
Abstract
We sought to determine the frequency of primary extranodal lymphoma (ENL) and its characteristics in Kanagawa, a human T-cell leukemia virus type 1 (HTLV-1) nonendemic area in Japan. Subjects were 847 newly diagnosed patients with malignant lymphoma at the Yokohama City University Hospital and 8 affiliated hospitals mainly located in Kanagawa prefecture from 1999 to 2005. We compared the clinicopathological characteristics of primary ENL with primary nodal lymphoma (NL). Histological specimens were evaluated according to the World Health Organization classifications. A total of 395 (46.6%) and 452 (53.4%) patients had primary ENL and primary NL, respectively. The frequency of primary ENL increased with age. Primary extranodal sites included the gastrointestinal tract (30.4%), Waldeyer’s ring (17.8%), orbits (7.0%), soft tissue and subcutaneous tissue (5.2%), bone (4.6%), skin (4.3%), thyroid gland (4.3%), testis and prostate (3.3%), bone marrow (3.3%), nasal and paranasal cavities (2.6%), salivary glands (2.3%), lung and pleura (2.0%), breast (1.8%), central nervous system (1.0%), uterus and ovary (0.5%), and others (9.8%). Among the 395 cases of primary ENL, diffuse large B-cell lymphoma (61.2%) was most frequently diagnosed, followed by extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (13.3%) and follicular lymphoma (5.6%). The frequency of primary ENL is approximately 50% of the total lymphoma cases in Kanagawa, an HTLV-1 nonendemic area in Japan. This frequency appears to be higher than that in Western countries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Malignant lymphomas can originate from almost every organ of the body, even those organs that normally do not have lymphoid tissue. Lymphomas originating at sites other than lymph nodes and lymphoid structures are classified as primary extranodal lymphoma (ENL). Many reports describe the origin of primary ENL in various organs, while some studies have investigated clinical differences between primary nodal lymphomas (NL) and primary ENL. However, the details of primary ENL in Japanese patients have not yet been elucidated. Therefore, we studied the clinical features and frequency of ENL in Kanagawa, a human T-cell leukemia virus type 1 (HTLV-1) nonendemic area in Japan. Although chemotherapy is the standard treatment for most primary NL, some primary ENLs according to the organs or histological subtype require combined modality approaches that include chemotherapy and surgery/radiotherapy.
Materials and methods
The subjects of this study were patients newly diagnosed with malignant lymphoma from November 1999 to February 2005 at the Yokohama City University Hospital and 8 other affiliated hospitals mainly located in Kanagawa prefecture. Globally, Japan is known as the area of HTLV-1 carriers; most of these carriers reside in western parts of Japan, such as Kyushuu and Okinawa regions. Kanagawa prefecture is one of the most demographic centers after Metropolis of Tokyo; it is located in eastern Japan and is an HTLV-1 nonendemic area. The clinical stage of malignant lymphoma was defined according to the Ann Arbor classification [1]. Although the spleen, thymus, Waldeyer’s ring, and Peyer’s patches are considered as lymphoid structures, they are not lymph nodes; in this report, lymphomas originating at these sites were classified as primary ENL. All the 847 patients were completely staged according to clinical history, physical examination, chest radiographs, computed tomography from the neck to pelvis, and bone marrow aspiration and biopsy. Histological specimens were evaluated according to the World Health Organization (WHO) classification [2]. Specimens that were initially evaluated before 2001 by classifications other than the WHO classification were re-evaluated by pathologists at the affiliated hospitals according to the WHO classification. The judgment of differentiation between primary ENL and primary NL was based on the information filled by the attending physicians in our registry file. ENL was diagnosed when the largest mass was located in the extranodal organ or the onset of extranodal origin was apparent with time based on clinical history. Undetermined cases of nodal or extranodal origin were excluded from this study.
Results
From 1999 to 2005, we consecutively registered 847 patients with malignant lymphoma. Of all patients, only 1.6% patients were HTLV-1-infected carriers and adult T-cell lymphoma/leukemia patients.
The characteristics of patients at the time of diagnosis are summarized in Table 1. Of the 598 tested patients, 2 patients were HIV positive, and both of them were included in the primary NL group. Primary ENL was observed in 395 patients (46.6%). Among patients with primary ENL, male patients were 56.7%, and the median age of patients was 61 years (range 15–92 years). Patients with extranodal origin were of higher age (P < 0.001), and more likely to have elevated lactate dehydrogenase (LDH) in serum (P < 0.001); however, they were more likely to have localized stage disease (P < 0.001) than patients with primary NL. The International Prognostic Index [3] was equally distributed in the two groups. The age distribution is shown in Table 2. The frequency of primary ENL increased with age.
The presumed original organs of origin of primary ENL are listed in Table 3. The gastrointestinal (GI) tract and Waldeyer’s ring were the most frequent primary sites accounting for 30.4 and 17.8% of cases, respectively. The histological subtypes according to the primary organs are also listed in Table 3. In most organs, diffuse large B-cell lymphoma (DLBCL) was the most frequent histological subtype.
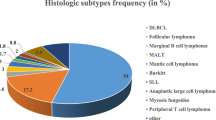
Histological subtypes of primary ENL are shown in Table 4. DLBCL was most frequently observed in 61.2% cases, followed by extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) in 13.3% cases, and follicular lymphoma (FL) in 5.6% cases. Except for MALT, extranodal origin was the most frequent in DLBCL (57.1%). In FL, extranodal origin was observed in only 14.3% of cases.
We also investigated the prognosis of the most frequent histology of primary ENL, i.e., DLBCL. Among 424 DLBCL patients, the 5-year overall survival (OS) rates for primary NL and primary ENL were 56 and 70%, respectively (Fig. 1). No significant differences were observed between the two groups. In extranodal DLBCL, we also investigated whether the primary site influenced the OS rate (Table 5). The likelihood of survival of patients with Waldeyer’s ring as the origin was particularly favorable, with a 5-year OS rate of 91% compared to patients with the other sites of origin (P = 0.006). In contrast, patients with bone marrow as the site of origin had a poor chance of survival, with a 5-year OS rate of 0%, compared to patients with the other sites of origin (P = 0.001). Histological diagnosis revealed that six of nine cases with primary bone marrow DLBCL had intravascular lymphoma, a subgroup of DLBCL known to have poor survival.

OS curves for nodal and extranodal diffuse large B-cell lymphoma patients. No significant difference was observed between the two curves
Discussion
The incidence of ENL differs greatly between countries. Approximately 25–40% of non-Hodgkin lymphoma patients present with a primary ENL in developing countries: US, 24% [4]; Canada, 27% [5]; Israel, 36% [6]; Lebanon, 44% [6]; Denmark, 37% [7]; and Holland, 41% [8]. In this study, primary ENL comprised 46.6% of all lymphomas, a greater proportion than that reported in most Western countries and slightly greater than that (42.4%) reported in a previous study on a Japanese cohort [9]. Furthermore, our data included cases of Hodgkin lymphoma, which accounts for approximately 5% of malignant lymphomas in Japan [10]. On the other hand, most of the abovementioned data from Western countries are limited to non-Hodgkin lymphoma. Since Hodgkin lymphoma with an extranodal origin is extremely rare, the inclusion of Hodgkin lymphoma cases might be expected to decrease the proportion of all subtypes of lymphoma of extranodal origin.
The definition of primary ENL is controversial. The Ann Arbor classification, which was originally formulated for Hodgkin lymphoma, does not clearly define primary NL and primary ENL. Therefore, the following two issues exist. The first is how to designate cases with involvement of both nodal and extranodal sites. This study relied on the decision of the attending physician, which was based mainly upon the site of the largest mass. We believe that this is a reasonable method to determine the origin of the lymphoma in a similar fashion to the previously reported definition of extranodal origin as no or minor nodal extranodal involvement along with a clinically dominant extranodal component [7], except for cases in which the primary site is obvious from the history of illness. In this study, cases in which the site of origin was difficult to determine were excluded. The second issue is whether to consider particular areas such as the spleen, thymus, and Waldeyer’s ring as nodal or extranodal. Indeed, including [4, 5, 8, 9, 11] or excluding [7, 12, 13] Waldeyer’s ring in the extranodal sites is controversial. Groves et al. [14] argued that primary splenic lymphoma and involvement of the spleen representing the spread of lymphoma from other sites show completely different characteristics; this suggests that primary splenic lymphoma is biologically an ENL. In this way, site-specific characteristics might be appeared in the future. For this reason, we distinguished these sites from the lymph nodes. With regard to the sites of origin in this study, the GI tract and Waldeyer’s ring accounted for 30.4 and 17.8% of primary ENL, respectively. It appears that the frequency of occurrence of primary ENL in the GI tract and Waldeyer’s ring is relatively low and high, respectively, compared to that in Western countries [4, 8].
In our series of patients, primary ENL showed the following characteristics as compared to primary NL: elderly onset, elevated LDH, and localized disease. The incidence of primary ENL increases with age. In a previous report on DLBCL, Moller et al. [12] noted that the proportion of extranodal disease was greater in elderly patients. Recently, the occurrence of malignant lymphoma, particularly primary ENL, is rapidly increasing [14, 15]. Zucca et al. commented that as a predisposing factor, increased incidence of immunosuppression due to HIV infection, other viral infections, and treatment with immunosuppressive agents might help to explain the increase in ENL [16]. Other possible causes might include environmental pollution due to pesticides and solvents [17–20]. The compromise of immune function and cumulative environmental exposure increase with age, which could contribute to increased incidence of ENL in elderly patients.
With regard to histologic subtypes, extranodal origin was the most frequent in DLBCL (57.1%), except for MALT and lymphoblastic lymphoma (only one case), although previous studies [12, 20] reported that 40–42% of DLBCL originate from extranodal sites. In most primary organs, DLBCL was the most frequent histologic subtype. We consider this result would be useful in determining the treatment strategy when appropriate biopsy can not be performed in the patient.
The OS of primary Waldeyer’s ring DLBCL patients was good; however, DLBCL patients with bone marrow as the primary site of origin showed poor survival. The possible reasons for this difference in survival are as follows: [1] Waldeyer’s ring is a sensory organ and the disease can be detected at the localized stage at this site and [2] in this study, more than half cases of primary bone marrow DLBCL proved to be intravascular large B-cell lymphomas, which are reported to show poor prognosis [21].
We conclude that the proportion of primary ENL in HTLV-1 nonendemic area in Japan is higher than that in Western countries. This can be greatly ascribed to the high rate of extranodal origin in DLBCL.
References
Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the Committee on Hodgkin’s Disease Staging Classification. Cancer Res. 1971;31:1860–1.
Jaffe ES, Harris NL, Stein H, Vardiman JW. Pathology and genetics of tumours of haematopoietic and lymphoid tissues. World Health Organization Classification of Tumours. Lyon: IARC Press; 2001.
A predictive model for aggressive non-Hodgkin’s lymphoma: the International Non-Hodgkin’s Lymphoma Prognostic Factors Project. N Engl J Med. 1993;329:987–94. doi:10.1056/NEJM199309303291402.
Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer. 1972;29:252–60. doi:10.1002/1097-0142(197201)29:1≤252::AID-CNCR2820290138≥3.0.CO;2-#.
Sutcliff SB, Gospodarowicz MK. Clinical features and management of localized extranodal lymphomas. In: Keating A, Armitage J, Burnet A, Newland A, editors. Haematological oncology, vol 2. Cambridge: Cambridge University Press; 1992. p. 189–223.
Ahmad M, Malik IA. Non-Hodgkin’s lymphoma in developing countries. In: Magrath IT, editor. The Non-Hodgkin’s lymphomas, 2nd ed. London: Arnold; 1997. p. 1031–54.
d’Amore F, Christensen BE, Brincker H. Clinicopathological features and prognostic factors in extranodal non-Hodgkin’s lymphomas. Danish LYFO Study Group. Eur J Cancer. 1991;27:1201–8.
Otter R, Gerrits WB, Sandt MMVD, Hermans J, Willemze R. Primary extranodal and nodal non-Hodgkin’s lymphoma. A survey of a population-based registry. Eur J Cancer Clin Oncol. 1989;25:1203–10. doi:10.1016/0277-5379(89)90416-1.
Takagi T. Clinical features of extranodal malignant lymphoma—staging classification and treatment strategies. Rinsho Ketsueki. 1999;40:188–91.
Nitsu N, Okamoto M. Activities and analysis. In: Adult lymphoma treatment study group, editors. Malignant lymphoma clinical and pathology. Tokyo: Sentan-igakusha; 2005. p. 14–28.
Zucca E, Roggero E, Bertoni F, Conconi A, Cavalli F. Primary extranodal non-Hodgkin’s lymphomas. Part 2: head and neck, central nervous system and other less common sites. Ann Oncol. 1999;10:1023–33. doi:10.1023/A:1008313229892.
Moller MB, Pedersen NT, Christensen BE. Diffuse large B-cell lymphoma: clinical implications of extranodal versus nodal presentation—a population-based study of 1575 cases. Br J Haematol. 2004;124:151–9. doi:10.1046/j.1365-2141.2003.04749.x.
Devesa SS, Fears T. Non-Hodgkin’s lymphoma time trends: United States and international data. Cancer Res. 1992;52:5432s–40s.
Groves FD, Linet MS, Travis LB, Devesa SS. Cancer surveillance series: non-Hodgkin’s lymphoma incidence by histologic subtype in the United States from 1978 through 1995. J Natl Cancer Inst. 2000;92:1240–51. doi:10.1093/jnci/92.15.1240.
Zucca E, Roggero E, Bertoni F, Cavalli F. Primary extranodal non-Hodgkin’s lymphomas. Part 1: gastrointestinal, cutaneous and genitourinary lymphomas. Ann Oncol. 1997;8:727–37. doi:10.1023/A:1008282818705.
Weisenburger DD. Epidemiology of non-Hodgkin’s lymphoma: recent findings regarding an emerging epidemic. Ann Oncol. 1994;5:19s–24s.
Levine PH, Hoover RN. The emerging epidemic of non-Hodgkin’s lymphoma: current knowledge regarding aetiologic factors. Cancer Res. 1992;52:5425s–574s.
Xu WS, Ho FC, Ho J, Chan AC, Srivastava G. Pathogenesis of gastric lymphoma: the enigma in Hong Kong. Ann Oncol. 1997;8:41–4. doi:10.1023/A:1008265829249.
Luppi M, et al. Additional neoplasms and HCV infection in low-grade lymphoma of MALT type. Br J Haematol. 1996;94:373–5. doi:10.1046/j.1365-2141.1996.d01-1791.x.
López-Guillermo A, et al. Diffuse large B-cell lymphoma: clinical and biological characterization and outcome according to the nodal or extranodal primary origin. J Clin Oncol. 2005;23:2797–804. doi:10.1200/JCO.2005.07.155.
Bogomolski-Yahalom V, et al. Intravascular lymphomatosis—an indolent or aggressive entity? Leuk Lymphoma. 1998;29:585–93. doi:10.3109/10428199809050918.
Acknowledgment
We thank Dr. Juichi Tanabe for collecting clinical data from Fujieda Municipal General Hospital.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fujita, A., Tomita, N., Fujita, H. et al. Features of primary extranodal lymphoma in Kanagawa, a human T-cell leukemia virus type 1 nonendemic area in Japan. Med Oncol 26, 49–54 (2009). https://doi.org/10.1007/s12032-008-9080-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12032-008-9080-0