
Abstract
Acquired or secondary hemophagocytic lymphohistiocytosis (sHLH) is a life-threatening hyperinflammation syndrome caused mostly by various infectious agents, autoimmune disorders or malignancy. So far, only anecdotal cases of sHLH associated with multiple myeloma have been published. We provide a review of all these reports and include a previously not published case of myeloma-associated sHLH in a 59-year-old male with complex partial epilepsy. Due to aggressive course of sHLH, increased awareness is indicated in all patients with malignancies which develop unremitting fever, cytopenia and splenomegaly. Early diagnosis and immediate introduction of adequate therapy is crucial for the outcome of HLH.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hemophagocytic lymphohistiocytosis (HLH), also called hemophagocytic syndrome (HPS), is a rare but aggressive and potentially life-threatening disorder. HLH was first described by Farquhar and Claireaux in 1952 [1] but remained a mysterious disease until recently. HLH occurs in two distinct forms: an inherited, familial form [2] and an acquired, secondary form [3]. The primary, autosomal recessive, familial hemophagocytic lymphohistiocytosis (FHL) usually arises in infants and has an estimated incidence of 1.2 children per million per year or 1:50,000 live-born children [4]. Secondary HLH (sHLH) can develop at any age, from children to the elderly, as a result of strong immunological activation due to severe infection (e.g. viral, bacterial, fungal, parasitic), autoimmune inflammatory disorder (e.g. SLE, rheumatoid arthritis), malignancy (acute lymphoblastic leukemia, T/NK-cell leukemia, Hodgkin and non-Hodgkin’s lymphomas, multiple myeloma (MM), acute myelogenous leukemia, myelodysplastic syndromes, melanoma, hepatocellular carcinoma, thymoma, germ cell tumor), or immune suppression/organ transplantation [3–8]. There is no exact data on the incidence of HLH in adults. A recent retrospective study of Ishii et al. [9] revealed an annual incidence of all types of HLH and in all age-groups of Japanese patients as 1 case in 800,000 per year. The most frequent form was infection-associated HLH (predominantly EBV-associated HLH), followed by lymphoma-associated HLH. The reported 5-year overall survival was highest in EBV- or other infection-associated HLH (>80%) and in autoimmune-associated HLH (almost 90%), intermediate in FHL or B-cell lymphoma–associated HLH (50%) and lowest in T/NK-cell lymphoma–associated HLH (<15%). However, it should be emphasized that the incidence of sHLH among adults probably is underestimated, due to diagnostic difficulties and overlooking or misdiagnosing of some sHLH cases.
Pathogenesis and clinical picture of HLH
HLH is not a single disease, but a clinical syndrome that can develop in association with a variety of triggers leading to the same characteristic hyperinflammatory phenotype [5]. Pathogenesis of HLH is not completely understood. It has been proposed that the clinical presentation of HLH is caused by an uncontrolled T-cell and macrophage stimulation, leading to a massive release of various pro-inflammatory mediators such as TNF-α (tumor necrosis factor α), interleukin(IL)-6, IL-8, IL-10, IL-12, IL-18, interferon γ, macrophage inflammatory protein (MIP 1-α) and hematopoietic growth factors from these cells [6, 9, 10]. The uncontrolled activation of immune cells is probably due to immune response triggered by different stimulants (infectious organisms, toxins, stress, tissue damage, metabolic products, etc.), and the underlying immune defect, inherited (mutations in genes PFR1/perforin/, UNC13D or STX11) or acquired (cytotoxic therapy, transplantation), may be a crucial factor in the development of HLH [5, 6].
The most typical signs of HLH are fever and hepatosplenomegaly associated with pancytopenia, neurological symptoms, skin rash, lymphadenopathy, jaundice and edema [4, 11, 12]. Laboratory findings include hypertriglyceridemia, hypofibrinogenemia, hyperferritinemia, coagulopathy, liver function test abnormalities such as elevated transaminases and bilirubin [2, 4, 12, 13]. Histopathological examination reveals accumulation of lymphocytes and histiocytes (macrophages), sometimes with hemophagocytic activity, observed in the spleen, bone marrow (BM), liver, lymph nodes and cerebrospinal fluid [11, 13]. Other typical findings in HLH are low natural killer (NK) cell activity and high levels of soluble interleukin-2 receptor (sIL-2r or sCD25) in serum and CSF.
In 1991, the HLH Study Group of the Histiocyte Society published the first diagnostic guidelines for HLH which were updated in 2004. According to the current guidelines (HLH-2004), five of the eight criteria must be fulfilled to diagnose HLH [13]. These criteria are 1/fever, 2/splenomegaly, 3/cytopenia affecting two or three lineages (Hb < 90 g/l; PLT < 100 × 109/l; neutrophils <1.0 × 109/l), 4/hypertriglyceridemia (>3.0 mmol/l) and/or hypofibrinogenemia (<1.5 g/l), 5/hemophagocytosis in BM, spleen, or lymph nodes, 6/hyperferritinemia (>500 μg/l), 7/low or absent NK-cell activity, 8/elevated level of sIL-2r (sCD25) > 2400 U/ml.
Case presentation
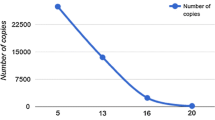
Our own experience with myeloma-associated HLH is based on the case of 59-year-old Swedish male with complex partial epilepsy (following meningitis in childhood) on antiepileptic triple therapy (carbamazepine, phenytoin, topiramate), who was diagnosed with IgG-κ MM, stage III A. He received two courses of cyclophosphamide (750 mg/m² i.v., day 1) and prednisone (250 mg/day p.o., days 1–4, 9–12); cyclophosphamide was 25% dose-reduced due to interaction with phenytoin. Stable disease (SD) status was obtained with 24% reduction of M-protein. High-dose therapy with melphalan 200 mg/m² and autologous peripheral stem cell transplantation (APSCT) was performed; the course after APSCT was unremarkable, apart from one epileptic attack on day +1; he was discharged from the hospital 2 weeks after APSCT. Two months after APSCT, 52% reduction of M-protein was present and the disease status was qualified as partial response (PR). On day +100, he complained of fatigue, M-protein was unchanged but Hb decreased to 104 g/l. Three weeks later (128 days after APSCT), he was admitted with a 2-day history of high fever (40ºC), general weakness and effort dyspnoea. Laboratory investigations showed Hb 64 g/l, WBC 8.78 × 109/l, PLT 34 × 109/l, CRP 263 mg/l, creatinine 109 μmol/l. Serum carbamazepine and phenytoin levels were both below the reference range. Treatment with antibiotics and antifungal agents was initiated. Two days later, the patient deteriorated and developed acute respiratory and renal failure; his thrombocytopenia worsened (PLT 9 × 109/l). Cultures failed to reveal any bacteria or fungi. EBV, CMV, HSV and Pneumocystis tests were negative. Unfortunately, creatinine increased to 513 μmol/l, and dialysis was started. On day 10 after admission, sHLH was suspected and BM aspiration was performed. It revealed the presence of 3% macrophages showing hemophagocytosis (Fig. 1) and only 1% plasma cells. The diagnosis of sHLH was established based on the presence of five out of eight diagnostic criteria (fever, anemia and thrombocytopenia, hemophagocytosis in the BM, hypertriglyceridemia/triglycerides 6.1 mmol/l, normal range 0.5–2.6/, hyperferritinemia/ferritin 8481 μg/l, normal range 20–300/), but two further criteria, NK-cell activity test and level of sIL-2r (sCD25), were not tested. Treatment with IVIG, corticosteroids and etoposide 150 mg/m² i.v. twice weekly was attempted starting from day 11 of hospitalization. Five days after initiating the etoposide treatment (day 16 of hospitalization), the patient developed an epileptic seizure. Computed tomography revealed bilateral subarachnoid hemorrhage in the frontal lobes. Further deterioration occurred shortly afterward, and the patient deceased 2 days later, 18 days after admission to the hospital.

May-Grünwald-Giemsa stain of the bone marrow aspirate smears (×1000). Centrally placed macrophage shows intense hemophagocytosis of erythrocytes and erythroblasts
The patient probably developed HLH already 3 months after APSCT (with unclear anemia as the first HLH symptom). Three weeks later, a fulminant sHLH developed where extensive diagnostic investigations failed to reveal any underlying infectious agent. Despite quite early (12 days from fever onset) diagnosis of HLH and immediate introduction of a wide spectrum of HLH therapy, the outcome was poor and the patient died. To our knowledge, this is the first published case of sHLH probably associated with both MM and anticonvulsants and the second reported case of sHLH after APSCT for myeloma.
Myeloma-associated HLH
Myeloma-associated hemophagocytic lymphohistiocytosis is a form of malignancy-associated sHLH which can occur before or during the treatment of the known malignancy, or as a first manifestation of unknown malignancy [3]. HLH has previously rarely been reported to be associated with MM, and we were able to find only four such cases in the literature [14–17].
The first case of sHLH in MM was published by Kaito et al. [14]. The article is written in Japanese with the English abstract. The patient with known MM developed within a short period of time pancytopenia and liver dysfunction. BM examination revealed an increased number of mature histiocytes, and a diagnosis of HLH was made. The patient died due to multiorgan failure, despite steroid therapy. According to the authors, autopsy showed hemophagocytic activity in BM, liver, lymph nodes and kidneys. Unfortunately, important information about the patient’s sex and age, type of M-protein, MM stage at presentation, previous MM treatment, assays performed in order to exclude infection as a cause of HLH, co-morbidities, etc. is not available in English.
Venizelos et al. [15] reported in 2002 a 54-year-old female with a 6-month history of fever, in whom concomitant sHLH (fever, pancytopenia, splenomegaly, hemophagocytosis in BM) and κ light-chain MM (30% of plasma cells in BM, renal failure) co-existed at the time of MM diagnosis. No possible infectious cause of sHLH was detected. The patient received six courses of VAD (vinca alkaloid, adriamycin, dexamethasone)-type regimen for MM, but the only applied specific treatment for HLH was VAD’s dexamethasone (DXM). The patient’s HLH resolved, and she was in a good condition 2 years after the onset of VAD therapy.
A detailed case report of 54-year-old male suffering from MM and sHLH was provided by Terrovitis et al. [16]. The patient presented with a 2-month history of back pain and, on admission, irritation of the right sciatic nerve. Magnetic resonance imaging revealed an osteolytic lesion in the L1 with compression of the spinal cord. The patient underwent decompression and stabilization surgery of the spine. In the meantime, investigations showed serum M-protein of type IgG-κ (69 g/l) and 60% plasma cells in BM. VAD-type therapy in combination with thalidomide 100 mg/day p.o. was started for stage III IgG-κ MM. Ten days after initiation of VAD, the patient developed fever followed by pancytopenia, liver dysfunction and hemophagocytosis in BM. Hyperferritinemia, hypertriglyceridemia and the lack of confirmed infection of any type completed the picture of sHLH. Interestingly, symptomatic treatment with Naproxen 500 mg daily resulted in an immediate relief of the fever. HLH therapy was started 21 days after HLH onset with a favorable effect. Four months after MM presentation, the patient was alive, in PR (partial response) of his MM and without signs of HLH.
The first reported case of sHLH after APSCT for MM was published in 2006 by Ostronoff et al. [17]. A 54-year-old female with MM (M-protein’s type not reported, stage III A) achieved CR (complete response) after four courses of VAD-type therapy. She was subsequently treated with melphalan 140 mg/m² and APSCT. On day +16, she developed fever, anemia, thrombocytopenia, hypofibrinogenemia, GI bleeding and splenomegaly. Hemophagocytosis was present in BM. HLH was diagnosed, and no causative infectious agent was detected. Treatment with IVIG and DXM was started on day +21, 5 days after the HLH onset. The patient’s condition improved, and day +39 BM aspirate was free of hemophagocytosis. Longer follow-up results are not available.
Concluding remarks
The association between hematological malignancies (in particular of lymphoproliferative type) and sHLH is rare, but possible and described within a wide range of entities [3, 8, 9, 12, 13]. So far, five cases (including this report) of myeloma-associated HLH were published in the literature [14–17]. Nevertheless, all of these MM cases differ at many points, e.g. regarding the MM stage at presentation, previous treatment of MM, timing of HLH occurrence and the anti-HLH therapy administered (Table 1). It is possible that sHLH can develop via different, so far unknown, pathways resulting in different therapy response and outcome. Two of the published HLH cases with MM may be due to the advanced malignancy before [15] or shortly after the diagnosis of MM [16]. The role of immune system impaired functioning in the development of HLH in MM after APSCT has been previously proposed in one case [17]. Our patient, described in this paper, probably developed HLH already 3 months after APSCT, but local myeloma progression and, although less likely, antiepileptics could play a role (e.g. by the influence on immunological reconstitution after APSCT). This possibly could be supported by the fact that cases relating anticonvulsants to the development of HLH have been published previously [18–20]. Anticonvulsants such as phenytoin and carbamazepine may have a negative impact on immunological system. In some cases, antiepileptic medications may evoke an anticonvulsant hypersensitivity syndrome as a result of idiosyncratic immunologic reaction [21]. It has also been proved that carbamazepine-specific T cells secrete IL-5 and INF-γ and present cytotoxic activity [22].
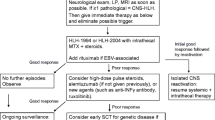
HLH should be considered in patients suffering from malignancy (including myeloma) with unremitting fever, cytopenia and/or splenomegaly. It is worth to emphasize that possibility of sHLH development exist during the whole period of cancer therapy and is not over after stem cell transplantation (both autologous and allogeneic). Management of sHLH, not only in MM, consists of early diagnosis, therapy of the triggering disease and HLH-specific treatment. The aim of such a treatment is to suppress the hyperinflammation that is leading to the life-threatening symptoms. So far, the problem of specific therapy of different HLH entities is unsolved. The treatment protocol HLH-2004 is designed for patients with all forms of HLH [13]. Initial therapy (weeks 1–8) is based on etoposide, dexamethasone and cyclosporine A. However, our own experience with the treatment of malignancy-associated HLH (M-HLH) shows that adults tolerate far lower etoposide doses (50–100 mg/m²/dose) when compared with children with FLH (unpublished data). Nevertheless, treatment protocol HLH-2004 should serve as a basis for the treatment of all HLH cases [5, 13].
HLH is a life-threatening hyperinflammatory syndrome which is difficult to diagnose and is often overlooked, especially in older children and adults [5]. Awareness of acquired HLH, its symptoms and diagnostic criteria should be mandatory among all physicians, especially those providing care to adults with hematological malignancies and/or receiving immunosuppressive treatment (e.g. chemotherapy, stem cell transplantation). The future research on sHLH needs focus on better understanding of pathways behind complex sHLH pathogenesis, recognition of better sHLH markers for diagnostics and follow-up (in malignancy-associated HLH ferritin and sIL-2r can be elevated due to malignancy), as well as more specific and effective therapies.
References
Farquhar JW, Claireaux AE. Familial haemophagocytic reticulosis. Arch Dis Child. 1952;27:519–25.
Henter J-I, Arico M, Elinder G, Imashuku S, Janka G. Familial hemophagocytic lymphohistiocytosis (primary HLH). Hematol Oncol Clin North Am. 1998;12:417–33.
Janka G, Imashuku S, Elinder G, Schneider M, Henter J-I. Infection- and malignancy-associated hemophagocytic syndromes. Hematol Oncol Clin North Am. 1998;12:435–44.
Henter J-I, Elinder G, Söder O, Öst Å. Incidence in Sweden and clinical features of familial hemophagocytic lymphohistiocytosis. Acta Paediatr Scand. 1991;80:428–35.
Janka G. Hemophagocytic lymphohistiocytosis: When the immune system runs amok. Klin Padiatr. 2009;221:278–85.
Janka GE, Schneider EM. Modern management of children with haemophagocytic lymphohistiocytosis. Br J Haematol. 2004;124:4–14.
Hasselblom S, Linde A, Ridell B. Hodgkin’s lymphoma, Epstein-Barr virus reactivation and fatal haemophagocytic syndrome. J Intern Med. 2004;255:289–95.
Machaczka M, Vaktnas J. Haemophagocytic syndrome associated with Hodgkin lymphoma and Pneumocystis jiroveci pneumonitis. Br J Haematol 2007;138:672.
Ishii E, Ohga S, Imashuku S, Yasukawa M, Tsuda H, Miura I, et al. Nationwide survey of hemophagocytic lymphohistiocytosis in Japan. Int J Hematol. 2007;86:58–65.
Henter J-I, Elinder G, Söder O, Hansson M, Andersson B, Andersson U. Hypercytokinemia in familial hemophagocytic lymphohistiocytosis. Blood. 1991;78:2918–22.
Öst Å, Nilsson-Ardnor S, Henter J-I. Autopsy findings in 27 children with haemophagocytic lymphohistiocytosis. Histopathology. 1998;32:310–6.
Reiner AP, Spivak JL. Hematophagic histiocytos. A report of 23 new patients and a review of the literature. Medicine (Baltimore). 1988;67:369–88.
Henter J-I, Horne A, Arico M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48:124–31.
Kaito K, Ono M, Kobayashi M, Kawamoto S, Nishiwaki K, Masuoka H, et al. A case of hemophagocytic syndrome with multiple myeloma. Rinsho Ketsueki. 1992;33:1095–7.
Venizelos ID, Garipidou V, Perifanis V. Hemophagocytic syndrome associated with multiple myeloma. Leuk Lymphoma. 2002;43:897–9.
Terrovitis JV, Matsouka C, Anagnostopoulos A, Anastasiou-Nana MI, Dimopoulos AM. Hemophagocytic lymphohistiocytosis after chemotherapy for multiple myeloma. Clin Lymphoma. 2004;5:194–6.
Ostronoff M, Ostronoff F, Coutinho M, Calixto R, Souto Maior AP, Sucupira A, et al. Hemophagocytic syndrome after autologous peripheral blood stem cell transplantation for multiple myeloma: successful treatment with high-dose intravenous immunoglobulin. Bone Marrow Transplant. 2006;37:797–8.
Yang YC, Jou ST, Chang YH, Liang JS, Lee WT. Hemophagocytic syndrome associated with antiepileptic drug. Pediatr Neurol. 2004;30:358–60.
Gumus H, Kumandas S, Per H, Karakukcu M. Hemophagocytic syndrome associated with high-dose lamotrigine. Pediatr Int. 2007;49:672–3.
Fukaya S, Yasuda S, Hashimoto T, Oku K, Kataoka H, Horita T, et al. Clinical features of haemophagocytis syndrome in patients with systemic autoimmune disease: analysis of 30 cases. Rheumatology. 2008;47:1686–91.
Cumbo-Nacheli G, Weinberger J, Alkhalil M, Thati N, Baptist AP. Anticonvulsant hypersensitivity syndrome: is there a role for immunomodulation? Epilepsia. 2008;49:2108–12.
Wu Y, Farrell J, Pirmohamed M, Park BK, Naisbitt DJ. Generation and characterization of antigen-specific CD4+, CD8+ and CD4+ CD8+ T-cell clones from patients with carbamazepine hypersensitivity. J Allergy Clin Immunol. 2007;119:973–81.
Acknowledgments
The authors would like to thank Dr Steven Shev for the linguistic expertise and Mrs Evalisa Larsson for the technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Machaczka, M., Vaktnäs, J., Klimkowska, M. et al. Acquired hemophagocytic lymphohistiocytosis associated with multiple myeloma. Med Oncol 28, 539–543 (2011). https://doi.org/10.1007/s12032-010-9484-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-010-9484-5