
Abstract
Chromosome abnormality is one of the important causes of spontaneous abortion. However, due to regional and ethnic differences, the reported rates of chromosomal abnormalities in patients with spontaneous abortion vary greatly. At present, there is no large sample statistics of chromosome abnormality in patients with spontaneous abortion in Yantai, Shandong province, China and hence 2959 couples (5918 individuals) with spontaneous abortion were recruited for this study. G banding was used to examine the karyotype of patients. The results showed that chromosomal abnormalities were present in 173 of 2959 couples with the rate of 5.85%. Female carriers were significantly higher than male. Chromosomal abnormality rate was positively correlated with the number of spontaneous abortions. Structural aberrations were significantly greater than numerical aberrations, with a prevalence of 92.49% and 7.51%, respectively. Balanced translocation, Robertson translocation and inversion were the most common types of chromosomal structural abnormalities. Among them, the proportion of balanced translocation was the highest (63.13%, 101/160). In addition, three cases of rare complex abnormal karyotype were detected. In summary, chromosome abnormality could be one of the important causes of spontaneous abortion in Yantai, Shandong province, China. The sex of patients with chromosomal abnormalities and the number of spontaneous abortions should be considered in genetic counselling. When one of the partners have chromosome abnormality, preimplantation genetic diagnosis and prenatal diagnosis could play a great significance for preventing the birth of children with chromosomal diseases and reducing birth defects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Abortion that occurs in a natural state (not for human purposes) is called spontaneous abortion. Spontaneous abortion occurs in ~15–20% of all clinically recognizable pregnancies (Rai and Regan 2006; Stephenson and Kutteh 2007). Spontaneous abortion is divided into early abortion (<12 weeks) and late abortion (12–28 w). In almost 50% of the cases, the aetiology is unknown. The common causes of abortion include: chromosomal abnormalities, maternal endocrine disorders (e.g., luteal insufficiency, polycystic ovary syndrome, hyperprolactinaemia, thyroid and diabetes), abnormalities of maternal reproductive tract (e.g., uterine deformity, Asherman syndrome, cervical insufficiency, uterine fibroids and genital tract infection), and an unhealthy lifestyle (e.g., smoking, alcohol abuse, excessive consumption of caffeine and environmental factors such as organic solvents and toxins).
Chromosome abnormality is one of the important causes of spontaneous abortion. Research shows that in the foetuses of spontaneous abortion, chromosomal abnormality is found to be 50–70% (Carp et al. 2004), among which triploidy is 18%. Triploid foetuses are prone to abortion because of the formation of tertiary spindles in the process of embryo development during mitosis, resulting in the distribution disorder of chromosomes in the middle and late stage of cell division, which seriously interferes with the normal development of embryos and leads to abortion. The frequency of chromosomal abnormalities among couples with spontaneous abortion varies from 2 to 10% (Dutta et al. 2011; Ayed et al. 2017; Yildirim et al. 2019; Pal et al. 2018; Fan et al. 2016), much higher than the 0.5% of the normal population (Fryns et al. 1984; Yang et al. 2014). The presence of chromosomal rearrangements can result in abnormal distribution of chromosomes during meiosis, which leads to the imbalance of gamete chromosomes. Gamete chromosomes imbalance will seriously affect the normal development of embryos, resulting in spontaneous abortion.
Chromosomal karyotype analysis has become one of the important methods to find the cause of abortion. However, due to regional and ethnic differences, the reported rates of chromosomal abnormalities in patients with spontaneous abortion vary greatly. At present, there is no large sample statistics of chromosome abnormality in patients with spontaneous abortion in Yantai. For this purpose, we collected 2959 couples with a history of spontaneous abortion in Yantai, tested their peripheral blood chromosomes, and conducted statistical analysis on the incidence and distribution of abnormal chromosomes. Our study will further clarify the role of chromosomal abnormalities in spontaneous abortion and provide references for genetic counselling of patients with spontaneous abortion. In addition, three rare complex karyotypes are described in detail.
Materials and methods
Patients
A total of 2959 couples (5918 individuals) with spontaneous abortion in the Yantai Yu Huang Ding Hospital from 1 January 2013 to 31 December 2018 were recruited. The age group of the subjects ranged from 22 years to 49 years. The clinical data of confirmed cases were retrospectively collected and analysed. Miscarriages due to immune effects, uterine abnormalities and other causes were excluded. The study was approved by the Ethical Committee of Yantai Yu Huang Ding Hospital. Informed consent was obtained from all participants.
G banding
Heparin anticoagulant blood, 0.8 mL was added to 5 mL lymphocyte culture medium and cultured in 37°C. After 68–72 h of incubation, colchicine (1 mg/mL) was added and incubated for another 2 h. Then the cells were treated with hypotonic solution of 0.075 M KCl at 37°C for 35 min, and fixed thrice using fixation liquid (methanol and acetic acid in a ratio of 3:1). Karyotype analysis was performed on G-banded metaphase chromosomes using a standard protocol that generated 400–450 band resolutions. Thirty metaphases per patient were counted, and a minimum of five metaphases were analysed. For mosaicism, at least 100 metaphases were counted. Chromosome polymorphisms, such as pericentric inversion 9 variant, centromeric heterochromatin variants and satellite variants were described in detail and classified as normal. Karyotype reports were based on the International System for Human Cytogenetic Nomenclature (ISCN 2013).
Statistical analysis
All data were analysed using SPSS v.17.0 for Windows (SPSS, Chicago, USA). Parametric variables were compared using the linear-by-linear association. P < 0.05 was considered to be statistically significant.
Results
A total of 2959 couples (5918 cases) with spontaneous abortion were examined. The median age of male was 31.45 years ± 5.63 and the median age of female was 30.81 ± 5.08. The number of spontaneous abortion varied from one to eight abortions/couple. Among them, the proportion of the patients having two spontaneous abortions was the highest (65.12%), and the patients with more than three spontaneous abortions accounted only 8.69% (table 1).
Chromosomal abnormalities were detected in 173 of 2959 couples with 5.85%. The percentage of female (110/173, 63.58%) carrying chromosomal abnormalities was higher than male (63/173, 36.42%) (table 2). No couple presented an abnormal karyotype in both partners. Chromosomal abnormality rate was positively correlated with the number of spontaneous abortions (P < 0.001).
Hundred and sixty cases showed structural aberrations and 13 cases showed numerical aberrations, with a prevalence of 92.49% and 7.51%, respectively. Balanced translocation, Robertsonian translocation and inversion were the most common types of chromosomal structural abnormalities. Chromosome number abnormality was mainly caused by sex chromosome number abnormality (table 2).
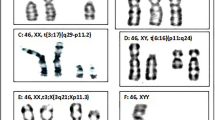
Among 101 cases of balanced reciprocal translocations, 19 showed involvement of chromosome 6; and 18 cases showed association of chromosome 3 (table 3). Three rare complex karyotypes were found, 45,XX,der(11)t(11;13)(q25;p12),-13 (figure 1a), 46,XY,inv(10)(q11.23q23.2), t(10;14)(p11.23;q22) (figure 1b), and 46,XY,inv(4)(q31.1q35),t(8;18)(q13; q12.2) (figure 1c).

Three cases of rare karyotype. The arrows show abnormal chromosomes. (a) 45,XX,der(11)t(11;13)(q25;p12),-13; (b) 46,XY,inv(10)(q11.23q23.2),t(10;14) (p11.23;q22); (c) 46,XY,inv(4)(q31.1q35),t(8;18)(q13;q12.2).
Robertsonian translocation was found in 31 cases. Among them, chromosomes 13 and 14 were involved in 12 cases (38.71%) (table 4). Inversion was found in 23 cases, mainly involving chromosomes 1, Y, 3 and 11 (table 5; figure 2). In addition, nine cases of X chromosome mosaicism, two cases of 47,XXX, one case of 47,XYY and one case of deletion of Xp were detected, four cases of fra(16) were observed, and one marker chromosome was identified (table 6).

Images of various inversions. The arrows show abnormal chromosomes. (a) inv(1)(p13.1q12), (b) inv(1)(p22.1p34.1), (c) inv(1)(p11q21), (d) inv(1)(p22q25), (e) inv(1)(q32.1q32.3), (f) inv(10)(q11.2q23.2), (g) inv(10)(p15q21), (h) inv(Y)(p11.2q11.2), (i) inv(11)(q13q21), (j) inv(11)(p15.4q21), (k) inv(11)(q13.2q23.2), (l) inv(2)(p14p16), (m) inv(2)(p11.1q13), (n) inv(4)(p12q21), (o) inv(3)(p23q11.2), (p) inv(5)(p15q32), (q) inv(12)(q13q15), (r) inv(13)(q14.1q21.2), (s) inv(16)(q22q23.2).
Discussion
In this study, 2959 couples with spontaneous abortion were detected, and the abnormal rate was 5.85%, much higher than the 0.5% of the normal population, which indicated that chromosomal abnormalities were one of the important causes of spontaneous abortion. The percentage of females carrying chromosomal abnormalities was higher than male, which is consistent with previous reports (table 7). However, in Sudhir et al. (2016), of the 12 patients, eight with chromosomal abnormalities were male four were female. There may be two reasons for this situation, one is due to regional differences, and the other reason may be due to insufficient sample.
Among 2959 couples, the number of spontaneous abortion varied from one to eight abortions/couple. Patients with less than two spontaneous abortions was the main part (91.31%, 2707/2595), and more than three spontaneous abortions only accounted for 8.69% (257/2959), indicated that the patients paid more attention to the causes of abortion. At the same time, we found that the chromosome abnormality rate of patients with more than three spontaneous abortions was significantly higher than that of patients with less than two spontaneous abortions and chromosome abnormality rate increase significantly with the number of spontaneous abortions, which is consistent with the reports of Asgari et al. (2013) and Mogib El-Dahtory (2011).
Among 173 cases of chromosomal abnormalities, structural aberrations were the most common chromosomal abnormalities (160/173), and the incidence (2.70%, 160/5918) was significantly higher than that (0.7%) in normal population (Wang et al. 2009). Balanced translocation (58.38%), Robertsonian translocation (17.92%) and inversion (13.29%) were the most common types of chromosomal structural abnormalities. Our results are consistent with previous studies (Dutta et al. 2011; Fan et al. 2016; Ayed et al. 2017).
Balanced translocation means that two chromosomes break at the same time, and the fragments are rejoined to form two derived chromosomes after exchanging positions, without causing an increase or decrease of chromosome fragments. Hundred and one cases of balanced reciprocal translocations were detected. The ratio of female/male carriers was 1.86:1 (65/35). Two proposed mechanism contributing to the higher incidence of female translocation carriers. One is that female translocation carriers release only one mature ovum per month, whereas male carriers release millions of sperm per ejaculation, resulting in possible pre-zygotic selection against unbalanced gametes (Kochhar and Ghosh 2013). Another may be that the abnormal chromosome structure leads to the decline of male spermatogenesis leading to infertility (Harton and Tempest 2012). We found that balanced reciprocal translocations mainly involved chromosomes 6 and 3. In addition, three rare complex karyotypes were found. All patients were in good health and denied a history of exposure to harmful substances and radiation. The first case is a 33-year-old woman with a karyotype of 45,XX,der(11)t(11;13) (q25;p12),-13; the second patient is a 25-year-old male with a karyotype of 46,XY,inv(10)(q11.23q23.2),t(10;14) (p11.23;q22), and the last patient is a 35-year-old male with a karyotype of 46,XY,inv(4)(q31.1q35),t(8;18) (q13;q12.2). None of the three karyotypes has been reported, so they were especially helpful to supplement the karyotype diversity of patients with chromosomal abnormalities.
Robertsonian translocation is a special kind of balanced translocation, involving only the acrocentric chromosomes. When two acrocentric chromosomes break at the centromere, their long arms join to form a derived chromosome. In our study, 31 cases of Robertsonian translocation were found, among them 12 cases were 45,XN,der(13;14)(q10;q10), accounting for 38.71%, which is well consistent with previous research results (Dutta et al. 2011; Sheth et al. 2013; Fan et al. 2016). Thus, our results further confirm that Robertsonian translocation is most likely to occur on chromosomes 13 and 14.
Inversion is a chromosome that has been broken twice, and the segment between the two breakpoints rotates 180° before reconnecting, leading to the rearrangement of the chromosome gene order. In our study, inversion were found in 23 cases, mainly involving chromosomes 1, Y, 3 and 11. Previous studies also described the presence of chromosomes 1, Y, 3 and 11 inversions in patients with spontaneous abortion (Dutta et al. 2011; Tunç et al. 2016). In addition, 12 cases were pericentric inversions, nine cases were paracentric inversion in the long arm of chromosome, and in two cases paracentric inversion was detected in the short arm of chromosome, suggesting that the incidence of paracentric inversion in the short arm of chromosome might be lower than that in the other two forms. It is widely known that the role of pericentric inversion 9 variant in spontaneous abortion is controversial. In this study, 28 cases of pericentric inversion 9 variant were detected, and the incidence rate (0.54%, 28/5918) was much lower than that of normal population (1.00–1.65%) (Teo et al. 1995), suggesting that the pericentric inversion 9 variant is a normal chromosomal variation.
Summary and conclusion
The prevalence of chromosomal abnormalities in couples with spontaneous abortion in Yantai, Shandong province was 5.85%, indicating that the chromosome abnormality could be one of the important causes of spontaneous abortion. The rate of percentage of chromosomal abnormalities in females was significantly higher than that of males. The rate of chromosome abnormality was positively correlated with the number of spontaneous abortions. Hence, gender and the number of spontaneous abortions should also be considered in genetic counselling. When one of the partners has chromosome abnormality, preimplantation genetic diagnosis, amniocentesis, or chorionic villus sampling could play a great significance for reducing birth defects.
References
Ayed W., Messaoudi I., Belghith Z., Hammami W., Chemkhi I., Abidli N. et al. 2017 Chromosomal abnormalities in 163 Tunisian couples with recurrent miscarriages. Pan. Afr. Med. J. 28, 99.
Asgari A., Ghahremani S., Saeedi S. and Kamrani E. 2013 The study of chromosomal abnormalities and heteromorphism in couples with 2 or 3 recurrent abortions in Shahid Beheshti Hospital of Hamedan. Iran J. Reprod. Med. 11, 201.
Carp H., Feldman B., Oelsner G. and Schiff E. 2004 Parental karyotype and subsequent live births in recurrent miscarriage. Fertil. Steril. 81, 1296–1301.
Dutta U. R., Rajitha P., Pidugu V. K. and Dalal A. B. 2011 Cytogenetic abnormalities in 1162 couples with recurrent miscarriages in southern region of India: report and review. J. Assist. Reprod. Genet. 28, 145–149.
Elghezal H., Hidar S., Mougou S., Khairi H. and Saad A. 2007 Prevalence of chromosomal abnormalities in couples with recurrent miscarriage. Fertil. Steril. 88, 721–723.
Fan H. T., Zhang M., Zhan P., Yang X., Tian W. J. and Li R. W. 2016 Structural chromosomal abnormalities in couples in cases of recurrent spontaneous abortions in Jilin province, China. Genet. Mol. Res. 15.
Fryns J. P., Kleczkowska A., Kubein E., Petit P. and Van B. H. 1984 Cytogenetic survey in couples with recurrent fetal wastage. Hum. Genet. 65, 336–354.
Harton G. L. and Tempest H. G. 2012 Chromosomal disorders and male infertility. Asian J. Androl. 14, 32–39.
Kochhar P. K. and Ghosh P. 2013 Reproductive outcome of couples with recurrent miscarriage and balanced chromosomal abnormalities. J. Obstet. Gynaecol. Res. 39, 113–120.
Mogib El-Dahtory F. A. 2011 Chromosomal abnormalities as a cause of recurrent abortions in Egypt. Indian J. Hum. Genet. 17, 82–84.
Pal A. K., Ambulkar P. S., Waghmare J. E., Wankhede V., Shende R. M. and Tarnekar A. M. 2018 Chromosomal aberrations in couples with pregnancy loss: a retrospective study. J. Hum. Reprod. Sci. J. 11, 247–253.
Rai R. and Regan L. 2006 Recurrent miscarriage. Lancet 368, 601–611.
Sheth F. J., Liehr T., Kumari P., Akinde R., Sheth H. J. and Sheth J. J. 2013 Chromosomal abnormalities in couples with repeated fetal loss: an Indian retrospective study. Indian J. Hum. Genet. 19, 415–422.
Stephenson M. and Kutteh W. 2007 Evaluation and management of recurrent early pregnancy loss. Clin. Obstet. Gynecol. J. 50, 132–145.
Sudhir N., Kaur T., Beri A. and Kaur A. 2016 Cytogenetic analysis in couples with recurrent miscarriages: a retrospective study from Punjab, north India. J. Genet. 95, 887–894.
Teo S. H., Tan M., Knight L., Yeo S. H. and Ng I. 1995 Pericentric inversion 9-incidence and clinical significance. Ann. Acad. Med. Singapore 24, 302–304.
Tunç E., Tanrıverdi N., Demirhan O., Süleymanova D. and Çetinel N. 2016 Chrom-osomal analyses of 1510 couples who have experienced recurrent spontaneous abortions. Reprod. Biomed. Online J. 32, 414–419.
Wang Y. W., Han W. T., Guan C. J., Ge W., Zhu X. Q., Jiang M. et al. 2009 Cytogenetic study on couples with a history of reproductive failure in China. J. Reprod. Contracept. 20, 237–246.
Yang Y., Wang H., Gao M., Xu S. S., Xu X. F., Cao X. Y. et al. 2014 Pre-pregnancy cytogenetic analysis of general couples in eastern China. Sci. Rep. J. 4, 7224.
Yildirim M. E., Karakus S., Kurtulgan H. K., Baser B. and Sezgin I. 2019 The type and prevalence of chromosomal abnormalities in couples with recurrent first trimester abortions: a Turkish retrospective study. J. Gynecol. Obstet. Hum. Reprod. 48, 521–525.
Acknowledgement
We thank the patient for their participation in this study.
Author information
Authors and Affiliations
Contributions
Z-YM and X-YL wrote the manuscript and coordinated the clinical analysis of the patients.
Corresponding author
Additional information
Corresponding editor: B. K. Thelma
Zong-Yu Miao and Xiao-Yan Liu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Miao, ZY., Liu, XY., Wu, H. et al. Cytogenetic analysis of 2959 couples with spontaneous abortion and detailed analysis of rare karyotypes. J Genet 101, 10 (2022). https://doi.org/10.1007/s12041-021-01347-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12041-021-01347-6