
Abstract
The understanding of how pain is processed at each stage in the peripheral and central nervous system is the precondition to develop new therapies for the selective treatment of pain. In the periphery, ATP can be released from various cells as a consequence of tissue injury or visceral distension and may stimulate the local nociceptors. The highly selective distribution of P2X3 and P2X2/3 receptors within the nociceptive system has inspired a variety of approaches to elucidate the potential role of ATP as a pain mediator. Depolarization by ATP of neurons in pain–relevant neuronal structures such as trigeminal ganglion, dorsal root ganglion, and spinal cord dorsal horn neurons are well investigated. P2X receptor-mediated afferent activation appears to have been implicated in visceral and neuropathic pain and even in migraine and cancer pain. This article reviews recently published research describing the role that ATP and P2X receptors may play in pain perception, highlighting the importance of the P2X3 receptor in different states of pain.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Two broad categories of pain, acute and chronic, are seen in clinical practice. Acute pain is of short duration, normally has an identifiable cause, and is focal to the side of injury. In contrast, chronic pain with the characteristics of a disease state has no identifiable cause, serves no biological function, and typically has a poor prognosis because of the lack of complex treatment strategies at present.
In recent years, the involvement of a variety of important mediators in pain transmission has been demonstrated. Certain well-investigated and important neurotransmitters, such as glutamate, serotonin, acetylcholine, and various other endogenous agents, such as prostaglandins, histamine, substance P, or bradykinin are involved in the molecular mechanisms of activation and sensitization of nociceptors that trigger pain. Moreover, ATP is a further strong candidate implicated in peripheral pain mediation. Early indication for the initiation of pain by ATP resulted from experiments with human skin blisters by Collier et al. in 1966 [1] and Bleehen and Keele [2] a decade later. Local application of ATP onto human skin induced a persistent sensation of pain associated with vascular changes [3]. Combined application of ATP with other algogenic substances such as capsaicin [4] or additional local ultraviolet irradiation enhanced the sensation of pain [5]. The infusion of ATP into the musculus trapezius evoked pain [6] and tenderness [7]. During the last 15 years, with the development of improved immunohistochemical and molecular biological techniques, a plethora of data approved the involvement of ATP in pain perception.
The potential importance of ATP in nociception results last, but not the least, from its ubiquitous presence at millimolar concentrations in living cells. On the one hand, ATP can be released from various cells as a consequence of tissue injury or visceral distension and may stimulate the local nociceptors [8–12]. Depolarization by ATP of neurons in pain relevant neuronal structures such as trigeminal ganglion (TG), dorsal root ganglion (DRG), and spinal cord dorsal horn neurons are well investigated. Nociceptive sensory neurons selectively express the P2X3 receptor at high levels (Fig. 1), suggesting the outstanding role of this receptor subtype in processing pain. The main purpose of this review was to outline the relevance of homomeric P2X3 and heteromeric P2X2/3 receptors in different pain states (Table 1). Because the involvement of other P2 receptor-types in nociception has recently been postulated, their involvement is also taken into consideration.

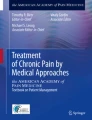
Ascending control of pain and localization of pain relevant P2X receptors in both neuronal and non-neuronal cells along the neuraxis. The receptor expression in dorsal root ganglion (DRG) and trigeminal ganglion (TG) neurons that is depicted in this schematic drawing is representative also for other sensory ganglia (e.g., nodose ganglia) neurons. High concentrations of ATP are released by nociceptive stimuli from the synaptic vesicles of primary afferent neurons or from damaged neuronal or non-neuronal cells in peripheral tissue. Before its rapid degradation to adenosine, ATP may stimulate P2X2/3,3 receptors localized on nociceptive terminals of sensory ganglia neurons. DRG neurons project to the dorsal horn of the spinal cord. On dorsal horn neurons, the P2X1–6 subtypes were detected, but the highest expression levels have been demonstrated for P2X2,4 and P2X6 receptors. Microglia cells of the dorsal horn possess P2X4 and P2X7 receptors. After activation of these receptors, a host of diffusible factors such as cytokines and chemokines are released, which then act at adjacent neurons to promote hypersensitivity responses. P2X3 receptors situated on the terminals of DRG neurons have been shown to positively modulate the release of glutamate and possibly ATP. Dorsal horn astrocytes can release ATP, which is, in turn, able to activate neighboring cells via several types of P2Y receptors. Ado Adenosine, ATP adenosine 5′-triphosphate, DRG dorsal root ganglion, TG trigeminal ganglion
P2 Receptors Implicated in Pain
ATP exerts its effects via P2 receptors, which can be subdivided into two major families, the P2X and P2Y receptors. P2X receptors are ligand-gated ion channels. Seven P2X subunits (P2X1–7) have been identified and cloned so far [13–15].
The topology of a P2X receptor subunit exhibits two transmembrane domains, connected by an extracellular loop containing regulatory N-glycosylation sites [16–18]. The N- and C-termini reside intracellularly [19]. At present, the crystal structure of P2X receptors is unknown; it is thought, however, that the channels are formed by a composition of homomeric or heteromeric trimers of subunits [17]. The biophysical and pharmacological properties of P2X receptors have been reviewed recently in detail [20, 21].
P2Y receptors belong to the superfamily of G protein coupled heptahelical receptors. Eight different mammalian P2Y subtypes are currently distinguished, namely, P2Y1,2,4,6,11,12,13,14 [22]. Negative coupling to Gi/o proteins, and thereby, inhibition of adenylate cyclase was shown for P2Y12,13,14 receptors, whereas positive coupling to Gq/11 proteins followed by activation of phospholipase C was reported for the P2Y1,2,4,6,11 subtypes. The P2Y11 receptor can additionally activate adenylate cyclase via positive coupling to Gi/o. Excellent updates summarizing P2Y receptor pharmacology and intracellular signalling have been published recently [14, 23, 24].
P2X Receptors
In the past, the distribution of P2X receptors in pain relevant neuronal structures was investigated in a number of studies. In sensory ganglia, all seven cloned mammalian P2X receptors are present [11, 25, 26]. Six of them (P2X1–6) were detected with distinct distribution patterns in primary afferent neurons of rats by means of immunohistochemistry and in situ hybridization [27–29, 36]. In contrast to the P2X2 and P2X3 receptors which were expressed in a comparably high magnitude, low mRNA and protein levels of the other subtypes, except for the nodose ganglion, were observed only.
However, in a recent study by Kobayashi and collaborators [30], a different expression pattern of P2X subunit mRNA was detected in rat DRG neurons. In conflict with former studies, the authors did not find P2X1 receptor mRNA either in DRG neurons or in DRG glia cells. Furthermore, the extent of P2X3 receptor expression was more than twice the extent of P2X2 receptor expression. Whereas in rats and mice up to 90% of DRG neurons were P2X3-immunoreactive, in the upper lumbosacral DRG of the cat, only 30% of the neurons expressed P2X3 receptors [31]. While P2X7 receptors could neither functionally nor immunohistochemically be found in small diameter neurons from both human [32] and rat DRG [26], both small and large diameter neurons of cat DRG were positively stained with P2X7 polyclonal antibodies [31]. In addition, the occurrence of this receptor subtype on non-neuronal cells in rat DRG has been repeatedly demonstrated [26, 32]. Because of the well-known problems concerning the specificity of P2X receptor antibodies, further studies will be necessary to clarify the discrepancies between functional and immunohistochemical data.
Nociceptive neurons can be divided into two major populations, non-myelinated C-fiber and myelinated A-fiber neurons [33]. The group of C-fiber neurons is comprised of both peptidergic neurons, which possess a receptor tyrosine kinase (TrkA) for nerve growth factor (NGF) and of non-peptidergic neurons, which lacks TrkA. A subpopulation of non-peptidergic C-fiber neurons expresses the receptor complex for glial cell-derived neurotrophic factor (GDNF). This population of neurons can be labeled by isolectine B4 from Griffonia simplicifolia [34, 35]. The majority of P2X3-positive neurons belongs to the GNDF sensitive population [36, 37] and project to inner lamina II of the dorsal horn of the spinal cord. The GDNF-sensitive population also expresses the transient receptor potential V1 (TRPV1), formerly known as vanilloid receptor 1 (VR1), which can be activated by capsaicin, the pungent agent of hot chili pepper. It is broadly accepted that TRPV1-positive neurons are nociceptive neurons.
The coexpression of TRPV1 and high levels of P2X3 (and P2X2) receptors in sensory neurons supports the involvement of the P2X3 and P2X2/3 receptors in pain [27, 38]. This assumption was confirmed by both in vivo experiments [39] and in vitro electrophysiological studies indicating the activation of primary afferents by ATP via these receptor-types [27, 40, 41, 42]. In capsaicin-sensitive neurons, ATP and its analog α,β-meATP, which selectively stimulates the P2X1,3 subtypes [43], evoke inward currents with fast activation and inactivation kinetics [42] that were lacking in P2X3-deficient mice [44, 45]. Medium-sized DRG neurons with fast activation but slow desensitization kinetics towards ATP and α,β-meATP were not sensitive to capsaicin and expressed mRNAs for P2X2 and P2X3 subunits, suggesting the presence of heteromeric P2X2/3 receptors [42].
An interesting study by Vacca and collaborators [46] provided evidence for the constitutive localization of P2X3 receptors in cholesterol and sphingolipid-rich membrane domains, the so-called lipid rafts, in rat DRG neurons. Lipid rafts are thought to be involved in many functions in neurons, including neurotrophic factor signaling, protein sorting in the trans-Golgi network and vesicular trafficking [47, 48]. Moreover, selective functional cross-talk of the P2X3 receptor with other raft-resident receptors, such as GABAB receptors, could be explained by their coexpression in the same membrane domain [46].
Approximately 40% of rat DRG neurons in culture ([36, 37], but see also [30]) and 37–58% of rat TG neurons [49] show P2X3 immunoreactivity. In DRG, the P2X3 receptor is expressed almost exclusively on small- and medium-diameter neurons. However in TG, P2X3 receptor immunoreactivity was detected also in the somata and processes of large-diameter neurons [29, 41, 50]. In nodose ganglion neurons, even a predominant expression of P2X2 and P2X2/3 receptors with sustained responses to ATP and α,β-meATP has been found [51, 52]. These responses were modulated by both endogenous and synthetic cannabinoids suggesting an interplay between cannabinoid receptors and P2X2 or P2X2/3 receptors in the sensation of pain [53].
In addition to the fact that the expression of P2X2, P2X2/3, and P2X3 receptors depends on the type of sensory neurons (TG, DRG, or nodose ganglion) studied, the duration of culturing may also be important, as a gradual decline of positive P2X3 immunostaining during postnatal development has been reported in DRG [54]. Although nearly all sensory neurons in DRG, TG, and nodose ganglion of mice express P2X3 receptors on embryonic day 14, only about 50% of both the small and medium-sized neurons possess this subtype on postnatal day 14.
Based on the onset and offset kinetics, three types of ATP-induced P2X currents were recorded in DRG neurons from adult rats [55, 56]. Fast currents were predominantly observed in small IB4-positive DRG neurons and were found to be mediated by homomeric P2X3 receptors. Both slow P2X2 and mixed P2X2/3 receptor-mediated currents occurred in small and medium-sized DRG neurons that were mostly IB4-positive. In P2X3 receptor deficient mice, about 90% of DRG neurons did not respond to ATP or α,β-meATP, and only a small percentage of neurons exhibited slowly desensitizing currents after the application of ATP, but were not activated by α,β-meATP [57, 58]. Most of these cells did belong to the medium-sized subgroup of DRG neurons, which are endowed with the P2X2 receptor subtype [12].
While the involvement of homomeric P2X3 and heteromeric P2X2/3 receptors in nociception is broadly accepted, homomeric P2X2 receptors have probably no major role in the transmission of pain. In fact, P2X2 knockout mice did not exhibit alterations in acute nocifensive behavior in response to intraplantar injection of P2X receptor agonists and react to acute thermal nociceptive stimulation with unchanged intensity [58]. These data suggest that P2X2 and also P2X2/3 receptors are probably not essential in mediating acute pain stimuli. By contrast, in the second phase of their responses to formalin, P2X2 knockout mice showed deficits in pain-related behaviors [58] that may be attributed to the loss of heteromeric P2X2/3 receptors.
The first indication for the functional expression of P2X receptors in spinal dorsal horn neurons was provided by investigations of Jahr and Jessell [59] who observed an excitation of a subpopulation of cultured spinal dorsal horn neurons by ATP. In rat spinal cord slice preparations, the application of ATP and ATPγS to lamina II neurons [60] and lamina V neurons [61], respectively, induced inward currents, suggesting the occurrence of functional P2X receptors. In the dorsal horn of the spinal cord, both mRNA and receptor protein for the P2X1–6 subtypes were detected, indicating their possible presence on second-order sensory neurons [28, 36, 62, 63]. In dorsal horn neurons, the highest expression levels have been shown for P2X2, P2X4, and P2X6 receptors; the P2X3 receptor was also present but at a lower level [36, 50]. In addition, P2X1, P2X2, and P2X3 receptors have been found to be localized at the terminals of primary afferent fibers that may belong to the most important sites involved in sensory signal regulation [64]. It is suggested that the activation of presynaptically localized P2X receptors may directly depolarize primary afferent fibers to initiate nociceptive signals, which are then transmitted to lamina neurons [65]. In this respect, P2X3 receptor-expressing terminals have been described to be restricted to the inner layer of lamina II [66]. Patch-clamp recordings from lamina I neurons in a spinal cord slice preparation also provided evidence for the expression of P2X receptors on many capsaicin-sensitive afferent fibers innervating lamina I neurons [65], whereas P2X receptor-expressing afferent fibers projecting onto lamina V neurons were capsaicin-insensitive Aδ-fibers [67]. Regrettably, due to the lack of selective agonists and antagonists, the respective P2X receptor subtypes could not be functionally identified.
An increasing body of evidence suggests the involvement of P2X4 receptors expressed at high levels by activated spinal microglia cells in neuropathic pain sensation [68, 69]. After stimulation by ATP, diffusible factors, such as tumor necrosis factor-α (TNF-α) and cytokines, released from microglia, may modulate neuronal pain processing within the spinal dorsal horn.
P2Y Receptors
In contrast to the plethora of data related to the role of P2X3 receptors in pain, only little is known about the involvement of P2Y receptors in sensory transmission and even this limited amount of data is somewhat controversial. However, a few studies have suggested that P2Y receptors contribute to pain transmission in an antinociceptive rather than nociceptive way [70, 71]. Recently, UTP-/UDP-sensitive P2Y receptors were shown to be involved in producing antiallodynic effects after ligation of the sciatic nerve in rats [70]. In contrast, both, ATP and α,β-meATP induced a gradually developing and long-lasting hyperalgesic effect in the same model, indicating the opposing effects of pain-relevant P2Y and P2X receptor subtypes in nociception [72].
Whereas in the rat spinal cord, P2Y2, P2Y4, and P2Y6 receptor mRNA was detected by means of reverse transcription-polymerase chain reaction, the presence of P2Y2 and P2Y4 receptor mRNA was found in DRG, only [70]. This finding disagrees with a recent study reporting the existence of P2Y1 and P2Y2 mRNA, but not of P2Y4 and P2Y6 mRNA, in a subset of DRG neurons [73]. Moreover, in non-neuronal DRG cells, mRNAs for P2Y2, P2Y12, and P2Y14 receptors were also found.
The observation that UTP, but not UDP, evokes sustained action potential firing in a subset of C fibers suggested the occurrence of one or more UTP sensitive P2Y receptors [70]. Furthermore, the majority of the UTP-sensitive fibers also responded to α,β-meATP demonstrating the coexpression of P2Y and P2X receptor subtypes [74].
Intrathecal administration of UTP and UDP, respectively, dose-dependently elevated the mechanical nociceptive threshold in the paw pressure test and prolonged the thermal nociceptive latency in the tail-flick test of rats [70]. Because UTP preferentially activates the P2Y2 and P2Y4 subtypes and UDP has some specificity for the P2Y6 subtype, the antinociceptive effect could be mediated by one of these receptors. Unfortunately, because of the lack of specific P2Y receptor antagonists, the receptor subtype involved could not be identified in this study. However, the involvement of a P2Y4 receptor is possible because of the existence of P2Y1 and P2Y4 mRNA in some of the dorsal horn neurons in the spinal cord [73].
Moreover, ATP and UTP, but not α,β-meATP, inhibited a slow depolarization caused by repetitive dorsal root stimulation in a subset of substantia gelatinosa neurons by activation of spinal P2Y receptors [75]. Similarly, the C-fiber-induced population of polysynaptic excitatory postsynaptic potentials (EPSPs) in the hemisected spinal cord was inhibited by ADP-β-S [71]. However, neither the non-selective P2 receptor antagonist suramin, nor the P2Y1 receptor antagonists PPADS and MRS 2179 interacted with the P2Y1,12,13 receptor agonist ADP-β-S, suggesting the involvement of a hitherto unclassified P2Y receptor subtype [71].
P2X3 Receptors in Acute Pain
Exogenously applied P2X receptor agonists induce acute pain in humans and animals. Intraplantar injection of the P2X1,2,3 and P2X2/3 receptor agonist α,β-meATP resulted in spontaneous, short-lasting licking, biting, and lifting of the injured hindpaw [39]. After local administration into the hindpaw, BzATP, which preferentially activates P2X1, P2X3, and P2X7 subtypes, also produced an acute paw flinching response [76] that was dose-dependently attenuated by the P2X1, P2X3, and P2X2/3 receptor antagonist TNP-ATP [77]. Moreover, the effect of BzATP was potentiated by coadministration of Cibacron blue, a selective allosteric enhancer of P2X3 and P2X2/3 receptor activation. Cibacron blue enhanced both agonist-induced receptor activity and recovery from desensitization of the human P2X3 receptor [76].
In human volunteers, application of low concentrations of ATP (0.2–0.6 nmol) into blister bases produced pain with a delayed onset and typically lasting up to 100 s [2]. In another study, only concentrations higher than 250 nmol ATP caused pain after intradermal injection [3]. In humans, iontophoretically applied ATP onto normal skin induced modest pain during 0–20 s of delivery, but was potentiated more than twice in hyperalgesic skin that was generated by UV inflammation and in combination with acute capsaicin treatment, respectively [78]. Usually, the pain produced by ATP diminished after several minutes, despite continuous iontophoretic administration of ATP, indicating the involvement of a fast desensitizing P2X3 receptor subtype. Considering their fast desensitization kinetics and slow recovery, the importance of homomeric P2X3 receptors in acute pain seems to be rather limited. Already, agonist concentrations far below the threshold concentration noteworthy to activate the receptor have been shown to desensitize P2X3 receptors in cultured mouse or rat sensory neurons [79]. Because nanomolar concentrations of endogenous ATP are normally found in the extracellular space [80, 81], a significant fraction of homomeric P2X3 receptors on nociceptive neurons should be desensitized, and thus, unable to sense changes in ATP concentrations produced after tissue damage [79]. However, a recent study contradicts this view. A/J mice exhibit a reduced magnitude of acute nocifensive behavior after intraplantar injection of α,β-meATP in comparison with other strains. In cultured capsaicin-sensitive DRG neurons, P2X3 protein and mRNA levels as well as an increase in intracellular calcium concentration, which were evoked by α,β-meATP, indicated a lower expression of P2X3 receptors in the A/J mouse strain compared to C57BL/6 J mice [82]. Hence, down-regulation of sensory P2X3 receptors was postulated to be one reason for low sensitivity to tissue injury pain.
In several models of acute nociception in rats and mice, the administration of the selective non-nucleotide P2X3/P2X2/3 receptor antagonist A-317491 was not effective [83, 84]. Neither acute thermal nor mechanical nociceptive stimuli were antagonized by subcutaneous application of this antagonist. A marginal suppression of pain-related behaviors was found after intraplantar capsaicin administration, only. Surprisingly, tetramethylpyrazine that has been used in traditional Chinese medicine as an analgesic, decreased acute paw flinching responses induced by α,β-meATP injection into the hindpaw and reduced current responses mediated by P2X3 receptors in isolated DRG neurons [85].
Indication for the relevance of P2X3 receptors in mediating acute pain results also from observations made in P2X3 receptor null-mutant mice [44, 45] or after continuous intrathecal delivery of P2X3 receptor antisense oligonucleotides [86]. In P2X3-null mice injection of ATP into the hindpaw evoked a significantly decreased nociceptive behavior compared to wild-type mice [44]. In contrast, administration of capsaicin instead of ATP evoked normal pain responses. It is notable that in this study, responses to noxious thermal and mechanical stimuli were similar in \( {\text{P2X}}^{{ - \mathord{\left/ {\vphantom { - - }} \right. \kern-\nulldelimiterspace} - }}_{3} \) and wild-type mice suggesting the lack of P2X3 receptor involvement in the mediation of both sensations, whereas another group has reported that \( {\text{P2X}}^{{ - \mathord{\left/ {\vphantom { - - }} \right. \kern-\nulldelimiterspace} - }}_{3} \) mice display altered neural processing of mild “warming” thermal stimuli [45].
The formalin test is considered as one of the widely used standard animal models of nociception [87]. After injection of formalin into the hindpaw of mice, two distinct phases of nociceptive behaviors can be distinguished. The first, acute phase can be observed at about 5 min after formalin application and may result from a direct stimulation of C-fibers. The second, persistent phase develops after about 15–30 min and appears to depend on an inflammatory reaction in the peripheral tissue combined with functional changes in the dorsal horn of the spinal cord [87]. Whereas there is, in principle, agreement on the involvement of P2X3 receptors in the late phase of nociceptive behavior [39, 45, 88, 89], some controversial data exist regarding the role of spinal P2X3 receptors in the first, transient phase of formalin-induced nociception. Intraplantar pretreatment with α,β-meATP and subsequent subplantar formalin injection or coadministration of ATP and formalin did not enhance hindpaw licking and lifting [39, 88]. In contrast, intrathecal administration of the nonselective P2 receptor antagonist PPADS or the P2X1, P2X3, P2X2/3 receptor antagonist TNP-ATP, respectively, reduced the first phase without any effect on the second phase of the formalin test [90]. Because both phases of formalin-evoked nociceptive behaviors were potentiated by Cibacron blue, a selective allosteric enhancer of P2X3 receptor function [89], the involvement of P2X3 receptors in acute and inflammatory pain (see below) is of strong likelihood.
This assumption is supported by a recent study investigating pain behaviors of P2X2 receptor null mice in the formalin model [58]. Interestingly, \( {\text{P2X}}^{{ - \mathord{\left/ {\vphantom { - - }} \right. \kern-\nulldelimiterspace} - }}_{2} \) mice did not show alterations in nocifensive responses in the acute phase, but revealed deficits in nocifensive responses in the second phase. Moreover, intraplantar injection of ATP or α,β-meATP resulted in a dose-dependent increase in typical pain behaviors like lifting and biting the treated hindpaw in both \( {\text{P2X}}^{{ + \mathord{\left/ {\vphantom { + + }} \right. \kern-\nulldelimiterspace} + }}_{2} \) and \( {\text{P2X}}^{{ - \mathord{\left/ {\vphantom { - - }} \right. \kern-\nulldelimiterspace} - }}_{2} \) mice excluding an involvement of P2X2 receptors in acute nocifensive behaviors. These data suggest that P2X2 and P2X2/3 are probably not important for acute pain sensation. Hence, homomeric P2X3 receptors may be sufficient for mediation of ATP or α,β-meATP induced acute pain-related behaviors.
The potential role of the spinal glutamate-NMDA receptor system in acute nociceptive signaling induced by α,β-meATP has repeatedly been demonstrated [91–93]. Presynaptically localized P2X3 receptors may increase glutamate release from the first sensory synapse in the spinal cord [92]. Nocifensive behavior which was evoked by hindpaw administration of ATP, α,β-meATP, or BzATP appeared to involve spinal release of excitatory amino acids, as the intrathecally delivered NMDA receptor antagonist MK-801 reduced the number of nociceptive events after the injection of the P2 receptor agonists [94]. The nocifensive behavior triggered by ATP and BzATP, but not by α,β-meATP and formalin, was also reduced by intrathecally injection of a neurokinin-1 (NK-1) receptor antagonist. Thus, two sets of fibers that were activated by ATP and BzATP or by α,β-meATP may contribute to the spontaneous, short lasting nocifensive behaviors.
P2X3 Receptors in Inflammatory Pain
Pain sensation as a result of P2X receptor activation is greatly increased in inflamed tissue. In normal rats, injection of α,β-meATP at ≥5 nmolar concentrations into the hindpaw is required to induce nocifensive behaviors like paw lifting and licking [95]. However, a comparable pain-related behavior was caused in rats by the application of a 100-fold lower α,β-meATP concentration after the injection of intraplantar carageenan into the hindpaw or irradiation with ultraviolet.
During acute inflammation, high concentrations of extracellular ATP have been measured on the sites of tissue injury in experimental animals and in arthritic patients [9, 10, 96, 97]. High extracellular levels of ATP originated not only from damaged cells, but also from non-damaged endothelial cells [98], and in consequence, ATP may modulate vascular perfusion of the damaged tissue and stimulate immune response [99] or may produce nociceptive responses and hyperalgesia. The already mentioned algogenic action of ATP, after its application into blister base preparations of human volunteers, was potentiated under conditions of inflammation [2, 100]. In inflamed tissue, pH values as low as 5.5 have been observed [101, 102]. Hence, an increase in P2X receptor conductance under acidic conditions (for P2X2 and P2X2/3 receptors see [103, 104]) could contribute to the algogenic effect of ATP.
An elevated P2X receptor activity can also result from the enhanced expression of this receptor in inflamed tissue and can contribute to abnormal pain responses associated with inflammatory injuries. In the CFA model, a potentiation of the current responses to ATP was observed in isolated DRG neurons due to an enhanced expression of the P2X2 and P2X3 receptor protein [105]. Similarly, in TG neurons, the P2X3 receptor expression was increased already 1 day after induction of masseter muscle inflammation by CFA [106]. Interestingly, in contrast to the results with DRG neurons, the P2X3 receptor expression in TG neurons was not limited to small-sized (muscle afferent) neurons but was also observed in the medium-sized (cutaneous afferent) neuronal population. TG neurons co-expressed P2X3 with either calcitonin gene-related peptide or substance P, and P2X3 receptor expression was increased in both neuronal populations after CFA treatment [106]. Recently, it was demonstrated that under the same conditions the levels of CGRP and substance P were also elevated [107]. This might be of particular importance because CGRP can up-regulate P2X3 receptor mRNA levels in TG neurons as it was shown in migraine pain ([108], see below).
There are numerous reports demonstrating antinociceptive effects of P2X3 receptor antagonists in different models of inflammatory pain in vivo providing strong evidence for the involvement of P2X3 receptors in acute and chronic inflammatory pain. Moderate decrease in nociceptive behavior in the tail-flick assay was observed after spinal instillation of various nonselective P2 receptor antagonists like suramin, Evans blue, trypan blue, or reactive blue 2, but not after application of PPADS [109]. Intrathecal administration of suramin caused significant antinociception in the formalin test [109] and inhibited the noxious electrically evoked responses of dorsal horn neurons 3 h after carageenan injection into the rat hindpaw but not in control animals [110]. In the same model, the nonselective PPADS was ineffective. During the second phase of formalin-evoked nociceptive behavior in the rat, the P2X1,3 receptor antagonistic PPADS [90] and TNP-ATP [89] were both effective in suppressing pain-relevant behavioral changes. In experimental pain models of both the CFA-induced inflamed paw [111, 112] and CFA-induced monoarthritis of the temperomandibular joint [111], TNP-ATP dose-dependently reduced the mechanical hypersensitivity.
ATP and α,β-meATP elevated the responsiveness of nociceptors in skin which had been inflamed with carrageenan treatment [113] or ultraviolet irradiation [78]. In rats with monoarthritis, α,β-meATP but not the selective P2X1 receptor agonist β,γ-meATP decreased pressure pain threshold, confirming the immunohistochemically documented enhancement of P2X3 receptor expression in trigeminal ganglion neurons [111]. In contrast, the injection of α,β-meATP into the knee joint of anesthetized rats suffering from chronic arthritis did not change C- and Aδ-fiber responses [114]. Although primary afferent terminals in the dorsal horn of the spinal cord show P2X3 receptor immunoreactivity [36, 66], intrathecal instillation of α,β-meATP did not influence C-fiber evoked responses of dorsal horn neurons in carrageenan-inflamed rats [110]. In addition, in in vivo recordings of dorsal horn neurons, both threshold and suprathreshold responses evoked by electrical stimulation of C- and Aδ-fiber primary afferents were comparable in wild-type and P2X3 knockout mice [45]. These results are somewhat puzzling, because nociceptive behaviors as a result of inflammatory pain after injection of CFA or formalin into the hindpaw of rats was significantly reduced by continuous intrathecal administration of P2X3 receptor antisense oligonucleotides [115]. Moreover, P2X3 knockout mice showed a reduced formalin-induced flinching behavior in both acute and persisting phase [44], but surprisingly, an enhanced thermal hyperalgesia in chronic inflammation compared to the wild-type animals [45]. Finally, P2X3 receptor knockdown after treatment with P2X3 antisense oligonucleotides dose-dependently decreased CFA-induced thermal hyperalgesia [115].
Hence, it is quite conceivable that spinal P2X3 receptors are not essentially involved in every pain state produced by the different experimental models of inflammation, and moreover, the involvement of other receptors or ion channels should also be considered. In this context, the involvement of P2X receptor-subtypes other than P2X3 in chronic inflammatory pain has recently been postulated. In tissue sections of injured nerves of patients suffering from persistent neuropathic pain and hypersensitivity after trauma, an elevated P2X7 receptor immunoreactivity was observed [32]. However, P2X7 receptor immunostaining was not detected in sensory neurons of human dorsal root ganglia, but was present in satellite cells surrounding these neurons [32].
Local administration of oxidized ATP, a selective P2X7 receptor antagonist, relieves inflammatory pain in arthritic rats [116, 117]. In mice lacking the P2X7 receptor, inflammatory hypersensitivity was completely absent in the CFA model [32], and the development of arthritis after injection of collagen into their joints was reduced [118]. Thus, inflammation may cause P2X7 receptor-dependent release of interleukin-1β, which in turn stimulates the production of other algogens, such as nerve growth factor, cyclooxygenase 2, and superoxide products [119–121]. Thereby, a vicious circle may develop because activation of the inflammatory cascade initiates degenerative and pathological changes, which in turn may elevate inflammatory and/or neuropathic insults. Hence, drugs that specifically inhibit P2X7 receptor function may have analgesic properties and may reduce inflammatory or neuropathic pain [122].
Furthermore, pain processing may also be influenced by activated microglia cells which have been shown to express high levels of P2X7 receptors [62, 123, 124]. Both peripheral nerve injury and inflammation leads to hypertrophy, proliferation, and activation of microglia [125]. In addition to P2X7 receptors, microglia cells express receptors for a host of mediators released during inflammation, such as substance P, calcitonin gene-related peptide (CGRP), and excitatory amino acids [126]. Interactions between the receptors for these agonists and the P2X7 receptor may have consequences for the functioning of pain transmission pathways.
Inflammation results in the production of a multiplicity of cytokines, growth factors, and inflammatory mediators, which can directly activate the nociceptors or may interact with ligand-gated ion channels [112]. Inflammatory mediators, such as substance P and bradykinin, potentiated currents through ATP receptor channels containing the P2X3 subunit [127]. However, the regulatory effect did not result from a direct modulatory action of substance P or bradykinin on the P2X3 or PX2/3 receptor, like it has been shown for the recombinant P2X2 receptor [128], but rather on an interaction between the receptors for substance P and bradykinin with the P2X receptor, which was mediated by a protein kinase-dependent mechanism.
Pain hypersensitivity elicited by intraplantar administration of multiple inflammatory mediators, such as prostaglandins of the E type and bradykinin, or P2X3 receptor agonists, is reduced or absent in mice with mutation of the SCN11A gene that encodes the voltage-gated sodium channel Nav1.9 [129]. In DRG neurons of the mouse, Nav1.9 was highly coexpressed with P2X3 receptors, which suggests that this sodium channel is a downstream effector of the increased pain sensitivity produced by α,β-meATP [129].
Members of the MAPK cascade such as nerve growth factor and extracellular signal-regulated protein kinase (ERK) have been shown to be involved in pain transmission and sensitization in DRG neurons and spinal dorsal horn [16, 130, 131]. Intrathecally applied nerve growth factor induced novel expression of P2X3 receptors at cervical and lumbar DRG neurons and at axons projecting to lamina I and outer lamina II of the spinal dorsal horn and to the ventromedial afferent bundle beneath the central canal [132].
ERK, in turn, induces prodynorphin and NK-1 up-regulation and contributes to persistent inflammation and hyperalgesia [130]. In CFA inflamed rats, both α,β-meATP injection into the damaged paw and mechanical stimulation of the hindpaw increased the phosphorylated extracellular signal-regulated protein kinase (pERK) immunoreactivity in primary afferent neurons [112]. It has been shown that about 75% of the pERK-labeled DRG neurons coexpress P2X3 receptors [112]. Most of the neurons labeled for pERK belonged to the small-sized subgroup of DRG neurons, but some of them were medium-sized A-fiber neurons, which may possess heteromeric P2X2/3 receptors [4]. The rise in pERK immunoreactivity occurred already several minutes after α,β-meATP treatment and was significantly, but not completely, decreased in the presence of PPADS or TNP-ATP. This and the ineffectiveness of the selective P2X1 receptor antagonist IP5I [133], strongly indicated the inclusion of a P2X3 receptor subtype in the induction of hypersensitivity towards mechanical stimulation during peripheral inflammation.
Furthermore, P2X3 receptors localized on sensory neurons interact with proteinase-activated receptors (PAR) that are supposedly involved in tissue inflammation and repair [134]. PARs belong to the family of G protein-coupled receptors and are expressed by small-sized DRG neurons, and after activation, may facilitate the release of substance P and CGRP in peripheral tissues [135]. Activation of PAR reduced the threshold of pain-like behavior after administration of α,β-meATP into the hindpaw of rats and augmented the α,β-meATP induced Fos expression in laminae I and II of the spinal dorsal horn [136]. In contrast, Shimizu and coworkers [137] reported that enhanced cFos expression after the exposure of one hindpaw to heat persisted in mice, in spite of the genetic deletion of their P2X3 receptors.
However, not only peripheral and spinal, but also supraspinal P2X3 and P2X2/3 receptors may be involved in the transmission of inflammatory pain. Antinociceptive effects in peripheral tissues were registered after bilateral microinjecton of α,β-meATP into the nucleus locus coeruleus [138] and intracerebroventricular instillation of α,β-meATP [139]. Furthermore, intracerebroventricular administration of the selective P2X3 receptor antagonist A-317491 or pretreatment with antisense oligonucleotides for the P2X3 gene decreased inflammatory nociceptive behaviors induced by intraplantar injection of formalin and intraperitoneal injection of acetic acid [139]. The authors postulated the release of endogenous ATP that may inhibit pain transmission via activation of supraspinal P2X3 and/or P2X2/3 receptors, and in this way, may relief pain sensation.
Altogether, these findings support an outstanding role of P2X3 receptors in inflammatory pain processing, although many details and inconsistencies still expect further clarification.
P2X3 Receptors in Chronic Neuropathic Pain
Neuropathic pain syndromes are clinically characterized by spontaneous and evoked types of pain, which arise from damage or disease within the nervous system [140]. In the absence of stimulation, nociceptors are normally silent. However, these neurons may become abnormally sensitive and may develop pathological spontaneous activity after peripheral nerve lesion. Moreover, inflammatory reactions of the damaged nerve trunk can induce ectopic nociceptor activity. There is a great deal of evidence indicating the involvement of P2X3 receptors in painful peripheral neuropathies [83, 141–143]. It is widely accepted that the expression of peripheral P2X3 receptors is regulated by peripheral nerve injury. However, between single studies are discrepancies regarding the direction of the change, even though most investigators report an up-regulation of P2X3/P2X2/3 receptor expression or function in different models of neuropathic pain.
An increased P2X3 receptor expression in DRG and spinal cord was observed after chronic constriction injury of the sciatic nerve [144] and in trigeminal ganglia after mandibular inferior alveolar nerve injury [49]. An enhanced expression of P2X3 receptors was only observed on intraspinal terminals of small and medium diameter primary sensory neurons and in the ipsilateral spinal dorsal horn [144]. In contralateral, uninjured nerves, no ectopic sensitivity to ATP was observed [141]. Using in situ hybridization, reduced levels of P2X3 receptor mRNA in rat sensory ganglia were detected in axotomized neurons, but increased levels in adjacent intact neurons [145]. These data suggest an elevated synthesis of the P2X3 receptor protein in pain-relevant neurons. Interestingly, whereas the total amount of P2X3 receptor protein did not change, the membrane fraction of this protein increased in DRG several days after spared nerve injury, suggesting that nerve injury promotes trafficking of the P2X3 receptor to the cell surface but does not elevate total expression of the P2X3 receptor in the cytoplasm [143]. Furthermore, the elevated membrane expression of the P2X3 receptor was accompanied by an increase in receptor sensitivity without any change in extracellular endogenous ATP levels.
In contrast, after sciatic nerve axotomy, down-regulation by more than 50% of P2X3 receptor expression was found in DRGs of the lumbar segments 4 and 5, which was completely reversed after intrathecally delivered glial cell line-derived neurotrophic factor (GDNF) [37]. A decrease in P2X3 receptor expression was accompanied by reduced current responses towards α,β-meATP in acutely isolated DRG neurons 2 weeks after L5/L6 spinal nerve ligation [146]. However, subsets of small and large DRG neurons maintained unchanged P2X3 receptor expression and function. These neurons possibly contribute to neuropathic pain [146]. Similar to the decrease in P2X3 receptor immunoreactivity in rat DRG after peripheral axotomy, there was a significant decrease in numbers of P2X3-like immunoreactive neurons in intact post mortem human DRG after central axotomy [147].
The local administration of P2X receptor agonists has repeatedly been shown to increase thermal and mechanical hyperalgesia and allodynia in chronic constriction sciatic nerve injury [86, 143, 148]. After nerve injury, the usefulness of nonselective or selective P2 receptor antagonists or P2X3 antisense oligonucleotides in reducing neuropathic pain was also demonstrated. In the spared nerve injury model, allodynia and α,β-meATP-induced flinching were effectively reversed by PPADS and TNP-ATP (an antagonist of the P2X1, P2X3, and P2X2/3 subtypes, [143]). Furthermore, treatment with the more specific P2X3/P2X2/3 receptor antagonist A-317491 reduced the excitability of dorsal horn neurons in the chronic constriction injury model of neuropathic pain, compared with sham-operated rats, suggesting an antinociceptive effect after the blockade of P2X3 receptors [149]. After subcutaneous injection, the active S- but not the inactive R-enantiomer of A-317491 dose-dependently reduced thermal hyperalgesia and mechanical allodynia in both the Bennett model and the CFA-induced thermal hyperalgesia [83].
Evidence for the involvement of P2X3 receptors in neuropathic pain also results from the observation that down-regulation of P2X3 receptors reduces hyperalgesic and allodynic responses of rats with ligated nerves [115, 148]. A distinct decrease of P2X3 mRNA in the DRG and P2X3 receptor protein in inner lamina II of the dorsal horn of the spinal cord, combined with reduced mechanical hyperalgesia, was reported [150, 151]. The effects of antisense oligonucleotides on nociceptive indices were observed in the ipsilateral, but not in the contralateral, paw in both models. Moreover, intrathecal injection of P2X3 antisense oligonucleotides attenuated the hyperalgesia and allodynia after the nerve injury [82, 86].
Recently, P2X4 receptors with no previously known connection to nociception have been described as participants in neuropathic pain. Tsuda and co-workers [68] have demonstrated that ligation of rat peripheral sensory nerves stimulates P2X4 receptor expression in microglia on the ipsilateral side of the spinal cord. Significant P2X4 receptor accumulation was detected as early as 1 day after lesion [152]. Both, pharmacological blocking by TNP-ATP and the intrathecal administration of antisense oligonucleotides targeting P2X4 receptors reduced the resulting neuropathic pain [68]. Vice versa, stimulation of P2X4 receptors in microglia caused and maintained allodynia. It is conceivable that processing of neuropathic pain may involve diffusible factors like plasminogen or TNF-α, which were released by microglia after P2X4 receptor activation and may modulate neuronal pain signaling [69]. Interestingly, in contrast to the nerve injury model, chronic inflammation after administration of complete Freund’s adjuvant was not associated with P2X4 receptor up-regulation [68] and microglia activation [153].
P2X3 Receptors in Visceral Pain
ATP can be released from epithelial cells upon distension of hollow visceral organs and was, for the first time, identified as a motor neurotransmitter in the urinary bladder of the guinea pig in 1972 [154]. More recently, the involvement of ATP in sensory neurotransmission in the rabbit bladder was detected [8, 44]. This sensory function may be important for the physiological action of bladder filling and emptying cycles but also for nociception in pathological states [11, 44]. Birder and coworkers [155] have suggested that urothelial cells share a number of similarities with sensory neurons and may have “neuron-like” properties.
In dependence on the magnitude of distension, different amounts of ATP are released from epithelial cells of hollow organs [8, 156]. After moderate distension, low extracellular ATP concentrations would stimulate P2X receptors on intrinsic sensory fibers and contribute to peristalsis. In the bladder, ATP was suggested to act on P2X1 receptors of the detrusor muscle mediating contraction. Excessive distension would release large amounts of ATP that may activate P2X receptors situated on extrinsic sensory nerves, which then relay pain signals to the central nervous system, finally resulting in colic pain. Evidence has been accumulated supporting this hypothesis. In rats, enhancement of nerve discharges has been observed during distension of the urinary bladder and application of α,β-meATP to a bladder–pelvic preparation, which was prevented by the unselective P2 receptor antagonist suramin [157]. Moreover, with increasing postnatal age, the expression of P2X3 receptors rose in rat urothelial cells and suburothelial plexus, but did not change in detrusor and serosa [158]. The peak expression was reached at postnatal days 14–21, followed by a decline to values that were observed after birth. Interestingly, in the same study, the expression of the P2X2 receptor subunit decreased with age in urothelial cells.
P2X3 knockout mice have been found to have not only a loss in the rapidly desensitizing currents in sensory neurons, but also a marked urinary bladder hyporeflexia, characterized by an impaired voiding frequency and an increased bladder capacity [44, 159]. Because the loss of P2X3 receptors might decrease sensory neuron activity during bladder filling, and in consequence, disturb micturition reflex, selective modulation of P2X3 receptors may provide new treatment strategies for many bladder storage disorders.
Pain is the most troubling symptom to patients with interstitial cystitis [160]. Several studies have shown that bladder urothelial cells from patients with interstitial cystitis release more ATP after stretching than those from control patients. The released ATP may activate P2X3 receptors, which are expressed in the urothelium of patients but also, to a lower degree, of healthy persons [160, 161]. Moreover, P2X2 receptors were detected in human urothelium, also suggesting the expression of P2X2/3 heteromeric receptors [160]. Similarly, an increase in P2X3 immunoreactivity was detected in suburothelial nerve fibers in bladder biopsies of patients with refractory neurogenic detrusor overactivity. The up-regulation of P2X2 and P2X3 receptors in interstitial cystitis was accompanied by an elevated protein expression, and a decrease in P2X3 gene expression, whereas the expression of the P2X2 gene remained unchanged [160, 161]. In contrast to the up-regulation of P2X3 receptors in urothelium in interstitial cystitis, P2X3 (and/or P2X2/3) receptor activity in lumbrosacral dorsal root ganglion neurons innervating the urinary bladder was decreased in the rat model of cyclophosphamide-induced cystitis [162].
ATP is suggested to be also an enteric transmitter because the P2X3 receptor is expressed by specific functional groups of enteric neurons. P2X3 receptors were localized on nerve cells of the mesenteric ganglia of the stomach, small and large intestines, and on nerve cells of the submucosal ganglia in the small and large intestine of the guinea pig [163]. These neurons were shown to be excitatory and inhibitory muscle motor neurons, ascending interneurons and cholinergic secretomotoric neurons, suggesting an involvement of P2X3 receptors in enteric mechano- and chemosensitivity. In most cases, the P2X3 receptor was not co-localized with the P2X2 subunit on the same neuron, with the exception of some nitric oxide synthase-immunoreactive neurons where both subunits form heteromers [163].
Retrograde labeling combined with immunocytochemistry indicated that small- to medium-sized neurons from the DRG at levels T8–L1 and L6–S1 innervate the descending colon of mice [164]. More than one-third of the retrogradely labeled cells expressed the P2X3 receptor subtype. This value corresponds well with the P2X3 receptor endowment of the whole DRG population, where about 40% of the neurons were P2X3 positive. Hence, the P2X3 receptor might have an important role in the transmission of noxious signals from the colon.
One of the most common abdominal pain syndromes is the irritable bowel syndrome (IBS), which is characterized by enhanced visceral sensation and abdominal pain [165]. Comparable to interstitial cystitis, P2X3 receptor expression is up-regulated in colonic nerve fibers of patients suffering from IBS [166]. Several studies have shown that α,β-meATP may excite gastrointestinal afferents [167–169]. α,β-meATP induced a reproducible, concentration-dependent excitation of lumbar splanchnic nerve afferents that was reversed by the P2 receptor antagonist PPADS [170]. Recently, it has been demonstrated that lumbar splanchnic nerves, which terminate in the thoracolumbal spinal cord, are more likely to express P2X3 receptors than paired sacral pelvic nerves, which terminate in the lumbrosacral spinal cord [171].
Intraparenteral injection of acetic acid provoked visceral pain in mice that was attenuated by the P2X1–3 receptor antagonist TNP-ATP and the nonselective antagonists PPADS and suramin [172]. IP5I, the selective P2X1 receptor antagonist, was ineffective. Thus, P2X3 and/or P2X2/3 receptors, which are activated by endogenously released ATP appear, to play a role in acetic acid-induced abdominal pain. Interestingly, the antinociceptive potency of TNP-ATP was comparable to that of morphine in blocking acetic acid-induced abdominal constriction [172].
P2X3 Receptors in Migraine Pain
The involvement of ATP in migraine was first suspected in conjunction with the vascular theory of this disorder [108, 174]. Currently and largely based on animal models, migraine is also hypothesized to involve neuronal dysfunction in brain areas that mediate nociception, particularly, the trigeminal nerve, spinal trigeminal nucleus, and thalamus [106, 108]. Conceivably, ATP, released in pain attack, may activate P2X3 receptors, which are endogenously expressed by a considerable portion of trigeminal nociceptive neurons.
In the last years, evidence has accumulated that the neuropeptide CGRP, which is a potent vasodilator and pro-inflammatory agent, may play a major role in migraine [173]. Activation of trigeminal nerves enhances the release of CGRP and other peptides that, in turn, cause the release of pro-inflammatory mediators [174]. These mediators may additionally stimulate CGRP synthesis and release over hours to days. CGRP did not only elevate the concentration of pro-inflammatory molecules, but also enhanced P2X3 receptor conductance in an in vitro model of cultured trigeminal nociceptive neurons [108]. This effect peaked 5 h after CGRP treatment and was accompanied by an up-regulation of P2X3 mRNA and protein synthesis. Furthermore, CGRP did not increase agonist sensitivity but accelerated recovery of the P2X3 receptor from desensitization, which possibly contributed to the elevated P2X3 receptor function. Interestingly, the effect of CGRP was selective and limited to the P2X3 receptor because TRPV1 receptor function has not been changed.
Whereas most trigeminal neurons coexpress P2X3 receptors and CGRP binding sites [106], in DRG neurons, only a low expression of CGRP binding sites, and moreover, an infrequent coexpression with P2X3 receptors was found [175]. In contrast to the effects on trigeminal neurons, in DRG neurons, no increase in P2X3 receptor function by CGRP was observed [108]. Hence, coexpression of both P2X3 receptors and CGRP binding sites in the same neuron seems to be a precondition for the increase in P2X3 receptor activity by CGRP. It is possible that P2X3 receptor conductance was stimulated through second messenger mechanisms, which were activated by CGRP binding.
P2X3 Receptors in Cancer Pain
Until now, a wide variety of P2X and P2Y receptors has been detected in numerous cancer tissues. An excellent review summarizing the present knowledge about the role of P2 receptors in cancer has been published recently [176]. Whereas most studies focus upon involvement of different P2 receptor subtypes in tumor growth and apoptosis, only sparse and if available, discrepant information exists concerning the role of ATP in cancer pain. Interestingly, tumor tissues contain ATP in exceptionally high concentrations, which may be released during growth of the tumor [177], and moreover, may activate nociceptive nerve endings.
An elevated P2X3 receptor function compared to control animals was observed in DRG neurons, which were prepared from rats with gastric ulcers induced by acidic acid injection into the wall of the distal stomach [178]. Whereas in saline-treated controls, 38 and 29% of the cells did respond to ATP and α,β-meATP with inward currents, respectively; the number of responsive cells was enhanced in rats with gastric ulcer. Furthermore, P2X3 receptor currents showed decelerated desensitization kinetics in DRG neurons prepared from tumor-expressing rats compared to their controls. In contrast, in the same model, virtually all nodose ganglion neurons prepared from the saline-treated group produced inward currents after application of ATP and α,β-meATP, suggesting the involvement of specific gastric sensory neurons in gastric ulcer pain.
In a murine model of bone-cancer pain, in which a tumor develops within the calcaneus bone and in the surrounding subcutaneous tissue, about one-third of C-fiber nociceptors that are located in the skin overlying the tumor exhibited spontaneous activity [179]. This effect was accompanied by a decrease in the number of protein gene product 9.5 (PGP 9.5) labeled epidermal nerve fibers, a phenomenon, which is characteristic in cancer-evoked hyperalgesia [180] and also in a variety of neuropathic conditions in humans [181]. Hence, the decline in PGP 9.5-immunoreactive epidermal nerve fibers suggested the involvement of a neuropathic component in this model of bone-cancer pain. After implantation of osteolytic fibrosarcoma cells in and around the calcaneus bone, an increased P2X3 receptor expression was found in a subset of nociceptive epidermal nerve fibers during tumor growth, although the total number of nociceptive epidermal nerve fibers decreased [180]. In this subpopulation of nociceptive fibers, P2X3 receptor immunoreactivity was co-localized with immunoreactivity for CGRP. In another study investigating migraine pain, CGRP has stimulated the up-regulation of P2X3 receptors in trigeminal sensory neurons [108], implying an interplay between P2X3 and CGRP (see above). Hence, CGRP may enhance trafficking of P2X3 receptors to the cell-surface membrane in the calcaneus bone tumor model, as it was already shown for trigeminal sensory neurons [108].
The close association between the levels of CGRP and P2X3 receptors was also demonstrated in a new rat model of adenoid squamous cell carcinoma [182]. In this model, an elevated expression of CGRP and P2X3 receptors, but also of substance P and TRPV1 receptors has been found in trigeminal ganglia. The over-expression of these molecules was supposed to be involved in the mechanical and thermal hypersensitivity observed in rats with oral tumors via a facilitation of nociceptive transmission.
Concluding Remarks
The understanding of how pain is processed at each stage in the peripheral and central nervous system is the precondition to develop new therapies for the selective treatment of different states of pain. Especially, the specific expression of P2X3 receptors on pain relevant sensory afferent neurons favors this receptor subtype as a potential target for the development of new analgesic drugs. Despite the plethora of data dealing with the role of P2X receptors, primarily P2X3 and P2X2/3 receptors, in pain transmission, a final evaluation seems to be far away. In particular, the degree of involvement of this receptor subtype in migraine and tumor pain has to be elucidated. The recently described interactions between P2X3 receptors and neuropeptides and the discovery of other P2 receptor subtypes like P2X4 and P2X7 that are supposed to be involved in the mediation of painful stimuli make clear that the mechanisms of the algogenic action of ATP are more complex than originally assumed.
Abbreviations
- BBG:
-
Brilliant blue G
- BzATP:
-
2′- and 3′-O-(4-benzoyl-benzoyl)-ATP
- CFA:
-
complete Freund’s adjuvant
- CGRP:
-
calcitonin gene related peptide
- DRG:
-
dorsal root ganglion
- ERK:
-
extracellular signal-regulated protein kinase
- Ip5I:
-
di-inosine pentaphosphate
- IBS:
-
irritable bowel syndrome
- α,β-meATP:
-
α,β-methylene ATP
- 2-MeSATP:
-
2-methylthio ATP
- NK-1:
-
neurokinin-1
- PAR:
-
proteinase-activated receptors
- PPADS:
-
pyridoxal-phosphate-6-azophenyl-2′, 4′-disulfonic acid
- RB2:
-
reactive blue 2
- TG:
-
trigeminal ganglion
- TNP-ATP:
-
trinitrophenyl-substituted ATP
- TRPV1:
-
transient receptor potential vanilloid 1
References
Collier HO, James GW, Schneider C (1966) Antagonism by aspirin and fenamates of bronchoconstriction and nociception induced by adenosine-5′-triphosphate. Nature 212:411–412
Bleehen T, Keele CA (1977) Observations on the algogenic actions of adenosine compounds on the human blister base preparation. Pain 3:367–377
Coutts AA, Jorizzo JL, Eady RA, Greaves MW, Burnstock G (1981) Adenosine triphosphate-evoked vascular changes in human skin: mechanism of action. Eur J Pharmacol 76:391–401
Tsuda M, Koizumi S, Kita A, Shigemoto Y, Ueno S, Inoue K (2000) Mechanical allodynia caused by intraplantar injection of P2X receptor agonist in rats, involvement of heteromeric P2X2/3 receptor signaling in capsaicin-insensitive primary afferent neurons. J Neurosci 20:RC90
Hamilton SG, McMahon SB, Lewin GR (2001) Selective activation of nociceptors by P2X receptor agonists in normal and inflamed rat skin. J Physiol 534:437–445
Inoue K, Koizumi S, Ueno S (1996) Implication of ATP receptors in brain functions. Prog Neurobiol 50:483–492
Mork H, Ashina M, Bendtsen L, Olesen J, Jensen R (2003) Experimental muscle pain and tenderness following infusion of endogenous substances in humans. Eur J Pain 7:145–153
Ferguson DR, Kennedy I, Burton TJ (1997) ATP is released from rabbit urinary bladder epithelial cells by hydrostatic pressure changes—a possible sensory mechanism? J Physiol 505(Pt 2):503–511
Park W, Masuda I, Cardenal-Escarcena A, Palmer DL, McCarty DJ (1996) Inorganic pyrophosphate generation from adenosine triphosphate by cell-free human synovial fluid. J Rheumatol 23:665–671
Ryan LM, Rachow JW, McCarty DJ (1991) Synovial fluid ATP, a potential substrate for the production of inorganic pyrophosphate. J Rheumatol 18:716–720
Chizh BA, Illes P (2001) P2X receptors and nociception. Pharmacol Rev 53:553–568
Burnstock G (2000) P2X receptors in sensory neurones. Br J Anaesth 84:476–488
Burnstock G (2006) Historical review: ATP as a neurotransmitter. Trends Pharmacol Sci 27:166–176
Erb L, Liao Z, Seye CI, Weisman GA (2006) P2 Receptors, intracellular signaling. Pflugers Arch 452:552–562
North RA (2002) Molecular physiology of P2X receptors. Physiol Rev 82:1013–1067
Ji RR, Baba H, Brenner GJ, Woolf CJ (1999) Nociceptive-specific activation of ERK in spinal neurons contributes to pain hypersensitivity. Nat Neurosci 2:1114–1119
Nicke A, Baumert HG, Rettinger J, Eichele A, Lambrecht G, Mutschler E, Schmalzing G (1998) P2X1 and P2X3 receptors form stable trimers: a novel structural motif of ligand-gated ion channels. EMBO J 17:3016–3028
Rettinger J, Aschrafi A, Schmalzing G (2000) Roles of individual n-glycans for ATP potency and expression of the rat P2X1 receptor. J Biol Chem 275:33542–33547
Egan TM, Cox JA, Voigt MM (2004) Molecular structure of P2X receptors. Curr Top Med Chem 4:821–829
Egan TM, Samways DS, Li Z (2006) Biophysics of P2X receptors. Pflugers Arch 452:501–512
Gever JR, Cockayne DA, Dillon MP, Burnstock G, Ford AP (2006) Pharmacology of P2X channels. Pflugers Arch 452:513–537
Hussl S, Boehm S (2006) Functions of neuronal P2Y receptors. Pflugers Arch 452:538–551
von Kugelgen I (2006) Pharmacological profiles of cloned mammalian P2Y-receptor subtypes. Pharmacol Ther 110:415–432
Brunschweiger A, Muller CE (2006) P2 receptors activated by uracil nucleotides—an update. Curr Med Chem 13:289–312
Khakh BS (2001) Molecular physiology of P2X receptors and ATP signalling at synapses. Nat Rev Neurosci 2:165–174
Zhang XF, Han P, Faltynek CR, Jarvis MF, Shieh CC (2005) Functional expression of P2X7 receptors in non-neuronal cells of rat dorsal root ganglia. Brain Res 1052:63–70
Lewis C, Neidhart S, Holy C, North RA, Buell G, Surprenant A (1995) Coexpression of P2X2 and P2X3 receptor subunits can account for ATP-gated currents in sensory neurons. Nature 377:432–435
Collo G, North RA, Kawashima E, Merlo-Pich E, Neidhart S, Surprenant A, Buell G (1996) Cloning of P2X5 and P2X6 receptors and the distribution and properties of an extended family of ATP-gated ion channels. J Neurosci 16:2495–2507
Xiang Z, Bo X, Burnstock G (1998) Localization of ATP-gated P2X receptor immunoreactivity in rat sensory and sympathetic ganglia. Neurosci Lett 256:105–108
Kobayashi K, Fukuoka T, Yamanaka H, Dai Y, Obata K, Tokunaga A, Noguchi K (2005) Differential expression patterns of MRNAs for P2X receptor subunits in neurochemically characterized dorsal root ganglion neurons in the rat. J Comp Neurol 481:377–390
Ruan HZ, Birder LA, de Groat WC, Tai C, Roppolo J, Buffington CA, Burnstock G (2005) Localization of P2X and P2Y receptors in dorsal root ganglia of the cat. J Histochem Cytochem 53:1273–1282
Chessell IP, Hatcher JP, Bountra C, Michel AD, Hughes JP, Green P, Egerton J, Murfin M, Richardson J, Peck WL, Grahames CB, Casula MA, Yiangou Y, Birch R, Anand P, Buell GN (2005) Disruption of the P2X7 purinoceptor gene abolishes chronic inflammatory and neuropathic pain. Pain 114:386–396
Snider WD, McMahon SB (1998) Tackling pain at the source: new ideas about nociceptors. Neuron 20:629–632
Molliver DC, Wright DE, Leitner ML, Parsadanian AS, Doster K, Wen D, Yan Q, Snider WD (1997) IB4-binding DRG neurons switch from NGF to GDNF dependence in early postnatal life. Neuron 19:849–861
Bennett DL, Michael GJ, Ramachandran N, Munson JB, Averill S, Yan Q, McMahon SB, Priestley JV (1998) A distinct subgroup of small DRG cells express GDNF receptor components and GDNF is protective for these neurons after nerve injury. J Neurosci 18:3059–3072
Vulchanova L, Riedl MS, Shuster SJ, Buell G, Surprenant A, North RA, Elde R (1997) Immunohistochemical study of the P2X2 and P2X3 receptor subunits in rat and monkey sensory neurons and their central terminals. Neuropharmacology 36:1229–1242
Bradbury EJ, Burnstock G, McMahon SB (1998) The expression of P2X3 purinoreceptors in sensory neurons, effects of axotomy and glial-derived neurotrophic factor. Mol Cell Neurosci 12:256–268
Chen CC, Akopian AN, Sivilotti L, Colquhoun D, Burnstock G, Wood JN (1995) A P2X purinoceptor expressed by a subset of sensory neurons. Nature 377:428–431
Bland-Ward PA, Humphrey PP (1997) Acute nociception mediated by hindpaw P2X receptor activation in the rat. Br J Pharmacol 122:365–371
Robertson SJ, Rae MG, Rowan EG, Kennedy C (1996) Characterization of a P2X-purinoceptor in cultured neurones of the rat dorsal root ganglia. Br J Pharmacol 118:951–956
Cook SP, Vulchanova L, Hargreaves KM, Elde R, McCleskey EW (1997) Distinct ATP receptors on pain-sensing and stretch-sensing neurons. Nature 387:505–508
Ueno S, Tsuda M, Iwanaga T, Inoue K (1999) Cell type-specific ATP-activated responses in rat dorsal root ganglion neurons. Br J Pharmacol 126:429–436
North RA (2002) Molecular physiology of P2X receptors. Physiol Rev 82:1013–1067
Cockayne DA, Hamilton SG, Zhu QM, Dunn PM, Zhong Y, Novakovic S, Malmberg AB, Cain G, Berson A, Kassotakis L, Hedley L, Lachnit WG, Burnstock G, McMahon SB, Ford AP (2000) Urinary bladder hyporeflexia and reduced pain-related behaviour in P2X3-deficient mice. Nature 407:1011–1015
Souslova V, Cesare P, Ding Y, Akopian AN, Stanfa L, Suzuki R, Carpenter K, Dickenson A, Boyce S, Hill R, Nebenuis-Oosthuizen D, Smith AJ, Kidd EJ, Wood JN (2000) Warm-coding deficits and aberrant inflammatory pain in mice lacking P2X3 receptors. Nature 407:1015–1017
Vacca F, Amadio S, Sancesario G, Bernardi G, Volonte C (2004) P2X3 receptor localizes into lipid rafts in neuronal cells. J Neurosci Res 76:653–661
Keller P, Simons K (1998) Cholesterol is required for surface transport of influenza virus hemagglutinin. J Cell Biol 140:1357–1367
Tsui-Pierchala BA, Encinas M, Milbrandt J, Johnson EM Jr. (2002) Lipid rafts in neuronal signaling and function. Trends Neurosci 25:412–417
Eriksson J, Bongenhielm U, Kidd E, Matthews B, Fried K (1998) Distribution of P2X3 receptors in the rat trigeminal ganglion after inferior alveolar nerve injury. Neurosci Lett 254:37–40
Llewellyn-Smith IJ, Burnstock G (1998) Ultrastructural localization of P2X3 receptors in rat sensory neurons. Neuroreport 9:2545–2550
Virginio C, North RA, Surprenant A (1998) Calcium permeability and block at homomeric and heteromeric P2X2 and P2X3 receptors, and P2X receptors in rat nodose neurones. J Physiol 510(Pt 1):27–35
Thomas S, Virginio C, North RA, Surprenant A (1998) The antagonist trinitrophenyl-ATP reveals co-existence of distinct P2X receptor channels in rat nodose neurones. J Physiol 509(Pt 2):411–417
Krishtal O, Lozovaya N, Fedorenko A, Savelyev I, Chizhmakov I (2006) The agonists for nociceptors are ubiquitous, but the modulators are specific: P2X receptors in the sensory neurons are modulated by cannabinoids. Pflugers Arch 453:353–360
Ruan HZ, Moules E, Burnstock G (2004) Changes in P2X3 purinoceptors in sensory ganglia of the mouse during embryonic and postnatal development. Histochem Cell Biol 122:539–551
Petruska JC, Cooper BY, Johnson RD, Gu JG (2000) Distribution patterns of different P2x receptor phenotypes in acutely dissociated dorsal root ganglion neurons of adult rats. Exp Brain Res 134:126–132
Grubb BD, Evans RJ (1999) Characterization of cultured dorsal root ganglion neuron P2X receptors. Eur J Neurosci 11:149–154
Zhong Y, Dunn PM, Bardini M, Ford AP, Cockayne DA, Burnstock G (2001) Changes in P2X receptor responses of sensory neurons from P2X3-deficient mice. Eur J Neurosci 14:1784–1792
Cockayne DA, Dunn PM, Zhong Y, Rong W, Hamilton SG, Knight GE, Ruan HZ, Ma B, Yip P, Nunn P, McMahon SB, Burnstock G, Ford AP (2005) P2X2 knockout mice and P2X2/P2X3 double knockout mice reveal a role for the P2X2 receptor subunit in mediating multiple sensory effects of ATP. J Physiol 567:621–639
Jahr CE, Jessell TM (1983) ATP excites a subpopulation of rat dorsal horn neurones. Nature 304:730–733
Li J, Perl ER (1995) ATP modulation of synaptic transmission in the spinal substantia gelatinosa. J Neurosci 15:3357–3365
Shiokawa H, Nakatsuka T, Furue H, Tsuda M, Katafuchi T, Inoue K, Yoshimura M (2006) Direct excitation of deep dorsal horn neurones in the rat spinal cord by the activation of postsynaptic P2X receptors. J Physiol 573:753–763
Collo G, Neidhart S, Kawashima E, Kosco-Vilbois M, North RA, Buell G (1997) Tissue distribution of the P2X7 receptor. Neuropharmacology 36:1277–1283
Vulchanova L, Arvidsson U, Riedl M, Wang J, Buell G, Surprenant A, North RA, Elde R (1996) Differential distribution of two ATP-gated channels (P2X receptors) determined by immunocytochemistry. Proc Natl Acad Sci U S A 93:8063–8067
Gu JG (2003) P2X receptor-mediated modulation of sensory transmission to the spinal cord dorsal horn. Neuroscientist 9:370–378
Chen M, Gu JG (2005) A P2X receptor-mediated nociceptive afferent pathway to lamina I of the spinal cord. Mol Pain 1:4
Vulchanova L, Riedl MS, Shuster SJ, Stone LS, Hargreaves KM, Buell G, Surprenant A, North RA, Elde R (1998) P2X3 is expressed by DRG neurons that terminate in inner lamina II. Eur J Neurosci 10:3470–3478
Nakatsuka T, Furue H, Yoshimura M, Gu JG (2002) Activation of central terminal vanilloid receptor-1 receptors and alpha beta-methylene-ATP-sensitive P2X receptors reveals a converged synaptic activity onto the deep dorsal horn neurons of the spinal cord. J Neurosci 22;1228–1237
Tsuda M, Shigemoto-Mogami Y, Koizumi S, Mizokoshi A, Kohsaka S, Salter MW, Inoue K (2003) P2X4 receptors induced in spinal microglia gate tactile allodynia after nerve injury. Nature 424:778–783
Inoue K (2006) ATP receptors of microglia involved in pain. Novartis Found Symp 276:263–272
Okada M, Nakagawa T, Minami M, Satoh M (2002) Analgesic effects of intrathecal administration of P2Y nucleotide receptor agonists UTP and UDP in normal and neuropathic pain model rats. J Pharmacol Exp Ther 303:66–73
Gerevich Z, Borvendeg SJ, Schroder W, Franke H, Wirkner K, Norenberg W, Furst S, Gillen C, Illes P (2004) Inhibition of N-type voltage-activated calcium channels in rat dorsal root ganglion neurons by P2Y receptors is a possible mechanism of ADP-induced analgesia. J Neurosci 24;797–807
Gerevich Z, Illes P (2004) P2Y receptors and pain transmission. Purinergic Signalling 1:3–10
Kobayashi K, Fukuoka T, Yamanaka H, Dai Y, Obata K, Tokunaga A, Noguchi K (2006) Neurons and glial cells differentially express P2Y receptor MRNAs in the rat dorsal root ganglion and spinal cord. J Comp Neurol 498:443–454
Stucky CL, Medler KA, Molliver DC (2004) The P2Y agonist UTP activates cutaneous afferent fibers. Pain 109:36–44
Yoshida K, Nakagawa T, Kaneko S, Akaike A, Satoh M (2002) Adenosine 5′-triphosphate inhibits slow depolarization induced by repetitive dorsal root stimulation via P2Y purinoceptors in substantia gelatinosa neurons of the adult rat spinal cord slices with the dorsal root attached. Neurosci Lett 320:121–124
Alexander K, Niforatos W, Bianchi B, Burgard EC, Lynch KJ, Kowaluk EA, Jarvis MF, Van BT (1999) Allosteric modulation and accelerated resensitization of human P2X(3) receptors by Cibacron blue. J Pharmacol Exp Ther 291:1135–1142
Lewis CJ, Surprenant A, Evans RJ (1998) 2′,3′-O-(2,4,6-trinitrophenyl) adenosine 5′-triphosphate (TNP-ATP)—a nanomolar affinity antagonist at rat mesenteric artery P2X receptor ion channels. Br J Pharmacol 124:1463–1466
Hamilton SG, Warburton J, Bhattacharjee A, Ward J, McMahon SB (2000) ATP in human skin elicits a dose-related pain response which is potentiated under conditions of hyperalgesia. Brain 123(Pt 6):1238–1246
Sokolova E, Skorinkin A, Moiseev I, Agrachev A, Nistri A, Giniatullin R (2006) Experimental and modeling studies of desensitization of P2X3 receptors. Mol Pharmacol 70:373–382
Phillis JW, O’Regan MH, Perkins LM (1993) Adenosine 5′-triphosphate release from the normoxic and hypoxic in vivo rat cerebral cortex. Neurosci Lett 151:94–96
Kuzmin AI, Lakomkin VL, Kapelko VI, Vassort G (1998) Interstitial ATP level and degradation in control and postmyocardial infarcted rats. Am J Physiol 275:C766–C771
Tsuda M, Shigemoto-Mogami Y, Ueno S, Koizumi S, Ueda H, Iwanaga T, Inoue K (2002) Downregulation of P2X3 receptor-dependent sensory functions in A/J inbred mouse strain. Eur J Neurosci 15:1444–1450
Jarvis MF, Burgard EC, McGaraughty S, Honore P, Lynch K, Brennan TJ, Subieta A, Van BT, Cartmell J, Bianchi B, Niforatos W, Kage K, Yu H, Mikusa J, Wismer CT, Zhu CZ, Chu K, Lee CH, Stewart AO, Polakowski J, Cox BF, Kowaluk E, Williams M, Sullivan J, Faltynek C (2002) A-317491, a novel potent and selective non-nucleotide antagonist of P2X3 and P2X2/3 receptors, reduces chronic inflammatory and neuropathic pain in the rat. Proc Natl Acad Sci U S A 99:17179–17184
McGaraughty S, Jarvis MF (2005) Antinociceptive properties of a non-nucleotide P2X3/P2X2/3 receptor antagonist. Drug News Perspect 18:501–507
Liang SD, Gao Y, Xu CS, Xu BH, Mu SN(2004) Effect of tetramethylpyrazine on acute nociception mediated by signaling of P2X receptor activation in rat. Brain Res 995:247–252
Barclay J, Patel S, Dorn G, Wotherspoon G, Moffatt S, Eunson L, Abdel’al S, Natt F, Hall J, Winter J, Bevan S, Wishart W, Fox A, Ganju P (2002) Functional downregulation of P2X3 receptor subunit in rat sensory neurons reveals a significant role in chronic neuropathic and inflammatory pain. J Neurosci 22:8139–8147
Tjølsen A, Berge OG, Hunskaar S, Rosland JH, Hole K (1992) The formalin test, an evaluation of the method. Pain 51:5–17
Sawynok J, Reid A (1997) Peripheral adenosine 5′-triphosphate enhances nociception in the formalin test via activation of a purinergic P2X receptor. Eur J Pharmacol 330:115–121
Jarvis MF, Wismer CT, Schweitzer E, Yu H, Van BT, Lynch KJ, Burgard EC, Kowaluk EA (2001) Modulation of BzATP and induced nociception: attenuation by the P2X receptor antagonist, TNP-ATP and enhancement by the P2X(3) allosteric modulator, Cibacron blue. Br J Pharmacol 132:259–269
Tsuda M, Ueno S, Inoue K (1999) Evidence for the involvement of spinal endogenous ATP and P2X receptors in nociceptive responses caused by formalin and capsaicin in mice. Br J Pharmacol 128:1497–1504
Tsuda M, Ueno S, Inoue K (1999) In vivo pathway of thermal hyperalgesia by intrathecal administration of alpha,beta-methylene ATP in mouse spinal cord: involvement of the glutamate-NMDA receptor system. Br J Pharmacol 127:449–456
Nakatsuka T, Gu JG (2001) ATP P2X receptor-mediated enhancement of glutamate release and evoked EPSCs in dorsal horn neurons of the rat spinal cord. J Neurosci 21:6522–6531
Nakatsuka T, Tsuzuki K, Ling JX, Sonobe H, Gu JG (2003) Distinct roles of P2X receptors in modulating glutamate release at different primary sensory synapses in rat spinal cord. J Neurophysiol 89:3243–3252
Wismer CT, Faltynek CR, Jarvis MF, McGaraughty S (2003) Distinct neurochemical mechanisms are activated following administration of different P2X receptor agonists into the hindpaw of a rat. Brain Res 965:187–193
Hamilton SG, Wade A, McMahon SB (1999) The effects of inflammation and inflammatory mediators on nociceptive behaviour induced by ATP analogues in the rat. Br J Pharmacol 126:326–332
Gordon JL (1986) Extracellular ATP: effects, sources and fate. Biochem J 233:309–319
Verghese MW, Kneisler TB, Boucheron JA (1996) P2U agonists induce chemotaxis and actin polymerization in human neutrophils and differentiated HL60 cells. J Biol Chem 271:15597–15601
Bodin P, Burnstock G (1998) Increased release of ATP from endothelial cells during acute inflammation. Inflamm Res 47:351–354
Bours MJ, Swennen EL, Di Virgilio F, Cronstein BN, Dagnelie PC (2006) Adenosine 5′-triphosphate and adenosine as endogenous signaling molecules in immunity and inflammation. Pharmacol Ther 112:358–404
Bleehen T, Hobbiger F, Keele CA (1976) Identification of algogenic substances in human erythrocytes. J Physiol 262:131–149
Reeh PW, Steen KH (1996) Tissue acidosis in nociception and pain. Prog Brain Res 113:143–151
Zimmermann K, Reeh PW, Averbeck B (2002) ATP can enhance the proton-induced CGRP release through P2Y receptors and secondary PGE(2) release in isolated rat dura mater. Pain 97:259–265
King BF, Wildman SS, Ziganshina LE, Pintor J, Burnstock G (1997) Effects of extracellular pH on agonism and antagonism at a recombinant P2X2 receptor. Br J Pharmacol 121:1445–1453
Nakazawa K, Liu M, Inoue K, Ohno Y (1997) pH dependence of facilitation by neurotransmitters and divalent cations of P2X2 purinoceptor/channels. Eur J Pharmacol 337:309–314
Xu GY, Huang LY (2002) Peripheral inflammation sensitizes P2X receptor-mediated responses in rat dorsal root ganglion neurons. J Neurosci 22:93–102
Ambalavanar R, Moritani M, Dessem D (2005) Trigeminal P2X3 receptor expression differs from dorsal root ganglion and is modulated by deep tissue inflammation. Pain 117:80–291
Ambalavanar R, Moritani M, Moutanni A, Gangula P, Yallampalli C, Dessem D (2006) Deep tissue inflammation upregulates neuropeptides and evokes nociceptive behaviors which are modulated by a neuropeptide antagonist. Pain 120:53–68
Fabbretti E, D’Arco M, Fabbro A, Simonetti M, Nistri A, Giniatullin R (2006) Delayed upregulation of ATP P2X3 receptors of trigeminal sensory neurons by calcitonin gene-related peptide. J Neurosci 26:6163–6171
Driessen B, Reimann W, Selve N, Friderichs E, Bultmann R (1994) Antinociceptive effect of intrathecally administered P2-purinoceptor antagonists in rats. Brain Res 666:182–188
Stanfa LC, Kontinen VK, Dickenson AH (2000) Effects of spinally administered P2X receptor agonists and antagonists on the responses of dorsal horn neurones recorded in normal, carrageenan-inflamed and neuropathic rats. Br J Pharmacol 129:351–359
Shinoda M, Ozaki N, Asai H, Nagamine K, Sugiura Y (2005) Changes in P2X3 receptor expression in the trigeminal ganglion following monoarthritis of the temporomandibular joint in rats. Pain 116:42–51
Dai Y, Fukuoka T, Wang H, Yamanaka H, Obata K, Tokunaga A, Noguchi K (2004) Contribution of sensitized P2X receptors in inflamed tissue to the mechanical hypersensitivity revealed by phosphorylated ERK in DRG neurons. Pain 108:258–266
Hamilton SG, McMahon SB (2000) ATP as a peripheral mediator of pain. J Auton Nerv Syst 81:187–194
Dowd E, McQueen DS, Chessell IP, Humphrey PP (1998) P2X receptor-mediated excitation of nociceptive afferents in the normal and arthritic rat knee joint. Br J Pharmacol 125:341–346
Honore P, Kage K, Mikusa J, Watt AT, Johnston JF, Wyatt JR, Faltynek CR, Jarvis MF, Lynch K (2002) Analgesic profile of intrathecal P2X(3) antisense oligonucleotide treatment in chronic inflammatory and neuropathic pain states in rats. Pain 99:11–19
Dell’Antonio G, Quattrini A, Cin ED, Fulgenzi A, Ferrero ME (2002) Relief of inflammatory pain in rats by local use of the selective P2X7 ATP receptor inhibitor, oxidized ATP. Arthritis Rheum 46:3378–3385
Dell’Antonio G, Quattrini A, Dal CE, Fulgenzi A, Ferrero ME (2002) Antinociceptive effect of a new P(2Z)/P2X7 antagonist, oxidized ATP, in arthritic rats. Neurosci Lett 327:87–90
Labasi JM, Petrushova N, Donovan C, McCurdy S, Lira P, Payette MM, Brissette W, Wicks JR, Audoly L, Gabel CA (2002) Absence of the P2X7 receptor alters leukocyte function and attenuates an inflammatory response. J Immunol 168:6436–6445
Woolf CJ, Ma QP, Allchorne A, Poole S (1996) Peripheral cell types contributing to the hyperalgesic action of nerve growth factor in inflammation. J Neurosci 16:2716–2723
Woolf CJ, Allchorne A, Safieh-Garabedian B, Poole S (1997) Cytokines, nerve growth factor and inflammatory hyperalgesia: the contribution of tumour necrosis factor alpha. Br J Pharmacol 121:417–424
Samad TA, Moore KA, Sapirstein A, Billet S, Allchorne A, Poole S, Bonventre JV, Woolf CJ (2001) Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory pain hypersensitivity. Nature 410:471–475
Sawynok J (2006) Adenosine and ATP receptors. Handb Exp Pharmacol 177:309–328
Ferrari D, Chiozzi P, Falzoni S, Dal SM, Collo G, Buell G, DiVirgilio F (1997) ATP-mediated cytotoxicity in microglial cells. Neuropharmacology 36:1295–1301
Visentin S, Renzi M, Frank C, Greco A, Levi G (1999) Two different ionotropic receptors are activated by ATP in rat microglia. J Physiol 519:723–736
Watkins LR, Maier SF (2002) Beyond neurons: evidence that immune and glial cells contribute to pathological pain states. Physiol Rev 82:981–1011
Farber K, Kettenmann H (2005) Physiology of microglial cells. Brain Res Brain Res Rev 48:133–143
Paukert M, Osteroth R, Geisler HS, Brandle U, Glowatzki E, Ruppersberg JP, Grunder S (2001) Inflammatory mediators potentiate ATP-gated channels through the P2X(3) subunit. J Biol Chem 276:21077–21082
Wildman SS, King BF, Burnstock G (1997) Potentiation of ATP-responses at a recombinant P2X2 receptor by neurotransmitters and related substances. Br J Pharmacol 120:221–224
Amaya F, Wang H, Costigan M, Allchorne AJ, Hatcher JP, Egerton J, Stean T, Morissset V, Grose D, Chessell IP, Tate S, Green PJ, Woolf CJ (2006) The voltage-gated sodium channel Na(v)1.9 is an effector of peripheral inflammatory pain hypersensitivity. J Neurosci 26:12852–12860
Ji RR, Befort K, Brenner GJ, Woolf CJ (2002) ERK MAP kinase activation in superficial spinal cord neurons induces prodynorphin and NK-1 upregulation and contributes to persistent inflammatory pain hypersensitivity. J Neurosci 22:478–485
Ji RR, Samad TA, Jin SX, Schmoll R, Woolf CJ (2002) P38 MAPK activation by NGF in primary sensory neurons after inflammation increases TRPV1 levels and maintains heat hyperalgesia. Neuron 36:57–68
Ramer MS, Bradbury EJ, McMahon SB (2001) Nerve growth factor induces P2X(3) expression in sensory neurons. J Neurochem 77:864–875
King BF, Liu M, Pintor J, Gualix J, Miras-Portugal MT, Burnstock G (1999) Diinosine pentaphosphate (IP5I) is a potent antagonist at recombinant rat P2X1 receptors. Br J Pharmacol 128:981–988
Dery O, Corvera CU, Steinhoff M, Bunnett NW (1998) Proteinase-activated receptors, novel mechanisms of signaling by serine proteases. Am J Physiol 274:C1429–C1452
Steinhoff M, Vergnolle N, Young SH, Tognetto M, Amadesi S, Ennes HS, Trevisani M, Hollenberg MD, Wallace JL, Caughey GH, Mitchell SE, Williams LM, Geppetti P, Mayer EA, Bunnett NW (2000) Agonists of proteinase-activated receptor 2 induce inflammation by a neurogenic mechanism. Nat Med 6:151–158
Zhu WJ, Dai Y, Fukuoka T, Yamanaka H, Kobayashi K, Obata K, Wang S, Noguchi K (2006) Agonist of proteinase-activated receptor 2 increases painful behavior produced by alpha, beta-methylene adenosine 5′-triphosphate. Neuroreport 17:1257–1261
Shimizu I, Iida T, Guan Y, Zhao C, Raja SN, Jarvis MF, Cockayne DA, Caterina MJ (2005) Enhanced thermal avoidance in mice lacking the ATP receptor P2X3. Pain 116:96–108
Fukui M, Takishita A, Zhang N, Nakagawa T, Minami M, Satoh M (2004) Involvement of locus coeruleus noradrenergic neurons in supraspinal antinociception by alpha,beta-methylene-ATP in rats. J Pharmacol Sci 94:153–160
Fukui M, Nakagawa T, Minami M, Satoh M, Kaneko S (2006) Inhibitory role of supraspinal P2X3/P2X2/3 subtypes on nociception in rats. Mol Pain 2:19
Baron R (2006) Mechanisms of disease: neuropathic pain—a clinical perspective. Nat Clin Pract Neurol 2:95–106
Chen Y, Shu Y, Zhao Z (1999) Ectopic purinergic sensitivity develops at sites of chronic nerve constriction injury in rat. Neuroreport 10:2779–2782
Park SK, Chung K, Chung JM (2000) Effects of purinergic and adrenergic antagonists in a rat model of painful peripheral neuropathy. Pain 87:171–179
Chen Y, Li GW, Wang C, Gu Y, Huang LY (2005) Mechanisms underlying enhanced P2X receptor-mediated responses in the neuropathic pain state. Pain 119:38–48
Novakovic SD, Kassotakis LC, Oglesby IB, Smith JA, Eglen RM, Ford AP, Hunter JC (1999) Immunocytochemical localization of P2X3 purinoceptors in sensory neurons in naive rats and following neuropathic injury. Pain 80:273–282
Tsuzuki K, Kondo E, Fukuoka T, Yi D, Tsujino H, Sakagami M, Noguchi K (2001) Differential regulation of P2X(3) MRNA expression by peripheral nerve injury in intact and injured neurons in the rat sensory ganglia. Pain 91:351–360
Kage K, Niforatos W, Zhu CZ, Lynch KJ, Honore P, Jarvis MF (2002) Alteration of dorsal root ganglion P2X3 receptor expression and function following spinal nerve ligation in the rat. Exp Brain Res 147:511–519
Yiangou Y, Facer P, Birch R, Sangameswaran L, Eglen R, Anand P (2000) P2X3 receptor in injured human sensory neurons. Neuroreport 11:993–996
Dorn G, Patel S, Wotherspoon G, Hemmings-Mieszczak M, Barclay J, Natt FJ, Martin P, Bevan S, Fox A, Ganju P, Wishart W, Hall J (2004) SiRNA relieves chronic neuropathic pain. Nucleic Acids Res 32:e49
Sharp CJ, Reeve AJ, Collins SD, Martindale JC, Summerfield SG, Sargent BS, Bate ST, Chessell IP (2006) Investigation into the role of P2X(3)/P2X(2/3) receptors in neuropathic pain following chronic constriction injury in the rat: an electrophysiological study. Br J Pharmacol 148:845–852
Seltzer Z, Dubner R, Shir Y (1990) A novel behavioral model of neuropathic pain disorders produced in rats by partial sciatic nerve injury. Pain 43:205–218
Dowman R, Darcey T, Barkan H, Thadani V, Roberts D (2007) Human intracranially-recorded cortical responses evoked by painful electrical stimulation of the sural nerve. Neuroimage 34:743–763
Schwab JM, Guo L, Schluesener HJ (2005) Spinal cord injury induces early and persistent lesional P2X4 receptor expression. J Neuroimmunol 163:185–189
Rabchevsky AG, Degos JD, Dreyfus PA (1999) Peripheral injections of Freund’s adjuvant in mice provoke leakage of serum proteins through the blood–brain barrier without inducing reactive gliosis. Brain Res 832:84–96
Burnstock G, Satchell DG, Smythe A (1972) A comparison of the excitatory and inhibitory effects of non-adrenergic, non-cholinergic nerve stimulation and exogenously applied ATP on a variety of smooth muscle preparations from different vertebrate species. Br J Pharmacol 46:234–242
Birder LA, Kanai AJ, de Groat WC, Kiss S, Nealen ML, Burke NE, Dineley KE, Watkins S, Reynolds IJ, Caterina MJ (2001) Vanilloid receptor expression suggests a sensory role for urinary bladder epithelial cells. Proc Natl Acad Sci U S A 98;13396–13401
Cervero F, Laird JM (2004) Understanding the signaling and transmission of visceral nociceptive events. J Neurobiol 61:45–54
Namasivayam S, Eardley I, Morrison JF (1999) Purinergic sensory neurotransmission in the urinary bladder: an in vitro study in the rat. BJU Int 84:854–860
Studeny S, Torabi A, Vizzard MA (2005) P2X2 and P2X3 receptor expression in postnatal and adult rat urinary bladder and lumbosacral spinal cord. Am J Physiol Regul Integr Comp Physiol 289:R1155–R1168
Vlaskovska M, Kasakov L, Rong W, Bodin P, Bardini M, Cockayne DA, Ford AP, Burnstock G (2001) P2X3 knock-out mice reveal a major sensory role for urothelially released ATP. J Neurosci 21:5670–5677
Tempest HV, Dixon AK, Turner WH, Elneil S, Sellers LA, Ferguson DR (2004) P2X and P2X receptor expression in human bladder urothelium and changes in interstitial cystitis. BJU Int 93:1344–1348
Sun Y, Chai TC (2004) Up-regulation of P2X3 receptor during stretch of bladder urothelial cells from patients with interstitial cystitis. J Urol 171:448–452
Borvendeg SJ, Al-Khrasani M, Rubini P, Fischer W, Allgaier C, Wirkner K, Himmel HM, Gillen C, Illes P (2003) Subsensitivity of P2X but not vanilloid 1 receptors in dorsal root ganglia of rats caused by cyclophosphamide cystitis. Eur J Pharmacol 474:71–75
Poole DP, Castelucci P, Robbins HL, Chiocchetti R, Furness JB (2002) The distribution of P2X3 purine receptor subunits in the guinea pig enteric nervous system. Auton Neurosci 101:39–47
Robinson DR, McNaughton PA, Evans ML, Hicks GA (2004) Characterization of the primary spinal afferent innervation of the mouse colon using retrograde labelling. Neurogastroenterol Motil 16:113–124
Camilleri M (2001) Pathophysiology in irritable bowel syndrome. Drug News Perspect 14:268–278
Yiangou Y, Facer P, Baecker PA, Ford AP, Knowles CH, Chan CL, Williams NS, Anand P (2001) ATP-gated ion channel P2X(3) is increased in human inflammatory bowel disease. Neurogastroenterol Motil 13:365–369
Kirkup AJ, Booth CE, Chessell IP, Humphrey PP, Grundy D (1999) Excitatory effect of P2X receptor activation on mesenteric afferent nerves in the anaesthetised rat. J Physiol 520:551–563
Wynn G, Rong W, Xiang Z, Burnstock G (2003) Purinergic mechanisms contribute to mechanosensory transduction in the rat colorectum. Gastroenterology 125:1398–1409
Wynn G, Ma B, Ruan HZ, Burnstock G (2004) Purinergic component of mechanosensory transduction is increased in a rat model of colitis. Am J Physiol Gastrointest Liver Physiol 287:G647–G657
Page AJ, Martin CM, Blackshaw LA (2002) Vagal mechanoreceptors and chemoreceptors in mouse stomach and esophagus. Neurophysiol 87:2095–2103
Brierley SM, Carter R, Jones W, III, Xu L, Robinson DR, Hicks GA, Gebhart GF, Blackshaw LA (2005) Differential chemosensory function and receptor expression of splanchnic and pelvic colonic afferents in mice. J Physiol 567:267–281
Honore P, Mikusa J, Bianchi B, McDonald H, Cartmell J, Faltynek C, Jarvis MF (2002) TNP-ATP, a potent P2X3 receptor antagonist, blocks acetic acid-induced abdominal constriction in mice, comparison with reference analgesics. Pain 96:99–105
Durham PL (2006) Calcitonin gene-related peptide (CGRP) and migraine. Headache 46(Suppl. 1):S3–S8
Juhasz G, Zsombok T, Jakab B, Nemeth J, Szolcsanyi J, Bagdy G (2005) Sumatriptan causes parallel decrease in plasma calcitonin gene-related peptide (CGRP) concentration and migraine headache during nitroglycerin induced migraine attack. Cephalalgia 25:179–183
Natura G, von Banchet GS, Schaible HG (2005) Calcitonin gene-related peptide enhances TTX-resistant sodium currents in cultured dorsal root ganglion neurons from adult rats. Pain 116:194–204
White N, Burnstock G (2006) P2 receptors and cancer. Trends Pharmacol Sci 27:211–217
Maehara Y, Kusumoto H, Anai H, Kusumoto T, Sugimachi K (1987) Human tumor tissues have higher ATP contents than normal tissues. Clin Chim Acta 169:341–343
Dang K, Bielfeldt K, Lamb K, Gebhart GF (2005) Gastric ulcers evoke hyperexcitability and enhance P2X receptor function in rat gastric sensory neurons. J Neurophysiol 93:3112–3119
Cain DM, Wacnik PW, Eikmeier L, Beitz A, Wilcox GL, Simone DA (2001) Functional interactions between tumor and peripheral nerve in a model of cancer pain in the mouse. Pain Med 2:15–23
Gilchrist LS, Cain DM, Harding-Rose C, Kov AN, Wendelschafer-Crabb G, Kennedy WR, Simone DA (2005) Re-organization of P2X3 receptor localization on epidermal nerve fibers in a murine model of cancer pain. Brain Res 1044:197–205
Kennedy WR, Wendelschafer-Crabb G (1999) Utility of the skin biopsy method in studies of diabetic neuropathy. Electroencephalogr Clin Neurophysiol Suppl 50:553–559
Nagamine K, Ozaki N, Shinoda M, Asai H, Nishiguchi H, Mitsudo K, Tohnai I, Ueda M, Sugiura Y (2006) Mechanical allodynia and thermal hyperalgesia induced by experimental squamous cell carcinoma of the lower gingiva in rats. J Pain 7:659–670
Rong W, Burnstock G, Spyer KM (2000) P2X purinoceptor-mediated excitation of trigeminal lingual nerve terminals in an in vitro intra-arterially perfused rat tongue preparation. J Physiol 524:891–902
Jones CA, Vial C, Sellers LA, Humphrey PPA, Evans RJ, Chessell IP (2004) Functional regulation of P2X6 receptors by n-linked glycosylation: identification of a novel αβ-methylene ATP-sensitive phenotype. Mol Pharmacol 65:979–985
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wirkner, K., Sperlagh, B. & Illes, P. P2X3 Receptor Involvement in Pain States. Mol Neurobiol 36, 165–183 (2007). https://doi.org/10.1007/s12035-007-0033-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-007-0033-y