
Abstract
Background
Hepatocellular carcinoma (HCC) is a common cancer in certain portions of the world. Currently no effective therapies exist for patients with advanced or metastatic HCC. KW-2189, a DNA minor groove-binding agent, has shown promising activity against HCC in preclinical evaluations.
Methods
A phase II study was conducted to evaluate the activity of KW-2189 in patients with histologic or cytologic confirmed advanced or metastatic HCC who had no prior systemic therapy. Patients received KW-2189 at a dose of 0.5 mg/m2 administered on day 1 of a 6-week cycle. The primary endpoint of the trial was objective regression. Other endpoints included toxicity, disease-free survival, and overall survival.
Results
Due to hematologic toxicity the dose of KW-2189 was reduced to 0.375 mg/m2 after 11 patients had been enrolled into the trial. Due to continued significant hematologic toxicity in the next five patients enrolled at the lower dose the trial was closed to accrual. Two responses were seen in patients enrolled at the higher dose, including one sustained CR.
Conclusion
KW-2189 showed evidence of anti-tumor activity in HCC. However, because of significant and prolonged hematologic toxicity, when given as a single dose every 6 weeks, further development of this drug in HCC is not possible. Further exploration of DNA minor groove-binding agents in the treatment of HCC appears warranted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The majority of patients presenting with hepatocellular carcinoma (HCC) will have advanced disease at the time of presentation with only 10–30% having potentially resectable disease. [1] Few effective options are available for the treatment of unresectable disease. Chemotherapy, in particular, has been of limited benefit for patients with unresectable or metastatic HCC. [2] As such there is a need for new agents with activity in HCC.
The duocarmycins (DUMs) are a new group of antitumor antibiotics produced by Streptomyces. [3–6] The DUM’s antitumor activity occurs through a sequence-specific covalent binding to the minor groove of DNA, which in turn leads to DNA fragmentation. [7, 8] This DNA binding activity appears to be similar to that seen with other minor groove-binding agents including CC-1065 and its analogues. [9] While a variety of DUMs have been described, their use has been limited by their instability in aqueous solutions and in serum.
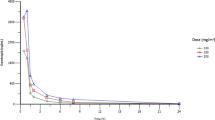
KW-2189 is a semisynthetic, water-soluble, derivative of DUM B2. [10] Once administered, KW-2189 is enzymatically cleaved by carboxyl esterase to its active metabolite DU-86. [11] Preclinical studies with KW-2189 and DU-86 suggest that the antitumor activity occurs through S-phase arrest rather than DNA fragmentation. [8] DNA fragmentation appears to only occur with prolonged exposure, a mode of action similar to that observed with CC-1065 and different from that of the other DUMs. [12]
Preclinical studies of KW-2189 have shown significant antitumor activity in a variety of murine tumor models and human tumor xenografts. [11] Based on the promising activity of KW-2189 in the preclinical setting a phase II clinical trial was performed in patients with HCC. The dose of KW-2189 was previously established through phase I trials. [13, 14] We now report the results of a phase II clinical trial conducted by the NCCTG.
Methods
Eligibility
Patients with histologic or cytologic confirmation of HCC deemed unresectable and not candidates for liver transplant were eligible and were required to be at least 18 years and to have an Eastern Cooperative Oncology Group (ECOG) performance score of 0–2. Contraindications included: a neutrophil count <1,500 cells/mm3; platelet count <100,000 cells/mm3; serum creatinine >0.3 mg/dl above upper limit of normal (ULN); total bilirubin >0.3 mg/dl above ULN; aspartate transaminase (AST) >5 times ULN; major surgery within 4 weeks before registration; known active CNS metastases, other active malignancy,. Prior chemotherapy, immunotherapy, biologic therapy, or radiotherapy was not allowed. Pregnant or lactating women were not eligible. Women of childbearing potential were to use adequate contraception. The institutional review boards of all participating institutions approved this study, and written informed consent was obtained from each patient before study entry.
Treatment
Patients received KW-2189 at a dose of 0.5 mg/m2 on day 1 of a 6-week cycle as an intravenous push during 30 to 60 s via side port free-flowing D5W infusion. Patients who had a complete disappearance of their tumor on two consecutive evaluations at least 6 weeks apart could be retreated for an additional cycle. For those patients whose tumor remained stable or demonstrated partial response, treatment was continued until progression.
At the time of retreatment, patients who experienced a severe (NCI Common Toxicity Criteria Version 2.0 grade III or IV) nonhematologic toxicity had treatment held until the severity of the toxicity was less than grade III, and then retreated at half their previous dose. If the toxicity persisted for more than 3 weeks, treatment was discontinued. If the neutrophil count was <1,500 cells/mm3 or platelet counts were >75,000 cells/mm3 at the time of retreatment, treatment was to be held until the counts rose above these levels and then the patient was to be retreated at 75% of their previous dose. Dose reductions to a level of 50% of the starting dose were permitted before a patient was discontinued from study therapy. Use of G-CSF was not permitted.
Evaluation
Patients underwent evaluation within 14 days before registration, before subsequent retreatments, and at the end of treatment. This involved a complete medical examination, measurement of the indicator lesion, hematologic and chemistry group readings, tumor assessment, and toxicity monitoring. At the time of study entry and at end of treatment, the patients also underwent a serum pregnancy test if of childbearing potential, urinalysis, and an electrocardiogram. After treatment was terminated, the patients entered an observational phase where they underwent a complete physician examination, tumor assessment, and toxicity monitoring every 3 months for the first year after registration and then every 6 months in years 2 to 5 after registration.
Disease Assessment
A measurable indicator lesion is defined as a tumor mass with clearly defined bidimensional measurements whose minimum size is at least 1.0 cm on chest radiograph or ruler or at least 2.0 cm on computed tomography scan, magnetic resonance imaging, or ultrasound. An assessable indicator lesion is defined as a tumor mass on physical examination or imaging study that can be assessed as to its changes in size but cannot be clearly measured in two dimensions. A patient is said to have responded to treatment if on two consecutive evaluations at least 6 weeks apart, there is a total disappearance of tumor [complete response (CR)] or a reduction of at least 50% in the sum of the products of the perpendicular diameters of a measurable lesion [partial response (PR)] or definite clinical evidence of a decrease in the size of an assessable lesion [regression (REG)]. Progression is defined as the appearance of new lesions; significant clinical deterioration not attributable to treatment or other medical conditions; a 25% or greater increase (definite increase) in the size of the indicator lesion from its smallest size for those patients who achieved a PR (REG); or a 25% or greater increase (definite increase) in the size of the indicator lesion from its pretreatment size for those patients who did not achieve a PR (REG). Stable disease is the failure to meet the criteria for response or progression.
Statistical Considerations
The primary endpoint of this trial was objective regression rate (CR, PR) which was defined as the number of patients whose tumor meets this criteria on two consecutive evaluations at least 37–45 days apart. A patient is considered evaluable if they met all eligibility criteria and initiated treatment. A two-stage phase II design was used with a significance level of 0.048 and power of 0.80 to test whether the true objective regression rate was at most 10% when the true objective regression rate is at least 25%. [15, 16]
Secondary endpoints were disease-free survival and overall survival. All the patients who met the eligibility criteria, signed a consent form, and had begun treatment were considered assessable for objective regression rate, distribution of progression-free survival, and distribution of overall survival. Confidence intervals for the true objective regression rate were constructed using the Duffy-Santner approach. The duration of treatment response was defined as time from the first of the two evaluations qualifying the patient as responder (PR or CR) until the date at which disease progression was noted. Time to progression is defined as the time from registration to disease progression. The patients who died without documentation of progression were considered to have had tumor progression on the date of death unless documented evidence clearly indicated that no progression occurred. Survival time was defined as the time from registration to death. Times to event distributions were estimated using the Kaplan-Meier method.
Results
Accrual to this trial was suspended after 11 patients with HCC treated at the 0.5 mg/m2 level due to severe myleosuppression that persisted in subsequent treatment cycles. The study was reopened to accrual at a starting dose of 0.375 mg/m2, and five additional patients were enrolled. Since the toxicity profile in these five patients was similar to that seen at the higher dose level, the study was permanently closed to accrual. The pretreatment characteristics of all eligible patients are shown in Table 1.
Treatment Course
The median number of treatment cycles administered among the 11 high-dose patients was 3 (range 1–9). Severe (grade 3–4) hematologic toxicities reported among these patients included thrombocytopenia (82%), neutropenia (82%), leukopenia (64%), and anemia (36%). Neutropenia and thrombocytopenia led to dose reductions in seven of eight patients who received more than one cycle of treatment. Severe nonhematologic toxicities included bleeding, nausea, and vomiting, each occurring in 9% of patients. Among the five patients entered at the lower starting dose, the median number of cycles received was 1 (range: 1–4). The severe (grade 3–4) hematologic toxicities included neutropenia (60%), leukopenia (40%), and thrombocytopenia (20%). Thrombocytopenia and neutropenia led to dose reductions in the two patients who received more than one cycle of treatment. Severe nonhematologic toxicities included jaundice and abdominal pain, each occurring in 20% of patients.
Clinical Outcomes
Two of the eleven patients treated at the higher dose had an objective response (1 CR, 1 PR). The patient with a CR had a response after one cycle of treatment and received a total of four cycles of therapy after presenting with upper abdominal seeding from a ruptured tumor. This patient required a 25% dose reduction after each cycle of therapy due to severe neutropenia and thrombocytopenia. Treatment was discontinued after the fourth cycle due to toxicity. This patient continues in a CR more than 7 years after completing treatment. The second patient had a dose reduction of 25% after the first cycle of therapy due to neutropenia. A response was noted after two cycles at the reduced dose and continued to receive treatment for another six cycles despite three additional dose reductions for neutropenia. The duration of this patient’s response lasted 12 months. None of the patients at the lower dose level had a response. The median progression-free survival time is 20 weeks among those starting at the higher dose and 6.6 weeks in those starting at the lower dose. The median survival time is 11.4 and 9 months for those receiving the higher and lower starting doses, respectively.
Discussion
KW-2189, a novel antitumor antibiotic derived from Streptomyces, has shown promising activity in preclinical models of HCC. This paper reports the first results of a clinical trial of KW-2189 in patients with HCC. Two responses were seen in the 16 patients enrolled in this trial, including one patient with a sustained CR. Despite initial evidence of potential benefit the trial was closed early due to significant and prolonged hematologic toxicity.
Only a limited number of clinical trials with DNA minor groove-binding agents have been reported. Preclinical studies with CC-1065 showed it to be extremely potent and to have lethal delayed toxicity limiting further development of the agent. Subsequently analogs of CC-1065, including adozelesin, bizelesin, and carzelesin, were developed and have been evaluated in phase I-II clinical trials. [17–25] Hematologic toxicity, particularly neutropenia and thrombocytopenia, was dose limiting in the phase I trials. [18, 19, 21, 22, 24, 25] The onset of hematologic toxicity tends to be delayed and prolonged. Similar findings were noted in the phase I trials with KW-2189. [13, 14] In the current trial of patients with HCC, grade 3–4 neutropenia and thrombocytopenia resulted in a dose reduction, but continued to be a problem at the lower dose. The trial was therefore closed before completion of the planned accrual with problems noted in other phase II trials of KW-2189 and CC-1065 analogs. [17, 23, 26, 27] As with other phase I and II trials, nonhematologic toxicity was uncommon.
Based on the results of this clinical trial, it appears there may be a potential role for DNA minor groove-binding agents in the treatment of HCC. However, the toxicity of KW-2189, when given based on the schedule used this trial, precludes further trials of this agent. The preclinical activity of KW-2189 and other DNA minor-groove-binding agents suggest that this class of agents may have promising activity if their hematologic toxicity can be appropriately managed.
References
Mor E, Kaspa RT, Sheiner P, Schwartz M. Treatment of hepatocellular carcinoma associated with cirrhosis in the era of liver transplantation. Ann Intern Med. 1998;129:643–53.
Simonetti RG, Liberati A, Angiolini C, Pagliaro L. Treatment of hepatocellular carcinoma: a systematic review of randomized controlled trials. Ann Oncol. 1997;8:117–36.
Ichimura M, Ogawa T, Katsumata S, Takahashi K-I, Takahashi I, Nakano H. Duocarmycins, new antitumor antibiotics produced by Streptomyces; producing organisms and improved production. J Antibiotics. 1991;44:1045–53.
Ichimura M, Ogawa T, Takahashi K-I, Kobayashi E, Kawamoto I, Yasuzawa T, et al. Duocarmycin SA, a new antitumor antibiotic from Streptomyces sp. J Antibiotics. 1990;43:1037–8.
Ogawa T, Ichimura M, Katsumata S, Morimoto M, Takahashi K. New antitumor antibiotics, duocarmycins B1 and B2. J Antibiotics. 1989;42:1299–301.
Takahashi I, Takahashi K-I, Ichimura M, Morimoto M, Asano K, Kawamoto I, et al. Duocarmycin A, a new antitumor antibiotic from Streptomyces. J Antibiotics. 1988;41:1915–7.
Boger DL, Johnson DS. CC-1065 and the duocarmycins: unraveling the keys to a new class of naturally derived DNA alkylating agents. Proc Natl Acad Sci USA. 1995;92:3642–9.
Okamoto A, Asai A, Saito H, Okabe M, Gomi K. Differential effect of duocarmycin A and its novel derivative DU-86 on DNA strand breaks in HeLa S3 cells. Jpn J Cancer Res. 1994;85:1304–11.
Hurley LH, Reynolds VL, Swenson DH, Petzold GL, Scahill TA. Reaction of the antitumor antibiotic CC-1065 with DNA: structure of a DNA adduct with DNA sequence specificity. Science. 1984;226:843–4.
Yasuzawa T, Muroi K-I, Ichimura M, Takahashi I, Ogawa T, Takahashi K, et al. Duocarmycins, potent antitumor antibiotics produced by Steptomyces sp. structures and chemistry. Chem Pharm Bull. 1995;43:378–91.
Kobayashi E, Okamoto A, Asada M, Okabe M, Nagamura S, Asai A, et al. Characteristics of antitumor activity of KW-2189, a novel water-soluble derivative of duocarmycin, against murine and human tumors. Cancer Res. 1994;54:2404–10.
Adams EG, Badiner GJ, Bhuyan BK. Effects of U-71,184 and several other CC-1065 analogues on cell survival and cell cycle of Chinese hamster ovary cells. Cancer Res. 1988;48:109–16.
Alberts SR, Erlichman C, Reid JM, Sloan JA, Ames MM, Richardson RL, et al. Phase I study of the duocarmycin semisynthetic derivative KW-2189 given daily for five days every six weeks. Clin Cancer Res. 1998;4:2111–7.
Abbruzzese J, Madden T, Newman R. Phase I clinical and pharmacokinetic trial of KW2189 in patients with solid tumors (meeting abstract). Proc Annu Meet Am Assoc Cancer Res. 1996;37:A1138.
Fleming TR. One-sample multiple testing procedure for phase II clinical trials. Biometrics. 1982;38:143–51.
Therneau T, Weiand H, Chang M. Optimal designs for a grouped sequential binomial trial. Biometrics. 1990;46:771–81.
Cristofanilli M, Bryan WJ, Miller LL, Chang AY, Gradishar WJ, Kufe DW, et al. Phase II study of adozelesin in untreated metastatic breast cancer. Anti-Cancer Drugs. 1998;9:779–82.
Burris HA, Dieras VC, Tunca M, Earhart RH, Eckardt JR, Rodriguez GI, et al. Phase I study with the DNA sequence-specific agent adozelesin. Anti-Cancer Drugs. 1997;8:588–96.
Foster BJ, LoRusso PM, Poplin E, Zalupski M, Valdivieso M, Wozniak A, et al. Phase I trial of Adozelesin using the treatment schedule of daily x5 every 3 weeks. Invest New Drugs. 1996;13:321–6.
Shamdas GJ, Alberts DS, Modiano M, Wiggins C, Power J, Kasunic DA, et al. Phase I study of adozelesin (U-73,975) in patients with solid tumors. Anti-Cancer Drugs. 1994;5:10–4.
Pitot HC, Reid JM, Sloan JA, Ames MM, Adjei AA, Rubin J, et al. A Phase I study of bizelesin (NSC 615291) in patients with advanced solid tumors. Clin Cancer Res. 2002;8:712–7.
Schwartz GH, Patnaik A, Hammond LA, Rizzo J, Berg K, Von Hoff DD, et al. A phase I study of bizelesin, a highly potent and selective DNA-interactive agent, in patients with advanced solid malignancies. Ann Oncol. 2003;14:775–82.
Pavlidis N, Aamdal S, Awada A, Calvert H, Fumoleau P, Sorio R, et al. Carzelesin phase II study in advanced breast, ovarian, colorectal, gastric, head and neck cancer, non-Hodgkin's lymphoma and malignant melanoma: a study of the EORTC early clinical studies group (ECSG). Cancer Chemother Pharmacol. 2000;46:167–71.
Awada A, Punt CJ, Piccart MJ, Van Tellingen O, Van Manen L, Kerger J, et al. Phase I study of Carzelesin (U-80,244) given (4-weekly) by intravenous bolus schedule. Brit J Cancer. 1999;79:1454–61.
van Tellingen O, Punt CJ, Awada A, Wagener DJ, Piccart MJ, Groot Y, et al. A clinical pharmacokinetics study of carzelesin given by short-term intravenous infusion in a phase I study. Cancer Chemother Pharmacol. 1998;41:377–84.
Markovic SN, Suman VJ, Vukov AM, Fitch TR, Hillman DW, Adjei AA, et al. Phase II trial of KW2189 in patients with advanced malignant melanoma. Am J Clin Oncol. 2002;25:308–12.
Small EJ, Figlin R, Petrylak D, Vaughn DJ, Sartor O, Horak I, et al. A phase II pilot study of KW-2189 in patients with advanced renal cell carcinoma. Invest New Drugs. 2000;18:193–7.
Acknowledgement
This study was conducted as a trial of the North Central Cancer Treatment Group and Mayo Clinic and was supported in part by Public Health Service grants CA-25224, CA-37404, and CA-60276 from the National Cancer Institute Department of Health and Human Services.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alberts, S.R., Suman, V.J., Pitot, H.C. et al. Use of KW-2189, a DNA Minor Groove-Binding Agent, in Patients with Hepatocellular Carcinoma: A North Central Cancer Treatment Group (NCCTG) Phase II Clinical Trial. J Gastrointest Canc 38, 10–14 (2007). https://doi.org/10.1007/s12029-007-9007-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-007-9007-6