
Abstract
Background
Gastric carcinoma is usually characterized with significant morbidity and mortality mainly because of late presentation. Late presentation of gastric carcinoma is a prominent feature in developing and poor countries.
Aim of Study
The purpose of this study is to present our experience with the pattern and outcome of gastric tumors at the University of Benin Teaching Hospital, Benin City, Nigeria; with emphasis on late presentation of the patients.
Patients and Methods
The case files of the patients that were managed at the University of Benin Teaching Hospital for gastric tumors over a 5-year period (January 2004 to December 2006) were analyzed for biodata, symptoms and signs of disease, findings at operation, treatment offered, and outcome of treatment.
Results
The male/female ratio was 2.3:1, with the youngest patient being 38 years while the oldest patient was 76 years old. Upper abdominal pain and a palpable mass per abdomen were the commonest symptoms and signs, respectively. Alcohol ingestion was the commonest identifiable risk factor. Only 30.4% of the patients presented within a year of the onset of symptoms. The gastric antrum was affected in over 78% of the cases, and adenocarcinoma was found in about 90% of the patients. Partial gastrectomy with gastrojejunostomy was the commonest procedure carried out. The mortality rate was 39.1%, and of the patients that died, 66.7% occurred within a year from time of diagnosis.
Conclusion
Most of the cases of gastric carcinoma presented in this study presented late with associated significant mortality. Health education is advised with a view to encouraging early presentation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric carcinoma is a major health problem worldwide with associated significant morbidity and mortality. Gastric carcinoma is characterized by marked geographical variations in the incidence and sex distribution [1, 2]. Gastric malignancies are relatively common in places like Japan, Eastern Europe, and China, while it is relatively uncommon in most developing countries like Nigeria and most other African countries [3, 4]. Apart from the worldwide variation in incidence, there are also regional variations within the African continent. For example, there is a higher incidence of gastric carcinoma in Nigeria and South Africa compared with other parts of the African continent. Similarly, in Nigeria, a regional variation in incidence has been recorded. More cases of gastric malignancies are reported from the northern part of Nigeria compared with the other parts of the country [5]. Some reports have indicated a decline in the incidence of gastric malignancies worldwide [6, 7]. However, the decline in incidence has not been apparent in some centers. Alatise et al. reported an incidence of 230 cases of gastric malignancies over a 16-year period giving an annual incidence of 14 cases [8]. Some risk factors for gastric malignancies have also been described by some studies [8–10].Prominent among such risk factors are genetic predispositions, dietary factors, and infection by the spirochete bacteria, Helicobacter pylori [9, 10].
A worrisome dimension about gastric malignancies, like most other malignancies in the developing countries, is that of late presentation with significant morbidity and mortality. Several reasons have been adduced why most patients in the developing countries present late, whereas in places like Japan and other developed countries, most of the patients are seen in the early stages of gastric malignancies.
The purpose of this study is to evaluate the pattern and outcome of gastric malignancies as seen at the University of Benin Teaching Hospital, Benin City, Nigeria, with a view to proffering solutions that may improve the overall prognosis of patients with gastric malignancies.
Patients and Methods
The case files of patients managed for gastric tumors over a 5-year (January 2004 to December 2008) period were studied. Data analyzed included age, sex, main presenting symptoms, duration of symptoms, previous treatment received before presentation, findings on clinical examination, and investigations. Findings at operation, the procedures carried out intraoperatively, histology of tumor, and outcome of surgery were analyzed. The period of survival from time of diagnosis to time of death was also analyzed. The findings are presented in simple tables and percentages.
Cases Excluded
There were three cases (two males and one female) that discharged against medical advice soon after the barium meal results suggested gastric malignancy. Because of incomplete data, they were excluded from the study.
Results
Over the 5-year period, there were 26 cases (18 males and 8 females) of suspected gastric tumors. However, only 23 cases (16 males and 7 females, with a male/female ratio of 2.3:1.) were studied. The age range of the patients was between 38 and 76 years with a mean of 53.7 ± 9.9 years (Table 1). Upper abdominal pain was the dominant symptom in the patients (Table 2). Over 80% of the patients had been on various forms of antiulcer medications even though none of the patients had a radiological or endoscopic diagnosis of peptic ulcer disease. Among the suspected risk factors, alcohol ingestion was the commonest identifiable risk factor (Table 3). Only 30.4% of the patients presented within a year of the onset of symptoms (Table 4). Sixteen patients had evidence of significant weight loss, and eight patients had palpable epigastric tumor on presentation (Table 2). The gastric antrum was the most commonly affected part (Table 5). Ten patients had partial gastrectomy and gastrojejunostomy, while only lymph node biopsy was done in two patients (Table 6). Over 90% of the patients had adenocarcinoma (Table 7). Table 8 shows the outcome of treatment while Table 9 shows the duration of life from time of diagnosis to time of death of the nine patients who died.
Discussion
In the present study, there were 23 cases of gastric malignancies over the 5-year period giving an annual incidence of 4.6 cases. Gastric malignancies are the second most common cancer in the gastrointestinal tract worldwide [11, 12]. Regional variations in the incidence of gastric malignancies even in the same country are a characteristic feature [3, 4, 8]. The incidence in Japan is reported to be 70 per 100,000 per year [2, 4]. Generally, gastric malignancies are less common throughout Africa than in Europe. Gastric malignancies are said to be more common in the northern part of Nigeria compared to the southern part [5]. Exact reasons for these regional variations in Nigeria have not been clearly demonstrated. However, dietary and social lifestyle in general may be a consideration in this direction, and this requires further studies.
Worldwide, gastric malignancies are said to be more common in males. In the present study, the male/female ratio is 2.3:1 and is similar to reports from other studies [8, 13–15]. Alatise et al. reported a male/female ratio of 3:2, Balint reported a male/female ratio of 2.6:1, Mabogunje reported a ratio of 1.3:1, and Siriwardana et al. reported a ratio of 3.5:1 [8, 13–15]. However, even though all the studies indicate a male preponderance, the regional variations in the male/female distribution of gastric malignancies are obvious in these studies. Some studies have attributed the male preponderance in males to a higher intake of alcohol which is associated with gastritis and which may in turn predispose to malignant transformation [8–10].
The peak age of incidence of gastric malignancies varies from center to center. While most studies from the developed countries report peak age of occurrence of mainly elderly patients, studies from developing countries on the other hand report more cases of gastric malignancies occurring in relatively younger patients [3, 4, 8, 16, 17]. In Japan, USA, and UK, most of the patients with gastric malignancies are above 60 years of age [3, 4, 16]. In the present study, the mean age of patients with gastric malignancies was 53.7 ± 9.9 years, and the youngest patient was 38 years. In Alatise et al.’s study, the peak age of occurrence of gastric carcinoma was 41–60 years, with 2.6% of the patients studied below 20 years of age and youngest being 7 years [8]. Similar pattern of gastric malignancies occurring in the very young has been reported from Korle Bu, Ghana [18]. It is possible that the earlier age of occurrence of gastric cancer in Nigeria and most other developing countries may be related to the lower life expectancy compared with what is obtained in the developed world.
The commonest symptom in the patients studied was upper abdominal pain which was present in 82.6%. Most of these patients were being treated for peptic ulcer disease at one point or the other even though there was no endoscopic or radiological diagnosis in any of the patients. Similar patterns have been reported by other studies [8, 18, 19]. Most cases of gastric malignancies initially present with upper abdominal pain as the chief complaint, and treatment for peptic ulcer disease tend to offer some relief, especially in the early stages. This initial relief of pain is one of the reasons why most patients with gastric malignancies present. Thus, it is recommended that before embarking on treatment for peptic ulcer disease, radiological and endoscopic investigations should be done in order to detect early cases of gastric malignancies. However, the value of this recommendation for all cases of suspected peptic ulcer disease is queried by other studies and recommends instead that radiological and endoscopic evaluation should be reserved only for the patients that have risk factors for developing gastric malignancies or when clinical evaluation suggests gastric malignancy [20, 21]. This latter recommendation is borne out of the fact that in most developing countries with scarce resources, not many of the patients can afford the prohibitive cost of barium meal and follow through and upper gastrointestinal endoscopy. Other presenting symptoms were vomiting, weight loss, easy satiety, anorexia, hematemesis, abdominal swelling, and passage of melena stools. These symptoms should make a clinician to suspect gastric malignancy in any patient. The commonest signs elicited were a palpable abdominal mass, epigastric tenderness, cachexia, and anemia. Other signs included visible peristalsis waves, hepatomegaly, succession splash, and ascites. All these signs are suggestive of advanced disease and often associated with poor prognosis. Other studies have reported similar findings [5, 8, 18].
With respect to risk factors for gastric malignancies, chronic alcohol ingestion, chronic use of the nonsteroidal anti-inflammatory drugs, and smoking were more frequently encountered. Other studies on gastric malignancies have reported similar findings [8–10]. Health education about the risk factors for gastric malignancies should be given due consideration as this may lead to alteration in social lifestyle. In this study, we did not evaluate the role of H. pylori in the development of gastric malignancies. However, other studies have reported a close association between H. pylori and development of gastric malignancies [22, 23]. In this respect, screening for and eradication of H. pylori have been recommended with a view to decreasing the overall incidence of gastric malignancies.
Late presentation was a prominent feature in this study. Most of our patients presented after about 2 years of the onset of symptoms. Most delays were caused either by use of various medications for suspected peptic ulcer diseases or inability to access health facilities for financial reasons. Other studies on gastric malignancies in the developing countries have similarly reported late presentation of patients that have gastric malignancies with associated significant morbidity and mortality [5, 8, 18]. Concerted efforts on health education of the populace with respect to features of gastric malignancies may help in reversing the trend of late presentation and thus improve the overall outcome of gastric malignancies.
About 78% of the cases presented in this study were antral tumors while another 13% had involvement of the body and antrum. There was a case of each of tumor involving the body and the entire stomach. Several studies have reported this pattern of presentation of gastric malignancies [8, 9, 11, 16–18]. Some other studies have however reported a changing pattern toward having more cases of gastric tumors involving the cardia and upper parts of the stomach [24, 25]. Several reasons have been adduced for this emerging pattern, especially in the western world [24, 25].
Adenocarcinoma was the commonest histological type in this study as over 90% of the patients had adenocarcinoma. There was only one case of each gastric lymphoma and leiomyoma. This pattern has been reported by other studies [1, 2, 8, 18].
In the present study, only about 43.5% of the patients had partial gastrectomy and jejunostomy. Partial gastrectomy was not possible in the other patients because at operation, the tumors were adjudged to be nonresectable. Thus, 39.1% of the patients had only a gastrojejunostomy bypass, 8.7% had only lymph node biopsy, and another 8.7% were not fit for operation and so only had a postmortem for confirmation of diagnosis. Only 16 patients received chemotherapy while the remaining seven patients did not receive chemotherapy, as they were considered too ill to receive any form of cytotoxic chemotherapy. The pattern presented here depicts the result of late presentation. This pattern of is similar to other studies in the developing countries where late presentation is characteristic [5, 8, 17, 18]. However, in Japan and other developed countries, their rate of resection is higher than what is presented in this study because their patients present earlier than our patients, and thus, they tend to have a better outcome with respect to management of gastric malignancies [3, 4].
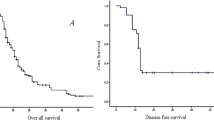
In this study, about 39.1% of the patients studied had died, 30.4% are still being followed up, 26.1% were lost to follow-up, and one of the patients discharged against medical advice. Of the nine cases of mortality, only one patient was alive at 2 years from time of diagnosis while 54% did not live beyond 1 year from time of diagnosis. This study shows the very gloomy picture of gastric malignancies as seen in the developing countries. This pattern of poor outcome of gastric malignancies has been reported by studies in the developing countries [5, 8, 17, 18]. This study also shows the difficulties we have in most centers with respect to follow-up of patients and thus tend to create problems in having a comprehensive statistical data. Some other studies have similarly reported the problems associated with losing patients to follow-up and discharges against medical advice [26, 27]. Health education is urgently required to reverse this trend and thus assist in improving the overall outcome of patient care.
In conclusion, gastric malignancy is not very common at the University of Benin Teaching Hospital, but it is associated with poor outcome. Most of the patients presented very late with associated significant morbidity and mortality. Virtually, all the patients were on one form of antiulcer medications or the other, and this was chiefly responsible for the late presentation. Vigorous health education is urgently needed so that patients with suspected gastric malignancies can present early and thus improve on the overall outcome of the management of gastric malignancies.
References
Yeoh KG. How do we improve outcomes of gastric cancer? J Gastroenterol Hepatol. 2007;22:970–2.
Kandasami P, Tan WJ, Norain K. Gastric cancer in Malaysia: the need for early diagnosis. Med J Malaysia. 2003;58:758–62.
Inoue M, Tsugane S. Epidemiology of gastric cancer in Japan. Postgrad Med J. 2005;81:419–24.
Vaquerano J, Esemuede N, Odocha O, Leffall LD. Gastric carcinoma in African Americans: a ten year single center analysis. In Vivo. 1996;10:233–5.
Oluwasola AO, Ogunbiyi JO. Gastric cancer: aetiological, clinicopathological and management patterns in Nigeria. Niger J Med. 2003;12:177–86.
Howson CP, Hiyama T, Wynder EL. The decline in gastric cancer: epidemiology of an unplanned triumph. Epidemiol Rev. 1986;8:1–27.
Rad R. Gastric cancer in Japan. NEJM. 2008;359:2394–5.
Alatise OI, Lawal OO, Adesunkanmi AK, et al. Clinical patterns and management of gastric cancer in Ile-Ife Nigeria. Arb Journal of Gastroenterol. 2007;8:123–6.
Oluwasola AO, Ogunbiyi JO. Helicobacter pylori-associated gastritis and gastric cancer in Nigeria. Indian J Gastroenterol. 2003;22:212–14.
Tsugane S, Sasazuki S. Diet and the risk of gastric cancer: review of epidemiological evidence. Gastric Cancer. 2007;10:75–83.
Jemal A, Tiwari RC, Murray T, et al. Cancer statistics 2004. CA Cancer J Clin. 2004;54:8–29.
Parkin DM. Global cancer statistics in the 2000. Lancet Oncol. 2001;2:533–43.
Balint GA. Gastric and colorectal cancer in the tropical part of Africa. Acta Medica Hunganca. 1990;47:91–8.
Mabogunje OA, Lawrie JH. Surgical management of advanced gastric carcinoma in Zaria, Nigeria. Eur J Surg Oncol. 1985;11:361–4.
Sirwardana HD, Pathirana A. Adenocarcinoma of the stomach in a tertiary care hospital in Sri Lanka. Ceylon Med J. 2007;52:53–5.
Sue-Ling HM, Johnston D, Martin IG, Dixon MF, Landsdown MRJ, McMahon MJ, et al. Gastric cancer: a curable disease in Britain. Br Med J. 1993;307:591–6.
Obekpa PO, Onumiya JE, Nwana EJC, et al. A clinicopathological review of gastric malignancies in the middle belt of Nigeria. Nig Med Pract. 1994;27:67–72.
Takyi HK. A review of cancer of the stomach as seen in Korle Bu Teaching Hospital. Ghana Med J. 1972;11:133–6.
Suvakonic Z, Bramble MG, Jones R, Wilson C, Idle N, Ryott T. Improving the detection rate of early gastric cancer requires more than open access gastroscopy: a five year study. Gut. 1997;41:308–13.
Breslin NP, Thomson ABR, Bailey RJ, Bluestein RK, Meddings J, Lafor E, et al. Gastric cancer and other endoscopic diagnosis in patients with benign dyspepsia. Gut. 2000;46:93–7.
Danbauchi SS, Kenshiri IB, Abdu-Guasu K. Fifteen years of upper gastrointestinal endoscopy in Zaria (1978–1993). Afr J Med Sci. 1999;28:87–90.
Wang C, Yuan Y, Hunt RH. The association between Helicobacter pylori infection and early gastric cancer: a metaanalysis. Am J Gastroenterol. 2007;102:1789–98.
Lawal OO, Rotimi O, Okeke I. Helicobacter pylori in gastrointestinal diseases. J Natl Med Assoc. 2007;99:31–4.
Hassan HA, Sharma VK, Raufman JP. Changing trends in gastric carcinoma at a university medical centre: a twelve year retrospective analysis. J clin Gastroenterol. 2001;32:37–40.
Borch K, Jonsson B, Tarpila A, et al. Changing pattern of histological type, location, stage and outcome of surgical treatment of gastric carcinoma. Br J Surg. 2002;87:618–26.
Ohanaka EC. Discharge against medical advice. Trop Doct. 2002;32:149–51.
Yawe KT, Bakari AA, Pindigu H, Mayun AA. Clinocopathological pattern and challenges in the management of colorectal cancer in sub-Saharan Africa. J Chin Clin med. 2007;2:688–94.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Osime, O.C., Momoh, M.I., Irowa, O.O. et al. Gastric Carcinoma—A Big Challenge in a Poor Economy. J Gastrointest Canc 41, 101–106 (2010). https://doi.org/10.1007/s12029-009-9118-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-009-9118-3