
Abstract
Introduction
It has been shown that CD44 may be associated with poor prognosis in various human malignancies. This study was designed to investigate and compare the prognostic relevance and clinical value of soluble forms of CD44 and its variant v6 (CD44v6) and their tissue expression in colorectal carcinoma.
Materials and methods
Serum levels of pre- and postoperative CD44 and CD44v6 molecules were evaluated in 37 colorectal cancer patients and compared to healthy individuals.
Results and discussion
The serum levels of soluble CD44 and CD44v6 showed no significant decrease after surgical resection of the tumor (p = 0.5). Both CD44 and CD44v6 serum levels either before or after surgery were significantly higher in patients than in normal individuals (p < 0.001). The serum level of CD44v6 molecule was higher in patients with lymph node metastasis than other patients (p = 0.05) implying the role of this molecule in tumor progression. Immunohistochemical staining showed expression of CD44 in 14.3% and CD44v6 in 42.9% of the tumor samples. The expression of CD44v6 was associated with metastatic involvement of lymph nodes (p = 0.03). CD44v6 expression was positively correlated with its level in the serum of patients (p = 0.04).
Conclusions
Results of this study showed that CD44v6 expression level either in the soluble form or in the cell membrane is associated with tumor metastasis indicating the importance of this molecule in progression of colorectal carcinoma. The serum levels of soluble CD44 as well as CD44v6 might be useful markers for tumor screening.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal carcinoma is one of the most common gastrointestinal malignancies with increasing occurrence in recent years in Iran like in other parts of world [1]. The prognosis of the disease is largely dependent on tumor stage at the time of surgery and is poor when development of metastasis has occurred. The process of metastasis has been shown to occur in different steps including adhesion to capillaries of distant organs. Certain highly metastatic cells have been shown to adhere strongly via adhesion molecules to endothelial cells and basement membrane components [2]. Cell adhesion molecules play an important role in cell–cell and cell–extracellular matrix adhesion [3].A unique group of adhesion molecules are CD44 surface molecules. CD44 is a family of glycoprotein molecules, first described by Dalchau et al. [4]. These molecules are involved in many physiological and pathological processes and have been proposed to function as a homing lymphocyte receptor [5]. The CD44 molecule also binds the extracellular matrix components hyaluronic acid, fibronectin, and collagen [5]. CD44 is known to be linked with the development and spread of carcinoma including metastasis [6]. A number of different CD44 isoforms are produced by alternative splicing of exons 6 (V1-2) to exon 14 (v10) [6]. The significance of the expression of CD44 protein variant 6 (CD44v6) have been shown to confer metastatic potential to tumor cells [7]. CD44v6 is thought to be positively correlated with invasive growth and metastasis development in some tumors [8, 9]. In addition to the expression on the cell membrane, CD44 proteins are also released from cells, and soluble CD44 proteins are detectable in the normal human circulation [10]. The basic level of soluble CD44 in the circulation is thought to have its origin in lymphocytes [11]. The observation that several human tumors show an overexpression of certain CD44 isoforms [12, 13] and the presence of soluble CD44 isoforms in the circulation may make CD44 a candidate for a potential serum marker for tumor detection. In a recent study, it has been demonstrated that soluble CD44 secretion contributes to the acquisition of aggressive tumor phenotype in human colon cancer cells [14]. However, more studies are needed to clarify the role of soluble forms of CD44 and CD44v6 as possible prognostic antigens in colorectal carcinoma. The current study is aimed at determining the serum level of these molecules to find their possible correlation with colorectal carcinoma and to identify the correlation of these molecules to each other and compare their clinicopathological parameters including tumor size, grade, stage, and lymph node metastasis. Moreover, considering the previous studies reporting the importance of CD44 and CD44v6 cell membrane expression in progression of colorectal cancer, the role of CD44 and CD44v6 soluble forms in relation to their immunohistochemical expression was also investigated.
Materials and Methods
Specimens
Blood samples were collected from 37 patients with proven adenocarcinoma of the colon (22 men and 15 women) before and 3 months after surgical resection of tumor. The serum was isolated and stored at −70°C until use. Serum was also prepared from 37 age- and sex-matched healthy individuals. Informed consent was obtained from all individuals participating in this study. The protocols were approved by the ethical committee of the Shiraz University of Medical Sciences. The average patients age was 55.3 ± 16 and ranged from 24 to 78 years. Tissue samples of colorectal carcinomas, as well as normal mucosa adjacent to the neoplastic tissue, were obtained during surgery. Tissue specimens were fixed with 10% formalin and embedded in paraffin, and cut into 5-μm sections for histological evaluation by routine hematoxylin and eosin staining as well as immunohistochemical staining. Grading and staging of tumors was done according to the TNM classification.
Immunohistochemistry
Tissue sections were deparaffinized and rehydrated and were incubated with 3% H2O2 to inactivate endogenous peroxidase activity. Slides were heated in 10 mM citrate buffer for antigen retrieval. Following a 20-min blocking step with 10% normal horse serum, the primary antibody was applied and incubated overnight. Primary antibodies were mouse anti-human monoclonal anti CD44 (clone, F10-44-2, Serotec GmbH, Germany) and anti CD44v6 (Clone VFF-7, Serotec). After treating with biotinylated anti-mouse IgG and avidin–peroxidase (Dako Glostrup, Denmark) for 30 min each, diaminobenzidine (Dako) 1 mg/ml in phosphate-buffered saline containing 0.03% hydrogen peroxide was applied as the chromogen. Sections were counterstained with hematoxylin for 15 s. A negative control study was performed by using unrelated antibody instead of primary antibody. Immunostaining intensity was rated as follows: very low or no staining as negative, weakly staining 1, moderate 2, and strong 3.
Enzyme-Linked Immunosorbent Assay
Soluble forms of CD44 and CD44v6 were measured in serums using enzyme-linked immunosorbent assay (ELISA) kits (Biosource, Nivelles, Belgium). Sensitivity of kits was 0.015 ng/ml for CD44 and 0.05 ng/ml for CD44v6. Assays were performed according to the manufacturer’s instructions. Briefly, specific monoclonal antibody was coated in wells of 96-well microtiter plates. CD44 or CD44v6 present in the properly diluted serum or in the standard bound to antibodies adsorbed to each wells. Horseradish peroxidase-conjugated monoclonal antibody against CD44 or CD44v6 was added. After incubation, unbound enzyme-conjugated antibodies were removed by washing, and a substrate solution was added to each well. Optical density in each sample was measured at 450 nm. A standard curve was prepared from six standard dilutions of antigens, which allowed determination of the levels of CD44 and CD44v6 in our samples.
Statistics
SPSS version 10 (SPSS, Chicago, IL, USA), independent samples t test, Chi-square and Spearman correlation coefficient were used for statistical analysis. P ≤ 0.05 was considered statistically significant.
Results
The characteristics of the patients are shown in Table 1. The locations of the tumors were in the rectum in 14 (37.9%) patients and in the colon in 23 (62.1%). Staging was available in 26 cases, in that five (19.2%) were Duke’s A, ten (38.5%) Duke’s B, and 11 (42.3%) were clinically stage C. In the patients, 84.4% of the tumors were well differentiated, and 15.6% were moderately differentiated. Lymph node metastasis was observed in 34.6% of cases.
Measurement of CD44 and CD44v6 in the serum of patients before and after surgery and in normal individuals was performed by ELISA. The mean serum CD44 level in the patients before (875 ± 204 ng/ml) and after surgery (853 ± 196 ng/ml) indicated no significant difference (p = 0.5, Table 2). CD44 serum level in patients both before and after surgery was significantly higher than its level in the control group (696 ± 259 ng/ml; p < 0.001). The mean serum level of preoperative CD44 in male patients (982 ± 170 ng/ml) was significantly higher than those in female patients (796 ± 205 ng/ml; p < 0.001). CD44 serum level in the control group was also higher in males (732 ± 268 ng/ml) than in females (642 ± 243 ng/ml; p < 0.001).
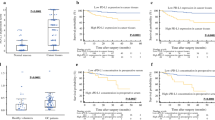
CD44v6 in the serum of patients before (131 ± 34 ng/ml) and after (133 ± 34 ng/ml) surgery showed no significant difference (p = 0.8). Comparing these levels with CD44v6, serum level in normal individuals (82.8 ± 19.6 ng/ml) indicated the higher concentration of this molecule in patients (p < 0.0001). The serum level of CD44v6 in relation to CD44 showed no correlation. CD44v6 was higher in male than female patients (p = 0.02). Although CD44v6 levels showed an increase in the serum of patients with greater size and stage of tumor, however, the result was not significant. A significant higher level of CD44v6 in patients with lymph node metastasis was observed in comparison to patients without metatasis (p = 0.05; Fig. 1).

Relationship between the serum level of CD44v6 and lymph node metastasis (absent or present) in patients. Bars indicate the mean ± SD of the serum concentrations (ng/ml) before and after surgical resection of tumor
Slide for immunohistochemistry was available in 28 patients. Paraffin-embedded specimens of colorectal cancer were analyzed for the expression of CD44 as well as CD44v6. The immunohistochemistry results were evaluated in terms of the percentage of immunopositive tumor cells and relative immunointensity. Membranous pattern of CD44 expression was observed in 14.3% of cases ranging from 20% to 70% of tumor cells (Fig. 2a). Expression was not significantly different from normal epithelial tissue (p = 0.1) in that CD44 showed very weak staining.

Expression of CD44 (a) and CD44v6 (b) in colorectal cancer patients. Magnification ×200
Different cytoplasmic or membranous patterns of CD44v6 expression with different staining intensity was observed in 12 (42.9%) patients (Fig. 2b). Expression was significantly higher compared with normal epithelial cells (p < 0.0001) in that CD44v6 was not detected. Metastasis to lymph nodes was found in seven out of 12 patients with CD44v6 expression compared to two out of 14 of CD44v6-negative tumors (p = 0.03) showing a higher expression of CD44v6 in patients with metastasis to lymph nodes. Correlation between CD44v6 expression and stage as well as grade was not significant.
No significant association between CD44 and its tissue expression was observed; however, soluble CD44v6 was positively correlated with its expression in tumor tissue cells (p = 0.04).
Discussion
It has been documented that functional fragments of the CD44 and its isoforms can be liberated from the cell membrane by extracellular and intramembrane proteolysis [15]. Soluble CD44 and its variant v6 have been shown to correlate with tumor metastasis in a number of malignancies [16, 17]. Conversely, no significant correlation between serum levels of CD44 and CD44v6 with the presence or absence of several cancers has been observed [18, 19]. In the present study, soluble CD44 in colorectal cancer patients and in normal individuals was detected. The low level of circulating CD44, found in healthy individuals, may be shed from normal lymphocytes. The mean concentration of CD44 in patient’s serum was significantly more than that of the control group. Similarly, in a previous study on 89 colorectal carcinoma patients, the concentration of CD44 was higher than the normal individuals indicating the role of soluble CD44 in particular, as a marker of cancer diagnosis [20]. In order to find the relationship between CD44 and the tumor mass, we measured the concentration of soluble CD44 before and after operation. Although surgical resection of the tumor mass reduced circulating CD44 levels, the difference in its level before and after operation was not significant. This may indicate that assessment of soluble CD44 may not be a suitable method to monitor the efficacy of treatment. The level of CD44 showed no significant difference in patients with well differentiated compared to those with moderately differentiated carcinoma. The concentration of soluble CD44 in relation to tumor size showed no significant correlation, though, patients with greater tumor size exhibited higher concentrations of CD44 rather than patients with smaller tumor size. In the present study, no significant correlation between CD44 serum level and stage was observed.
In terms of soluble CD44v6, similar to CD44, either pre- or postoperative serum level in patients was higher than normal individuals. The serum level of CD44v6 after operation showed no significant changes suggesting the release of this circulating protein from other biological sources such as activated lymphocytes or other nucleated blood cells. Only a few studies have been conducted concerning the role of soluble serum CD44v6 in relation to metastasis and pathological features in patients with colorectal cancer [21–23]. Zalewski and colleagues reported no association between CD44v6 expression estimated in the serum and any clinicopathological features in patients with colorectal adenocarcinoma [21]. No correlation to tumor burden was obtained in another study [22]. In contrast, CD44v6 has been significantly associated with lymph node metastasis on 44 patients before surgery [23]. In the present study, the serum CD44v6 level was higher in patients with lymph node metastasis than those without lymph node metastasis; this indicates the importance of soluble CD44v6, as a tumor marker of progression in colorectal carcinoma.
A finding in this study was the significant higher amounts of both preoperative soluble CD44 and CD44v6 serum levels in male patients than females that showed the effect of gender on the production or release of these molecules. It is noted that the percentage of male patients with metastasis in our study was 41.7% compared to 20% for female patients with metastasis (p < 0.05, data not shown). In addition, a higher number of male patients (52.8%) were in stages 3 and 4 compared to female patients (27.3%, p < 0.05). These data suggest the more aggressiveness of the disease in males than females. In some previous studies, male sex has been reported as a negative prognostic factor in colorectal carcinoma. [24, 25] This may be a reason for higher amounts of sCD44 and sCD44v6 observed in male patients than female ones. However, both sCD44 and sCD44v6 were higher in normal males than females as well, that may show the more stability of these molecules in males than in females.
In order to find the relevance of soluble CD44 and its variant v6 to their tumor cell expression in colorectal cancer, we studied the patients using embedded materials by immunohistochemistry and evaluated the relationship of this expression and clinicopathologic characteristics of patients. Results obtained showed the expression of CD44 in nearly 14% of patients. CD44v6 was positive in almost 43% of cases. CD44v6 was more expressed in Duck’s C stage of tumor cells in comparison to other stages, but the difference was not significant. The higher frequency of tumor tissue CD44v6 positivity in cases with metastasis indicates the prognostic value of this protein in colorectal carcinoma. This result is compatible with previous reports in which tumor tissue CD44v6 positivity has been associated with metastasis in colorectal cancer patients [26, 27].
Whether soluble forms of CD44 and CD44v6 were correlated with their tissue expression in patients was investigated. The serum level of CD44 showed no significant correlation with either CD44 or CD44v6 positivity; however, the level of soluble CD44v6 was positively correlated with the level of CD44v6 expression in tumor cells. In two previous studies, soluble CD44 and CD44v6 serum levels in relation to their expression on tumor tissue has been studied in patients with colorectal cancer. Similar to our study, Yemen and colleagues have reported a higher serum level of CD44v6 in those patients with CD44v6-positive tumor tissues than in those with CD44v6-negative ones [23]. Contrarily, no correlation between the serum level of CD44 and CD44v6 concentrations to CD44v6 tissue expression have been shown by Weg-Remers et al. [22]. These differences in the results may be due to differences in the number of patients, tumor cells biology, and or be due to the different techniques used in the studies, as in the former study, tissue expression of CD44v6 has been investigated by reverse transcriptase-polymerase chain reaction, whereas in the later one, immunohistochemical staining has been used.
Taken together as results of this study showed that serum CD44 and CD44v6 levels were both significantly higher in colorectal cancer patients than the normal individuals, suggesting the usefulness of these markers for tumor screening, though, their production by different sources, including their release from the lymphocytes can be a limitation to use them for screening and monitoring patients. Other findings including correlation of soluble CD44v6 to metastasis and its higher immunohistochemical expression in metastatic tumors than non-metastatic ones indicates the importance of this molecule in the progression of colorectal carcinoma in patients. Measurement of soluble form of CD44v6 in serum and/or immunohistochemical staining for CD44v6 seems to be simple methods for evaluation of metastasis in colorectal cancer patients. Further studies on a larger number of patients may provide important additional information for prognostic relevance of these molecules in colorectal cancer patients.
References
Hosseini SV, Izadpanah A, Yarmohammadi H. Epidemiological changes in colorectal cancer in Shiraz, Iran:1980–2000. ANZ J Surg. 2004;74:547–9.
Orr FW, Wang HH. Tumor cell interactions with the microvasculature: a rate-limiting step in metastasis. Surg Oncol Clin N Am. 2001;10:357–81.
Iiizumi M, Mohinta S, Bandyopadhyay S, et al. Tumor–endothelial cell interactions: therapeutic potential. Microvasc Res. 2007;74:114–20.
Dalchau R, Kirkley J, Fabre JW. Monoclonal anti-body to a human leukocyte-specific membrane glyco-protein probably homologous to the leukocyte-common (L-C) antigen of the rat. Eur J Immunol. 1980;10:737–44.
Dianzani U, Malavasi F. Lymphocyte adhesion to endothelium. Crit Rev Immunol. 1995;15:167–200.
Screaton GR, Bell MV, Jackson DG, et al. Genomic structure of DNA encoding the lymphocyte homing receptor CD44 reveals at least 12 alternatively spliced exons. Proc Natl Acad Sci USA. 1992;89:12160–4.
Günthert U, Hofmann M, Rudy W, et al. A new variant of glycoprotein CD44 confers metastatic potential to rat carcinoma cells. Cell. 1991;65:13–24.
Iida N, Bourguignon LYW. New CD44 splice variants associated with human breast cancers. J Cell Physiol. 1995;162:127–33.
Manten-Horst E, Danen EH, Smit L, et al. Expression of CD44 splice variants in human cutaneous melanoma and melanoma cell lines is related to tumor progression and metastatic potential. Int J Cancer Pred Oncol. 1995;64:182–8.
Picker LJ, De Los Toyos J, Telen MJ, et al. Monoclonal antibodies against the CD44 [in(lu)-related p80] and pgp-1 antigens in man recognize the Hermes class of lymphocyte homing receptors. J Immunol. 1989;142:2046–51.
Bazil V, Horejsi B. Shedding of the CD44 adhesion molecule from leukocytes induced by anti-CD44 monoclonal antibody simulating the effect of a natural receptor ligand. J Immunol. 1992;149:747–53.
Ristamäki R, Joensuu H, Jalkanen S. Does soluble CD44 reflect the clinical behavior of human cancer? Curr Top Microbiol Immunol. 1996;213:155–66.
Gansauge F, Gansauge S, Rau B, et al. Low serum levels of soluble CD44 variant 6 are significantly associated with poor prognosis in patients with pancreatic carcinoma. Cancer. 1997;80:1733–9.
Subramaniam V, Gardner H, Jothy S. Soluble CD44 secretion contributes to the acquisition of aggressive tumor phenotype in human colon cancer cells. Exp Molecular Pathol. 2007;83:341–6.
Cichy J, Pure E. The liberation of CD44. J Cell Biol. 2003;161:839–43.
Andratschke M, Chaubal S, Pauli C, et al. Soluble CD44v6 is not a sensitive tumor marker in patients with head and neck squamous cell cancer. Anticancer Res. 2005;25:2821–6.
Lein M, Jung K, Weiss S, et al. Soluble CD44 variants in the serum of patients with urological malignancies. Oncology. 1997;54:226–30.
Kainz C, Tempfer C, Winkler S, et al. Serum CD44 splice variants in cervical cancer patients. Cancer Lett. 1995;90:231–4.
Jung K, Lein M, Weiss S, et al. Soluble CD44 molecules in serum of patients with prostate cancer and benign prostatic hyperplasia. Eur J Cancer. 1996;32A:627–30.
Masson D, Denis MG, Denis M, et al. Soluble CD44: quantification and molecular repartition in plasma of patients with colorectal cancer. Br J Cancer. 1999;80:1995–2000.
Zalewski B. Levels of v5 and v6 CD44 splice variants in serum of patients with colorectal cancer are not correlated with pT stage, histopathological grade of malignancy and clinical features. World J Gastroenterol. 2004;10:583–5.
Weg-Remers S, Hildebrandt U, Feifel G, et al. Soluble CD44 and CD44v6 serum levels in patients with colorectal cancer are independent of tumor stage and tissue expression of CD44v6. Am J Gastroenterol. 1998;93:790–4.
Yamane N, Tsujitani S, Makino M, et al. Soluble CD44 variant 6 as a prognostic indicator in patients with colorectal Cancer. Oncology. 1999;56:232–8.
Perez-Palma J, Marchena-Gomez J, Dorta-Espineira M, et al. Predictive factors of years of potential life lost by colorectal cancer. Eur J Gastroenterol Hepatol. 2008;20:766–72.
Mai SK, Welzel G, Hermann B, et al. Long-term outcome after combined radiochemotherapy for anal cancer—retrospective analysis of efficacy, prognostic factors, and toxicity. Onkologie. 2008;31:251–7.
Bendardaf R, Algars A, Elzagheid A, et al. Comparison of CD44 expression in primary tumours and metastases of colorectal cancer. Oncol Rep. 2006;16:741–6.
Zhang JC, Wang ZR, Cheng YJ, et al. Expression of proliferating cell nuclear antigen and CD44 variant exon 6 in primary tumors and corresponding lymph node metastases of colorectal carcinoma with Dukes’ stage C or D. World J Gastroenterol. 2003;9:1482–6.
Acknowledgement
The authors are grateful to Fatemeh Safaei, Saied Malekhosseini, and Hossein Golmoghaddam for providing invaluable assistance. This work was supported by grants 2287 and 2802 from Shiraz University of Medical Sciences.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amirghofran, Z., Jalali, S.A., Hosseini, S.V. et al. Evaluation of CD44 and CD44v6 in Colorectal Carcinoma Patients: Soluble Forms in Relation to Tumor Tissue Expression and Metastasis. J Gastrointest Canc 39, 73–78 (2008). https://doi.org/10.1007/s12029-009-9062-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-009-9062-2