in children is the hearing loss with its incidence being 1–3 in 1000 live birth per year. Among these children, half of them will have severe to profound hearing loss [1]. The advent of cochlear implant for the people with severe to profound sensorineural hearing loss has become a boon as usage of traditional hearing aids were seen ineffective [2]. A cochlear implant is an electronic prosthetic device that converts the mechanical sounds to electrical impulses and stimulates the neural tissue. It has greatly improved the educational and professional prospects of profoundly deaf children [3]. There are various surgical techniques for cochlear implantation, classical one being mastoidectomy and posterior tympanotomy which was introduced in 1979 [4]. To minimize various disadvantages and surgical complications that are involved in standard procedure, various modifications in cochlear implantation surgery has been taken which includes introduction of veria technique [5]. A suprameatal approach for cochlear implantation was started by Kronenber et al. in 2000, where electrodes were inserted without mastoidectomy and posterior tympanotomy [4]. Veria technique has also seen various modifications. In the present modification of veria technique of cochlear implantation, we use a post-aural incision instead of classical endaural incision. Thus, making the cochlear implantation simple, easily doable, with less operating time, with minimal morbidity, faster healing due to smaller incision and avoiding facial nerve injury.
Methods
This is a prospective, interventional study which was conducted at SMS Medical College and Hospital, Jaipur. It included 9 cochlear implant patients who were implanted by this modification of classical Veria technique between January 2018 to June 2019 and were followed up for 6 months (Table 1). All patients were in age group of 3–5 years except one who was a 2-year-old female child (Table 2). All patients were prelingually deaf and underwent all routine investigations required for procedure under general anaesthesia. All required investigations for candidacy including Brain stem evoked response audiometry (BERA), Oto-acoustic emission (OAE), Tympanometry, High resolution computerised tomographic scan (HRCT) and Magnetic resonance imaging (MRI) were done for all patients. All patients were operated under general anaesthesia by the described modified Veria technique and intraoperative neural response telemetry was done.
The surgical technique is as follows:
-
a.
A postauricular ‘J’ shaped incision (Fig. 1) is made and an optimally thick (3–4 mm) posterior-inferiorly based skin flap is raised. It should neither be too thin to get necrosed nor be too thick to disturb in processor and receiver/stimulator interface.
Fig. 1 
Postaural ‘J’ shaped incision (Right ear)
-
b.
Then a superiorly based musculoperiosteal flap is raised (Fig. 2).
Fig. 2 
Superiorly based musculoperiosteal flap (Right ear)
-
c.
The Spine of Henle is identified and the posterior tympanomeatal flap is elevated from 12 to 6 ‘o’ clock position without intrameatal incision. The round window niche, promontory, chorda tympani and incudostapedial joint exposure is well established.
-
d.
Posterior canalplasty is done in lateral aspect of canal to make canal smooth and look like a funnel, then a small suprameatal shallow well is created behind the posterior wall of canal to keep the excess electrode in place. This suprameatal well is created keeping in mind the level of dura at tegmen mastoid and forward lying sigmoid sinus and is shaped like a pitcher.
-
e.
A superficial tunnel is drilled posterior and parallel to the posterior canal wall with entry point being just at the postero-superior point in external auditory canal and parallel to long process of incus with exit above the chordae tympani and directed towards the round window with help of Veria perforator (Fig. 3).
Fig. 3 
Making the tunnel with veria perforator (Right ear)
-
f.
Implant bed is drilled in parietal bone to accommodate the footprint of receiver/stimulator of cochlear implant and it is connected to the suprameatal well by drilling a narrow channel and keeping a support at exit point by a ledge in bony canal (cantilever bridge) (Fig. 4).
Fig. 4 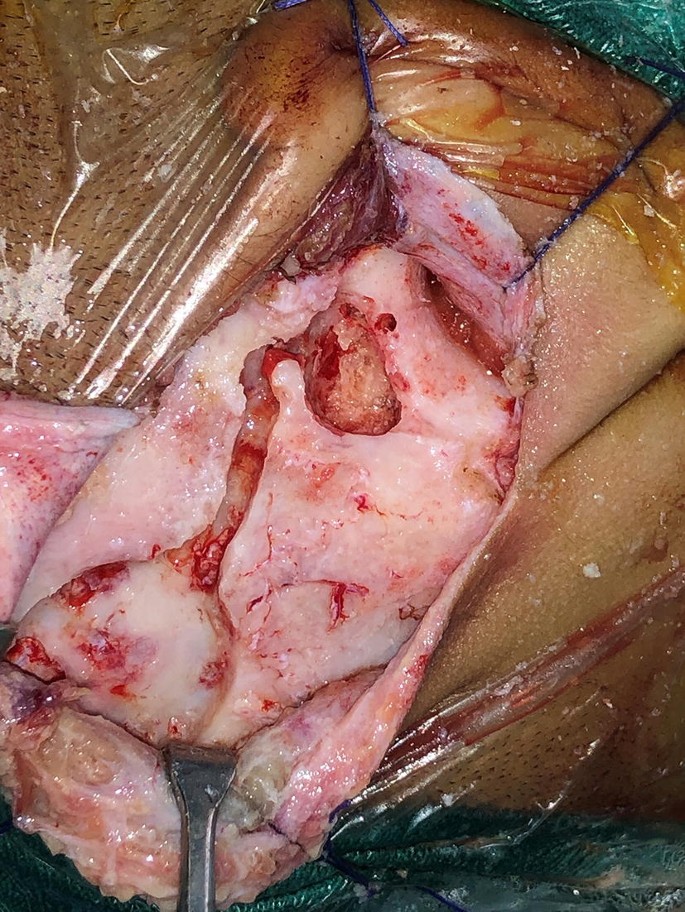
Well/Bed for cochlear implant (Right ear)
-
g.
The overhanging niche of round window is then drilled until the round window membrane is exposed through transcanal approach.
-
h.
After fixing the implant in receiver/stimulator well, the electrode is passed from the tunnel into the middle ear, in front of round window membrane. The electrode tip is positioned, round window membrane is punctured and the electrode is inserted into the cochlea with round window approach along with topical dexamethasone instillation (Fig. 5).
Fig. 5 
Electrodes in tunnel and extended round window cochleostomy (Right ear)
-
i.
Testing of the implant is done with either NRI (Neural Response Imaging), NRT (Neural Response Telemetry), or ART (Auditory Response Telemetry) and stapedial reflex.
-
j.
The electrode is fixed with soft tissues (muscle or fascia) at round window and in the tunnel. The tympanomeatal flap is replaced and the meatus is packed with gelfoam soaked in antibiotic drops.
-
k.
The wound is closed in two layers and mastoid dressing is done.
-
l.
Suture is removed after 7 days of surgery.
-
m.
The implant is switched-on at 21 days.





Results
The incision was given in the postauricular region in all cases. All the cases underwent round window or extended round window cochleostomy. All the landmarks such as round window membrane, promontory, incudostapedial joint and chordate tympani were clearly exposed. There was no difficulty in electrode insertion; all patients had complete insertion of electrode. Post-operative plain x ray (modified stenver’s view) was done in all cases to see the placement and integrity of electrodes. The total operative time taken for surgery ranged between 60 and 75 min with an average of 62.6 min. There were no major complications, intra-operative bleeding was seen in 3 cases from the mastoid emissary vein during elevation of superiorly based musculoperiosteal flap which was stopped with cautery and bone wax/bone dust. No injury to facial or chorda tympani nerve seen. No post-operative complications were seen. The implant was switched-on at 21 days. All 8 patients were followed up for 6 months. There was no significant difference in the outcome in terms of hearing and language development.
Discussion
Cochlear implants are the electronic devices which stimulate inner ear and act as functional replacement of the inner ear. The most common indication of cochlear implantation is bilateral severe to profound sensorineural hearing loss. The standard surgical procedure for cochlear implantation being transmastoid procedure with posterior tympanotomy [6]. The standard procedure consumes more operating time in majority of cases because of drilling of large cavity and need to locate the structures which can possibly get damaged while drilling [7].There are a number of complications related to this procedure such as facial nerve injury, injury to chorda tympani nerve, injury to various structures while drilling like sigmoid sinus, dura and ossicular chain [5].The pneumatisation of mastoid bone is important in cochlear implantation. It is found that drilling becomes difficult in sclerotic mastoid compared to good porous mastoid [8]. The position of cochlea also varies in few cases, in relation to facial nerve and oval window. In some cases, cochlea can be behind the facial canal where cochlea will be rotated posterior-superiorly with flat promontory which makes cochlear implantation difficult through classical approach [8]. Many surgical modifications have been proposed previously to reduce the complications and overcome the majority of the drawbacks seen in cochlear implantation with mastoidectomy and posterior tympanotomy approach. In the year 2000, Kronenben et al. proposed a suprameatal approach for cochlear implantation, where cochlear implantation was done without mastoidectomy and posterior tympanotomy [4]. Later, Prof.Trifon Kiratzidis designed an alternative approach to classical technique for cochlear implantation and named it after the Veria city [9]. It is a non-mastoidectomy procedure where endaural route is used for transcanal cochleostomy. Electrodes of the cochlear implant are passed through the tunnel which is drilled parallel to posterior canal wall through facial recess which opens into middle ear. It has an advantage of giving access to cochlea without endangering the facial nerve and also maintaining natural mastoid air cell systems [8]. The tunnel is drilled with a specially designed device known as Veria perforator. It consists of straight hand-piece on which a special ring with a guided rod is attached and it uses a 1.4 mm carbide burr to make the tunnel. While drilling, the axis of the cutting burr should always be parallel to the surface of the bone. In our modification in Veria technique, a post-auricular ‘J’ shaped incision is made instead of endaural incision, a superiorly bases musculoperiosteal flap is elevated, a tunnel is drilled in the posterior canal wall to reach to the middle ear cavity and mastoidectomy is avoided. This modification is used to consume less operating time with faster healing, less co-morbidities and preventing major complications that can occur in standard surgery such as injury to facial nerve and other important structures. Overall, the major advantage of this technique is versatility of the technique to handle all possible type of cochlear rotations, cochlear malformations, non-pneumatised temporal bone and jugular bulb variations with ease due to transcanal direct approach to the cochlea. Electrode is well covered with thin shell of bone which is no less than 0.6 mm and none of the cases had electrode extrusion. In a recent article, Marco Caversaccio et al. [10] have demonstrated the feasibility of robotic middle ear key hole access through the same route which our modified Veria technique uses.
Conclusion
Modified veria technique is a simple procedure for cochlear implantation which is safe and has easy and fast learning curve for operating surgeons as it consumes less operating time and avoids major complications that can occur during surgery. It can be used with all types of cochlear implants and even in the presence of cochlear malformations.
References
Copeland BJ, Pillsbury HC (2004) Cochlear implantation for the treatment of deafness. Annu Rev Med 55:157–167
Owens D, Espeso A, Hayes J, Williams RG (2006) Cochlear implants: referral, selection and rehabilitation. Curr Paediatr 16(5):360–365
Nadol JB Jr (1997) Patterns of neural degeneration in the human cochlear and auditory nerve: implications for cochlear implantation. Otolaryngeal Head Neck Surg 117(3):220–228
Jappel A et al (2004) Histological evaluation of suprameatal approach (SMA) in cochlear implant surgery. Int Congress Series 1273:115–117
Mostafa BE, Ezzat WF, El Mogui AM (2014) The modified transcanal approach for cochlear implantation: technique and results. Advan Otolaryngol 509703:1–5
Lenarz T (2017) Cochlear implant state of art. GMS Curr Top Otorhinolaryngol Head Neck Surg 16:1865–1011
Brett B et al (2012) A self-developedand constructed robot for minimally invasive cochlear implantation. Acta Otolaryngol 132:355–360
Jain R et al (2019) A clinico-radiological study: veria technique of cochlear implant—a study of 50 cases. Ind J Otolaryngol Head Neck Surg 71(2):1553–1561
Kiratzidis T, Arnold W, Iliades T (2002) Veria operationupdated. I. The trans-canal wall cochlear implantation. ORL J Otorhinolaryngol Relat Spec 64:406–412
Caversaccio M et al (2019) Robotic middle ear access for cochlear implantation: first in man. PLoS ONE. https://doi.org/10.1371/journal.pone.0220543
Funding
This research was not funded by any authority.
Author information
Authors and Affiliations
Contributions
All authors contributed in conceptualization of this novel technique, in the preparation and final disposition of this manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There has been no financial support and no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Singhal, P., Nagaraj, S., Verma, N. et al. Modified Veria Technique for Cochlear Implantation by Postaural Approach. Indian J Otolaryngol Head Neck Surg 72, 370–374 (2020). https://doi.org/10.1007/s12070-020-01895-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-020-01895-w