
Abstract
Background/Objective
Catheter-associated urinary tract infections (CAUTIs) account for 25% of all hospital-acquired infections. Neuro-critically ill patients are at 2–5 times greater risk of developing CAUTI because of increased use of indwelling urinary catheters due to neurogenic urinary retention. Despite the heightened risk of CAUTI occurrence for the neuro-critically ill, there is little data on specific characteristics of CAUTIs and risk factors among this population. The aim of this study was to identify characteristics and risk factors associated with CAUTI development in the neuro-critical patient population.
Methods
In this retrospective single-center case–control study in a tertiary care dedicated 30-bed neuroICU, approximately 3 controls (exact ratio—3.2) were randomly selected for each CAUTI case between January 1st, 2016 and December 31st, 2018. Demographic, clinical and laboratory data were collected, including prospectively collected data pertaining to urinary and bowel function. Descriptive and multivariate logistic regression analysis was conducted to identify common patient characteristics, CAUTI risk factors and duration from catheterization to developing a CAUTI (Time-to-CAUTI).
Results
Of 3045 admissions during the study period, 1045 (34.30%) had a urinary catheter at some point during their admission. Of those, 45 developed a CAUTI, yielding a CAUTI incidence rate of 1.50%, corresponding to 4.49 infections/1000 catheter days. On average, CAUTI patients were older as compared to controls (66.44 years of age vs 58.09 years; p < 0.0001). In addition to old age, other risk factors included female gender (75.60% female vs 24.20% males in case group, p < 0.0001), increased neuroICU length of stay (18.31 in cases vs. 8.05 days in controls, p = 0.0001) and stool incontinence (OR = 3.73, p = 0.0146). CAUTI patients more often carried a primary diagnosis of SAH, and comorbidities of hypertension (HTN), vasospasm and diabetes. Time-to-CAUTI was 6 days on average, with an earlier peak for patients requiring two or more catheter placements. Presence of stool incontinence was significantly associated with CAUTI occurrence.
Conclusion
Stool incontinence, older age, female sex, longer neuroICU LOS and presence of comorbidities such as HTN and diabetes were associated with CAUTI development in the neuro-critically ill population. Average Time-to-CAUTI after catheter placement was 6 days with earlier occurrence if more frequent catheterizations. Colonization of urinary catheters without infection might contribute to CAUTI diagnosis. Prospective research is needed to determine impact of prevention protocols incorporating these factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Healthcare-associated infections (HAI) greatly complicate patients’ hospital course and outcomes by increasing infection-related resource utilization, morbidity and mortality [1]. HAI’s affect 3.2% of the total patient population, and urinary tract infections (UTIs) are the most common form accounting for 40% of HAI reported to the National Healthcare Safety Network (NHSN) [2]. Among intensive care unit (ICU) patients, the overall rate of HAI is higher and estimated to be 15%, with catheter-associated UTI (CAUTI) accounting for approximately 25% [3]. Patients admitted to a neuroICU are at 2–5 times greater risk for CAUTIs due to neurogenic urinary retention and a resulting higher frequency of indwelling urinary catheters [4]. Despite the risks that CAUTIs pose specifically to the neuro-critically ill population, apart from the presence of an indwelling urinary catheter, there is little data to guide care teams on possible risk factors for CAUTIs in this subspecialty population. Identifying neuro-specific patient characteristics for susceptibility to CAUTI can serve as a foundation for predictive models that can help evaluate, control and eliminate HAIs and potentially improve patient outcomes, work efficiency and minimize related hospital costs.
The purpose of this study was to determine who among urinary-catheterized neuro-critically ill patients developed a CAUTI, when they developed it, and to evaluate the patient’s characteristics for commonalities and/or clinical traits, with the ultimate aim to gain insight on neuro-specific patient characteristics for susceptibility to CAUTI that would serve as a foundation for predictive models to decrease CAUTI occurrence in this population.
Methods
In this case-control study, we retrospectively reviewed patient characteristics and diagnoses of all patients over the age of 18 admitted to a 30-bed dedicated neuroICU of a single tertiary, level-one trauma and Academic Medical Center located in the Southeastern USA, who developed a CAUTI between January 1st, 2016 and December 31st, 2018. We randomly selected three neuroICU control patients per CAUTI case (144 catheterized controls, ratio control: case 3.2) and matched those to the cases using the following inclusion criteria: those who received an indwelling urinary catheter but did not develop a CAUTI within the study period. The institution’s Electronic Health Records (EHR) data were used, in order to obtain a relatively large comparison group as well as controlling for selection bias. During the study period, all case data (45 cases) were prospectively collected during daily urine-catheter-utilization rounds by the unit-based advanced practice nurses, eliminating recall bias. The institution’s EHR was also used to retrospectively collect control data, as well as cross-reference case data to ensure completeness and accuracy.
Using standard Centers for Disease Control and Prevention (CDC) and the National Health Surveillance Network (NHSN) definitions, a CAUTI was defined as a quantitative culture containing ≥ 105 colony forming units (CFU)/mL of one or two microorganisms in a patient with an indwelling urinary catheter in place for more than 2 consecutive days with one of these four signs or symptoms: (1) fever (> 38.0 °C), (2) suprapubic tenderness, (3) costovertebral angle pain and (4) costovertebral angle tenderness [5]. If more than two types of microorganisms were isolated, the sample was considered to be contaminated [6].
Demographic, clinical and laboratory data were collected prospectively during daily rounds. Clinical data included the following seven components: (1) patient diagnosis (1a) primary diagnosis and (1b) secondary diagnosis, (2) length of stay (LOS; 2a) hospital LOS (HLOS) and (2b) neuroICU LOS, (3) catheterization details (3a) catheter location and (3b) catheter timing, (4) in-indwelling urinary catheter details (4a) catheter number and (4b) catheter days, (5) urinary analysis (UA) details (5a) UA number and (5b) UA timing, (6) urinary culture details, (7) stool incontinence details (7a) number of incontinence episodes (7b) incontinence timing and (7c) fecal management system (FMS) use details and (8) antibiotic use details. The detailed culture reports for CAUTI cases with positive culture were collected from the infection control (IC) department using the TheraDoc® database.
The study was approved by the local Institutional Review Board (IRB201701469).
Data Analysis
Descriptive data analysis and summary statistics were used to describe the quantitative variables. Frequency tables were used to describe the categorical variables (patient diagnosis, gender, UA details, urinary culture details, stool incontinence, FMS use). Additional Student’s t-tests were conducted to assess differences in risk factors between cases and controls. Univariate and multivariate logistic regression models were created using variables collected in both cases and controls dataset (age, gender, HLOS, neuroICU LOS, primary diagnoses and presence of stool incontinence) to find the quantitative impact of these variables on the odds of getting a CAUTI infection in the neuro-critically ill population. The age variable was further stratified into four groups: 18–40 years, 41–60 years, 61–80 years and 81–100 years. Hospital LOS and neuroICU LOS were further stratified into two groups based on the mean for HLOS and research set benchmark for neuroICU LOS (HLOS > 22 and < 22 days; neuroICU LOS > 10 and < 10 days). The probability of < 0.05 was used as the minimum level of significance. Data analysis was conducted using SAS™ software version 9.4 (SAS Institute, Cary NC), GraphPad prism and Microsoft Excel 2019.
Results
There were a total of 3045 admissions to the neuroICU during the study period. Of those, 1045 (34.31%) patients had an indwelling urinary catheter during at least a part of their neuroICU stay. 45 patients developed a CAUTI. The average CAUTI rate defined as number of infections/1000 catheter days in the neuroICU for this study period was 5.34 (2016 calendar year), 5.69 (2017 calendar year) and 2.20 (2018 calendar year). Detailed and monthly CAUTI rate showing number of infections per 1000 catheter days is shown in Supplementary Table 2. CAUTI incidence in the entire neuro-critically ill population during the study period was 1.48% and CAUTI incidence in the catheterized neuro-critically ill population was 4.30%. The baseline characteristics of our study population are presented in Table 1. The mean age of the CAUTI patients was 66.44 years versus 58.09 years in the control group (p <0.0001). There were significantly more females among cases than controls (p < 0.0001).
Primary and Secondary Diagnosis
Distribution of the primary diagnosis across all patients is shown in Table 1. The most common primary diagnosis in the case group was subarachnoid hemorrhage (SAH). More than one-third of the cases (35.56%) had SAH as the primary diagnosis compared to 6.67% patients in the control group (p = 0.0005). In contrast, the most common primary diagnosis in the control group was ischemic stroke, 19.44%, compared to 11.11% of the CAUTI cases (p = 0.1810). Hypertension (HTN) (18, 40.00%), vasospasm (8, 17.78%) and diabetes (6, 13.33%) were the most common secondary diagnosis associated with cases, whereas the most common secondary diagnosis found in the controls was Cerebral Edema (31, 21.53%).
Length of Stay
The average HLOS for CAUTI cases was 22.20 days versus 12.75 days among controls (p < 0.0001). Similarly, the average NLOS was 18.21 days for CAUTI cases versus 8.05 days for controls (p < 0.0001) (Table 1).
Time-to-CAUTI
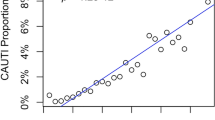
Time-to-CAUTI was analyzed for neuroICU stay and for duration of catheter in place (Figs. 1, 2). The average time from neuroICU admission to acquiring the CAUTI was 11.5 days (SD ± 7.53), with 31.11% of CAUTI cases being acquired during days 6–10 of their neuroICU admission. The average time from catheter insertion to acquiring the CAUTI was 6.2 days (range 2–25, SD ± 4.39). While half (53.30%) of CAUTI cases had one indwelling urinary catheterization during their hospital stay, 46.70% had ≥ 2 indwelling urinary catheterizations. Of these patients with > 2 indwelling catheters, 15 (33.30%) patients acquired a CAUTI by day 5 of neuroICU admission, while 3 patients (6.67%) acquired a CAUTI between 6 and 10 days of neuroICU admission.

Number of Foley days to CAUTI infection

Number of admission days to CAUTI infection
The average catheter days for the CAUTI cases were 7.5 days (range 2–25 days; SD + 5.01). Almost one-third (31.00%) of the CAUTI cases had longer than average catheter days and 13% of these cases had SAH as their primary diagnosis.
Univariate logistic models for the risk factors detailed in the methods section revealed that age group 61-80 years (OR = 11.19, p = 0.0210), female gender (OR = 4.21, p = 0.0002), HLOS > 22 days (OR = 4.81, p < 0.0001), NLOS > 10 days (OR = 12.03, p < 0.0001), primary diagnosis of SAH (OR = 8.27, p < 0.0001) and presence of stool incontinence (OR = 9.60, p < 0.0001) were significant risk factors for CAUTI development among neuroICU patients. On multivariate regression analysis, significant risk factors were: age group of 61-80 years (OR = 10.94, p = 0.0362), female gender (OR = 4.01, p = 0.0031), neuroICU LOS > 10 days (OR = 6.09, p = 0.0010) and presence of stool incontinence (OR = 3.73, p = 0.0146). Detailed results of multivariate analysis are included in the Supplementary Table (Table S1). Further analysis was conducted to understand the interaction between SAH, HLOS and NLOS. The logistical models showed that patients diagnosed with SAH were 7.4 times more likely to have HLOS > 22 days (p < 0.0001) and 50.26 times more likely to have ICU LOS > 10 days (p = 0.002).
Urine Analysis (UA) & Urine Culture Details
Two-thirds (64.44%) of cases received a UA on admission to the hospital out of which (53.33%) had a negative result. The most common reason for ordering a urine culture in patients was fever (53.33%). The most common microorganism in urine cultures was E. coli. The detailed results of urinalysis, reasons for ordering a urine culture, and urine culture microbiology results are shown in Table 2.
Stool Incontinence Details
Given the mixed microbiology seen in positive urine culture, the number of stool incontinence episodes within 3 days of infection were also explored. Among the case group, majority of patients (84.44%) had stool incontinence compared to one-third (36.11%) patients in control group (p < 0.0001). In the case group, more than half patients (57.78%) had greater than three stool incontinence episodes compared to less than one-third (28, 19.44%) patients in the control group (p < 0.0001) (Table 3). Out of all patients, where (FMS) was indicated, in case group (21, 80.76%) patients had an FMS placed compared to (19, 67.85%) eligible patients in the control group. Reasons for not having FMS varied from not clinically indicated per institutional guidelines (greater than 3 loose/watery stools in a 24-h period) or it was clinically contraindicated due to patient conditions (i.e., increased intracranial pressure, rectal tears or previous rectal surgery).
Antibiotic Use Details
The prevalence of antibiotic use (prior to a CAUTI episode in cases and during overall stay in controls) was assessed. We found significant difference in antibiotic use among both groups (Cases: 46.67%; controls: 29.81%; p = 0.04). The most common antibiotic used in the case group prior to a CAUTI episode was ampicillin (18.44%), whereas in the control group most common antibiotic used was cefepime (26.27%). This variable was incorporated in the multivariate logistic regression model to assess its impact on overall CAUTI probability; however, antibiotic use did not independently predict CAUTI development (OR = 1.29, p = 0.58).
Discussion
In this three-year long, case–control, single-center study of CAUTI in the neuroICU, we found that presence of stool incontinence, in addition to age group of 61–80 years, female gender, and NLOS > 10 days, are significantly associated with CAUTI development in neuro-critically ill patients. Other important risk factors identified were primary diagnosis of SAH, secondary diagnosis of HTN and diabetes, and occurrence of vasospasm. Furthermore, we found that presence of stool incontinence was significantly more prevalent in the CAUTI group. With regard to time to occurrence of CAUTI, the average time-to-CAUTI was only 6 days, with patients who required more than one indwelling urinary catheter placement within the first 5 days of admission contributing to an early peak of CAUTI occurrence. Antibiotic use prior to CAUTI development did not present an independent risk or protective factor.
The relationship between length of stay, age and gender predominance with risk for CAUTI [7] has been described in previous studies [8, 9] and our study specific to the neuroICU confirms these findings. HTN and diabetes were comorbidities identified as possible risk factors for CAUTI. Due to the effect of diabetes on the immune system, this might not be a surprising finding. For HTN, the association is less clear, and interpretation may be hampered by the lack of details about the coding of this diagnosis in our population, as well as lack of data on baseline level of control of HTN. For SAH, our data are in line with previous findings for SAH patients [10] indicating that SAH diagnosis itself may not increase CAUTI risk but rather increase the risk due to the prolonged hospital stay, and prolonged indwelling urinary catheter utilization for strict management of intake and output to achieve euvolemia especially in the setting of cerebral vasospasm. Similar results were found in the referenced previous study showing a CAUTI rate of 20.7/1000 catheter days [10]. Our data support the call for heightened attention in this specific diagnosis group, and future adjustment of practice patterns and catheter utilization in patients with SAH.
Of our findings, the presence of stool incontinence, the timing of CAUTI and the early risk for patients receiving more than one indwelling urinary catheter present previously unknown factors and are of specific relevance. More than 80% of our case group had the condition of stool incontinence, associated most often with neurogenic bowel and/or medication-related diarrhea oftentimes induced to counter constipation or even ileus. Generally, the national nursing guidelines for patients with stool incontinence suggest fecal containment, using either external rectal pouch or internal FMS, after three episodes of loose/watery stools in a 24h period [11]. Based on our data, which show an association between stool incontinence and CAUTI occurrence, this general recommendation may not be optimal or feasible for neuro-critically ill patients requiring an indwelling urinary catheter, especially if at risk for CAUTI. Earlier stool containment might be a possibility to reduce CAUTI rates.
Our data on time-to-CAUTI are an important new addition to the slim body of knowledge on CAUTIs in the neuroICU population. While in previous data, longer LOS has been found as a factor associated with CAUTI [10], our data show that there is a proportion of patients who develop a CAUTI early on, with repeated indwelling urinary catheter placement as risk factor. This may aid the practicing clinician not only in exertion of vigilance, but also perhaps suggest proactive rather than reactive stool containment, and avoidance of indwelling urinary catheter placement even more in this subset.
Another consideration is that with presence of an indwelling urinary catheter, chemical inflammation will occur with increased white blood cell (WBC) count in a UA, which does not necessarily indicate infection. The most common symptoms for ordering a urine culture in our study that eventually led to CAUTI diagnosis were non-specific, such as fever (53%) and increased WBC count (18%)—which often present in the neuro-critically ill population in absence of infection [12, 13]. Colonization of catheters after 6–7 days, especially in presence of stool incontinence, is another problem not well studied. In our study, several subjects had a CAUTI by definition, but a negative UA, suggesting that these were colonized specimens versus true active infections, despite using NSHN definitions. Adjustment of culturing practices might assist to avoid classification of a colonized catheter as acute infection and initiation of antibiosis where it might not be required.
Strengths and Limitations of the Study
By using standardized, prospective nursing indwelling urinary catheter rounding data, our data are free of recall bias. The study design as case–control allowed for comparison of patients without CAUTI to those with CAUTI development in the population of the same unit, hence eliminating potential impact of unit-specific practice on catheterized patients. Further, CAUTI rate vs. CAUTI incidence is typically the reported metric for CAUTI. However, this rate metric becomes skewed as the urinary catheter utilization decreases, a primary intervention in CAUTI reduction. As our catheter utilization reduced below 30% utilization, we found it helpful to also track CAUTI incidence (i.e., the number of raw infections) as a specific metric for infection patterns. No selection bias was present in the study as the controls were selected from the same population as the cases and their selection was independent of the presence or absence of risk factors of interest (e.g., age, gender, diagnosis, hospital LOS, indwelling urinary catheter days, frequency of catheterization, etc.). Limitations included local practice patterns of indwelling urinary catheter insertion including frequency of use, and nursing protocol of insertion, inability to comment on presence of urinary retention versus urinary incontinence as a possible factor that could reduce catheter utilization, and lack of granularity in our data to gain more insight into specific effects of sub-diagnoses such as vasospasm and cerebral edema.
Conclusion
Presence of stool incontinence, older age, female sex, longer neuroICU LOS, HTN and diabetes, were identified as risk factors for CAUTI development in the neuro-critically ill population. Urine culturing may yield colonization with bacterial growth despite negative urinalysis rather than reflect true infection. Average time-to-CAUTI was 6 days, with a subset of CAUTIs occurring early during the hospital course and linked to repeated catheter placements. Additional prospective and multicenter research is needed to understand the impact these clinical characteristics have in order to define why the neuro-critical care population is especially vulnerable, and to develop appropriate prevention protocols to avoid CAUTI in neuro-critical care patients.
References
Burgmann H, Hiesmayr JM, Savey A, Bauer P, Metnitz B, Metnitz PG. Impact of nosocomial infections on clinical outcome and resource consumption in critically ill patients. Intensive Care Med. 2010;36:1597–601.
Haque M, Sartelli M, McKimm J, Abu BM. Health care-associated infections: an overview. Infect Drug Resist. 2018;11:2321–33.
Iordanou S, Middleton N, Papathanassoglou E, Raftopoulos V. Surveillance of device associated infections and mortality in a major intensive care unit in the Republic of Cyprus. BMC Infect Dis. 2017;17:607.
Albayram O, MacIver B, Mathai J, et al. Traumatic Brain Injury-related voiding dysfunction in mice is caused by damage to rostral pathways, altering inputs to the reflex pathways. Sci Rep. 2019;9:8646.
Stone ND, Ashraf MS, Calder J, et al. Surveillance definitions of infections in long-term care facilities: revisiting the McGeer criteria. Infect Control Hosp Epidemiol. 2012;33:965–77.
Temiz E, Piskin N, Aydemir H, et al. Factors associated with catheter-associated urinary tract infections and the effects of other concomitant nosocomial infections in intensive care units. Scand J Infect Dis. 2012;44:344–9.
Al-Hazmi H. Role of duration of catheterization and length of hospital stay on the rate of catheter-related hospital-acquired urinary tract infections. Res Rep Urol. 2015;7:41–7.
Yan T, Liu C, Li Y, Xiao W, Li Y, Wang S. Prevalence and predictive factors of urinary tract infection among patients with stroke: a meta-analysis. Am J Infect Control. 2018;46:402–9.
Letica-Kriegel AS, Salmasian H, Vawdrey DK, et al. Identifying the risk factors for catheter-associated urinary tract infections: a large cross-sectional study of six hospitals. BMJ Open. 2019;9:e022137.
Hagerty T, Kertesz L, Schmidt JM, et al. Risk factors for catheter-associated urinary tract infections in critically ill patients with subarachnoid hemorrhage. J Neurosci Nurs. 2015;47:51–4.
Wound O, Continence Nurses S, Guideline Development Task F. WOCN Society Clinical Guideline: management of the adult patient with a fecal or urinary ostomy—an executive summary. J Wound Ostomy Continence Nurs 2018;45:50–8.
Busl KM. Healthcare-associated infections in the neurocritical care unit. Curr Neurol Neurosci Rep. 2019;19:76.
Marik PE. Fever in the ICU. Chest. 2000;117:855–69.
Funding
There was no dedicated financial support for this study.
Author information
Authors and Affiliations
Contributions
Conception of the study done by KP, AL and KMB. Data collection was done by KP, AV, AQ, AL, JH, AF and AS. Data interpretation was done by KP, AV, JH, JBL and KMB. Drafting of the article was done by KP, AV and AS. Data analysis was done by AV, AQ, AF and AS. Critical revision of the manuscript was done by AL, JH, JBL and KMB. Design of the analysis and design of the study was done by AF and KMB respectively. All authors approved the final version of this manuscript for publication.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest
Ethical Approval/Informed Consent
This manuscript complies with all instructions to authors. This study adheres to ethical guidelines and has approval from the local Institutional Review Board (IRB201701469).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Perrin, K., Vats, A., Qureshi, A. et al. Catheter-Associated Urinary Tract Infection (CAUTI) in the NeuroICU: Identification of Risk Factors and Time-to-CAUTI Using a Case–Control Design. Neurocrit Care 34, 271–278 (2021). https://doi.org/10.1007/s12028-020-01020-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-020-01020-3