
Abstract
Background
Elevated intracranial pressure (ICP) is an important cause of death following acute liver failure (ALF). While invasive ICP monitoring (IICPM) is most accurate, the presence of coagulopathy increases bleeding risk in ALF. Our objective was to evaluate the accuracy of three noninvasive ultrasound-based measures for the detection of concurrent ICP elevation in ALF—optic nerve sheath diameter (ONSD) using optic nerve ultrasound (ONUS); middle cerebral artery pulsatility index (PI) on transcranial Doppler (TCD); and ICP calculated from TCD flow velocities (ICPtcd) using the estimated cerebral perfusion pressure (CPPe) technique.
Methods
In this retrospective study, consecutive ALF patients admitted over a 6-year period who underwent IICPM as well as measurement of ONSD, TCD-PI or ICPtcd were included. ONSD was measured offline by a blinded investigator from deidentified videos. The ability of highest ONSD, TCD-PI, and ICPtcd to detect concurrent invasive ICP > 20 mmHg was assessed using receiver operating characteristic (ROC) curves. The ROC area under the curve (AUC) was calculated with 95% confidence interval (95% CI) and evaluated against the null hypothesis of AUC = 0.5. Noninvasive measures were also evaluated as predictors of in-hospital death.
Results
Forty-one ALF patients were admitted during the study period. In total, 27 (66%) underwent IICPM, of these, 23 underwent ONUS and 21 underwent TCD. Eleven out of 23 (48%) patients died (two from intracranial hypertension). Results of ROC analysis for detection of concurrent ICP > 20 mmHg were as follows: ONSD AUC = 0.59 (95% CI 0.37–0.79, p = 0.54); TCD-PI AUC = 0.55 (95% CI 0.34–0.75, p = 0.70); and ICPtcd AUC = 0.90 (0.72–0.98, p < 0.0001). None of the noninvasive measures were significant predictors of death.
Conclusions
In patients with ALF, neither ONSD nor TCD-PI reliably detected concurrent ICP elevation on invasive monitoring. Estimation of ICP (ICPtcd) using the TCD CPPe technique was associated with concurrent ICP elevation. Additional studies of TCD CPPe in larger numbers of ALF patients may prove worthwhile.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute liver failure (ALF), defined by the onset of hepatic encephalopathy and coagulopathy within 26 weeks of illness onset, may be associated with severe cerebral edema and raised intracranial pressure (ICP) [1]. Elevated ICP is an important cause of death and disability in ALF [1,2,3]. Cerebral edema is hypothesized to occur as a result of ammonia accumulating in glial cells, which then is converted to glutamine, resulting in an osmotic gradient and cellular edema [2, 4]. Vasodilatation and cerebral hyperperfusion may also play a role [2, 4]. Monitoring of ICP may permit therapeutic intervention before cerebral herniation and devastating brain injury occurs. Invasive ICP monitoring (IICPM) remains the gold standard for the measurement of ICP and frequently reveals otherwise unsuspected intracranial hypertension. We recently reported our experience with protocol-based use of IICPM in ALF [5]. Sustained intracranial hypertension was detected in 13/24 (54%) comatose ALF patients, while 5/24 (21%) required the highest therapeutic intensity level (TIL) for control of ICP, including the use of barbiturate coma or therapeutic hypothermia. However, ALF patients are coagulopathic by definition and are at risk of intracranial hemorrhage following monitor insertion [6, 7].
Noninvasive monitoring of ICP may therefore be especially useful in this disease. Two promising ultrasound techniques for ICP assessment are optic nerve ultrasound (ONUS) and transcranial Doppler (TCD). Similar to the mechanism that results in papilledema, elevated ICP is transmitted through the subarachnoid space and results in distension of the optic nerve sheath (ONS) [8]. While papilledema may take hours or days to develop, distension of the ONS may occur rapidly following an ICP elevation [8]. Sonographic measurement of the ONS diameter (ONSD) may, therefore, detect ICP elevation [9,10,11,12,13,14,15]. The optimal ONSD threshold to detect raised ICP has greatly varied between studies, raising concerns about the clinical value of this technique. In addition to ONUS, ICP may also be noninvasively assessed using two different TCD techniques. The technique described by Czosnyka et al. involves estimation of the cerebral perfusion pressure (CPPe), and thereby the ICP (ICPtcd), through measurement of cerebral blood flow velocities [16]. Elevated ICP may also be reflected in the Gosling pulsatility index (PI), which is the ratio of the difference between the peak-systolic and end-diastolic velocities and the mean flow velocity recorded on TCD [17]. These ultrasound-based measures may be the most promising as screening tools to exclude the presence of intracranial hypertension at the time of assessment.
Our primary objective was to examine the ability of 3 ultrasound-based measures—ONSD, ICPtcd, and TCD-PI—to exclude a concurrent ICP elevation on gold-standard measurement with IICPM, in the setting of ALF. Secondary objectives included the assessment of the accuracy of these measures for concurrent ICP elevation and to examine these measures as predictors of mortality in ALF.
Methods
All patients entered in our institutional ALF-ICP database between 2011 and 2017 who underwent IICPM as well as a noninvasive assessment (ONUS or TCD) were eligible. Additional inclusion criteria were age > 12 years, use of IICPM and performance of at least one noninvasive assessment concurrently with IICPM. Subjects were excluded when all available noninvasive measurements were found to be of suboptimal quality on blinded review.
ALF-ICP Database
In 2011, a written protocol for the use of IICPM in ALF was put in place at our institution. This included criteria for patient selection, steps to reverse coagulopathy prior to insertion, timing of insertion, and a requirement for computed tomography (CT) imaging in all patients prior to and following monitor insertion. In view of the risk involved, a quality control database was created to track complications, the frequency with which intracranial hypertension requiring therapy occurred and patient outcomes. The neurosurgery and neurointensive care teams were routinely consulted to assess eligibility for IICPM in ALF patients admitted to the intensive care unit (ICU). All such patients were entered into the ALF-ICP database. Prospectively entered data included demographics, baseline variables, CT imaging details, use of IICPM, data on sustained ICP elevations at any time, therapeutic measures directed at ICP control, outcome at hospital discharge, and follow-up information on outcome obtained at subsequent clinic visits up to 6 months. The therapeutic intensity level (TIL-Basic) for control of ICP, as described in traumatic brain injury (TBI), was estimated as shown in Table 1 [18]. A point-of-care ultrasound (POCUS) assessment was routinely performed on these patients, contingent on operator availability. All POCUS findings relevant to ICP assessment were prospectively entered into the database, including ONSD and TCD measurements. We have previously reported our experience with IICPM in ALF using this database [5].
Invasive ICP Monitoring
Protocol criteria for the use of IICPM in ALF included a Glasgow Coma Scale < 9 and West Haven encephalopathy grade 4 [5]. The IICPM protocol excluded patients with an absence of brainstem signs, inability to reverse coagulopathy per protocol and nonsurvivable illness. The protocol for reversal of coagulopathy prior to monitor insertion is shown in Table 2. All patients underwent a noncontrast CT scan of the brain prior to and within a 24-hour following monitor insertion. Sustained intracranial hypertension at any time during the admission was defined as an ICP > 20 mmHg for > 10 min in an hour with the patient at rest. Note that this database entry was distinct from ICP elevation at the time of ultrasound assessment, which was used to validate the noninvasive measurements.
Optic Nerve Ultrasound
All ONUS examinations were performed using a SonoSite™ M-Turbo (SonoSite Inc., Bothell, WA, USA) point-of-care ultrasound machine and a L25 linear array transducer with ophthalmic preset, by neurointensivists who had performed a minimum of 50 examinations and typically performed at least 5–10 examinations per month. The ONUS examination was performed within 24 h of the initial assessment, with the first examination typically performed prior to the insertion of an invasive monitor. Measurement of ONSD was then taken daily, while the patient was in the ICU, as part of a POCUS assessment that also included TCD. Performance of ONUS and TCD was, however, subject to availability of a neurointensivist with expertise in the appropriate examination. The head of bed was maintained between 30 and 45 degrees at the time of the ultrasound evaluation. Video clips of 6–10 s duration were recorded from each eye and bedside ONSD measurement performed from still images in the axial plane only. The sonographer was not blinded to the patient’s ICP at the time of image acquisition and bedside ONSD measurement. All recorded ONUS videos were, however, downloaded in the Digital Imaging and Communications in Medicine format and deidentified for the purposes of this study. An investigator then measured the ONSD from these deidentified videos 3 mm behind the globe using a standard, previously described measurement technique [14]. The ONSD used in this analysis was, therefore, measured offline by an investigator blinded not only to the concurrent invasive ICP, but all of the clinical details of the patient. The ONSD was measured by the blinded investigator from all ONUS videos recorded, while an invasive ICP monitor was in place. The highest among these blinded ONSD measurements was then evaluated against the invasive ICP simultaneously measured at the time of that specific ONUS study, recorded by the sonographer at the time of the examination. Since this was not a prospectively designed diagnostic study unlike some other studies of ONSD [10,11,12,13,], the mean of 3 consecutive measurements could not be obtained. The clinician performing the POCUS assessment did so for clinical purposes and typically recorded only one study of optimal quality from each eye during each session. Criteria for adequate quality of video images prior to measurement of ONSD included clear definition of both margins of both the optic nerve and the optic nerve sheath extending from the posterior margin of the sclera posterior to the globe (Fig. 1).

Optic nerve sheath diameter (ONSD) measurement. Image depicts a magnified view of the posterior globe and retrobulbar region, with the optic nerve (OpN) visible as a linear hypoechoic structure within the optic nerve sheath (OpNS). Caliper A depicts a point 3 mm posterior to the extrapolated posterior scleral border, at which point the ONSD is measured by Caliper B. In this sample image, ONSD is 0.70 cm, concurrent to an invasive intracranial pressure (ICP) of 21 mmHg
Transcranial Doppler
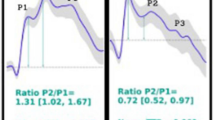
A transcranial color-coded sonography (TCCS) study was typically performed along with ONUS, although not all patients underwent TCCS. The TCCS study was performed using the same ultrasound machine, with a P21 phased-array transducer and transcranial preset. Operators were American Society of Neuroimaging certified in neurosonology and performed approximately 10–30 TCD studies per month. The M1 segment of the middle cerebral artery was evaluated on both sides, using an angle of insonation of no more than 30°. Angle correction was not performed, as is standard practice at our institution, since angle-corrected velocities are consistently higher [19] and have not been as extensively validated against clinical endpoints such as cerebral vasospasm and hyperemia. They are therefore harder to interpret from the standpoint of clinical decision making. Peak-systolic velocity (PSV), end-diastolic velocity (EDV), time-averaged peak velocity (TAPV), and a Gosling were measured in each vessel. The PI was calculated automatically using the formula (PSV-EDV)/TAPV [20]. As with ONUS, the sonographer was not blinded to the patient’s ICP at the time of the examination. Unlike manual measurement of ONSD, however, which was subsequently performed by a blinded investigator, all TCD measurements used in the analysis were automatically derived from the spectral Doppler waveform by the ultrasound machine. The mean arterial pressure (MAP) and invasive ICP simultaneously measured at the time of the TCD examination were recorded by the sonographer. The MAP was measured via a radial or femoral arterial catheter with the transducer leveled to the phlebostatic axis, rather than the tragus. A noninvasive CPPe was then estimated using the formula described by Czosnyka et al [16]. The MAP was then subtracted from the CPPe to obtain the ICPtcd.
The highest PI and ICPtcd recorded in the database while an ICP monitor was in place were evaluated against the simultaneously measured invasive ICP recorded by the sonographer at the time of that specific study.
Outcomes of Interest
The highest recorded ONSD was evaluated exclusively against the invasive ICP measured simultaneously at the time of ONSD measurement, while the highest PI and highest calculated ICPtcd were evaluated against the invasive ICP recorded simultaneously at the time of the specific TCD examination from which these values were derived. Noninvasive assessments prior to or nonconcurrent with IICPM were not included in the analysis. We chose the single highest recorded noninvasive measure in the database for evaluation against the simultaneous gold-standard measurement since our primary goal was to examine the ability of these tests to exclude intracranial hypertension with high confidence (high negative predictive value). We studied the ability of noninvasive techniques to detect a concurrent ICP > 20 mmHg. A secondary outcome was all-cause mortality for the admission.
Management Protocol
Clinical management of ALF was based on a comprehensive institutional ALF protocol based on the recommendations of the ALF study group. While all POCUS findings, including ONSD and TCD measurements, were communicated to the primary clinical team, changes in ICP management were primarily based on IICPM, as per the clinical practice prevalent at the time of this study. All patients received TIL-1 (basic ICU) care (Table 1). Therapy was then escalated as necessary (Table 1) to maintain ICP < 20–25 mmHg and the cerebral perfusion pressure (CPP) > 50–60 mmHg. Hypertonic saline (3% NaCl infusion and 23.4% NaCl bolus dosing) was mostly used for hyperosmolar therapy, in conjunction with a high-sodium dialysate in patients requiring renal replacement therapy. Intracranial hypertension refractory to standard therapy (TIL-4) was managed with a barbiturate coma and/or hypothermia to 32–34 °C using the Arctic Sun® (Medivance Inc., Louisville, CO, USA) external hydrogel device.
Statistical Analysis
Descriptive statistics included a proportion with percentage for categorical variables and median with interquartile range (IQR) for continuous variables. The significance of association between categorical variables was tested using the Chi-square or Fisher’s exact test, as appropriate. The Mann–Whitney U test was used to evaluate the significance of differences in continuous variables between two groups. An intraclass coefficient was calculated, and scatter diagrams plotted, to study agreement between noninvasive (calculated using the TCD CPPe technique) and simultaneously measured invasive CPP as well as ICP. A Bland–Altman plot was constructed to study agreement between simultaneous ICPtcd values and simultaneous ICP measurements obtained via IICPM. Receiver operating characteristic (ROC) curves were constructed to evaluate the ability of ONSD, ICPtcd, and PI to detect concurrent ICP elevation on IICPM, defined as an ICP > 20 mmHg. An area under the curve (AUC) with a 95% CI was calculated for ROC curves and evaluated against the null hypothesis of an AUC = 0.5. If this null hypothesis was rejected (p < 0.05), the optimal value to identify elevated ICP was derived from the ROC curve. A negative predictive value (NPV), sensitivity, specificity, and positive predictive value (PPV) for this value were calculated. This analysis was then repeated for an ICP threshold of > 25 mmHg. All statistical analysis was performed using MedCalc for Windows, version 17.9.7 (MedCalc Software, Ostend, Belgium).
Results
A total of 41 patients with ALF were entered into the database during the period of the study. A total of 27/41 (66%) patients underwent IICPM, of these 21 underwent ONUS and TCD, while two additional patients underwent ONUS alone because of poor transtemporal acoustic windows for TCD examination. Four patients who underwent IICPM did not undergo any ultrasound assessment, because an appropriately trained sonographer was unavailable. The distribution of baseline variables in patients who underwent IICPM and were included in this study (n = 23), as well as the distribution of all variables related to ICP measurement and management (including all noninvasive and invasive measures), is shown in Table 3. Eleven of 23 patients (48%) died; two of these were caused by intracranial hypertension. Eleven (48%) developed sustained ICP elevation at any time. Five (22%) required a TIL > 2; 4 of these required a TIL of 4. As previously reported, only one patient who underwent IICPM suffered any hemorrhage; this was an asymptomatic 5-mm subdural hematoma in a patient who recovered spontaneously without deficit [5].
Optic Nerve Sheath Diameter
At least one video of adequate quality was identified for all 23 patients who underwent ONUS and IICPM. The median highest ONSD was 0.68 (IQR 0.08) in patients with ICP <=20 mmHg on concurrent invasive monitoring and 0.67 (IQR 0.08) in patients with ICP > 20 mmHg (p = 0.53). The ROC for the ability of the highest measured ONSD to detect a concurrent ICP > 20 mmHg on IICPM (Fig. 2) demonstrated an AUC of 0.59 (95% CI 0.37–0.79, p = 0.54). There was no statistically significant difference in the median highest measured ONSD between survivors (0.68 cm, IQR 0.07) and patients who died (0.66 cm, IQR 0.09, p = 0.53).

Receiver operating characteristic (ROC) curve of measured optic nerve sheath diameter (ONSD) for the detection of intracranial pressure (ICP) > 20 mmHg on concurrent invasive ICP monitoring
Transcranial Doppler Pulsatility Index
TCD PI measures were available in 21 patients. The median highest PI was 1.03 (IQR 0.52) in patients with ICP <=20 mmHg on concurrent invasive monitoring and 1.01 (IQR 0.18) in patients with ICP > 20 mmHg (p = 0.77). The ROC for the ability of the highest measured PI to detect a concurrent ICP > 20 mmHg on IICPM demonstrated an AUC of 0.55 (95% CI 0.34–0.75, p = 0.70). There was no statistically significant difference in the median highest measured PI between survivors (1.02, IQR 0.34) and patients who died (1.03, IQR 0.35, p = 0.20).
Transcranial Doppler CPPe/ICPtcd
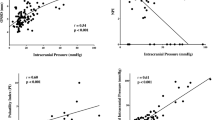
TCD CPPe/ICPtcd measures were available in 21 patients. The median highest ICPtcd was 12 (IQR 9) in patients with ICP <=20 mmHg on concurrent invasive monitoring and 28 (IQR 10) in patients with ICP > 20 mmHg (p = 0.006). The Intraclass Correlation Coefficient for CPP vs CPPe was 0.86 (95% CI 0.67–0.94) and for ICP vs ICPtcd was 0.66 (0.31–0.85), scatter plots in Figs. 3, 4. The Bland–Altman plot of ICPtcd vs concurrent ICP on IICPM is shown in Fig. 5. The ROC for the ability of the highest measured ICPtcd to detect a concurrent invasive ICP > 20 mmHg (Fig. 6) demonstrated an AUC of 0.90 (95% CI 0.72–0.98, p < 0.0001). An ICPtcd > 18.55 mmHg demonstrated a NPV of 100% (95% CI 74–100%), sensitivity of 100% (48–100%), specificity of 81% (58–95%), and PPV 56% (34–75%) for the detection of concurrent ICP > 20 mmHg. ROC analysis for an ICP > 25 mmHg threshold revealed AUC 0.93 (0.76–0.99, p < 0.0001). An ICPtcd > 19 mmHg demonstrated NPV 100% (78–100%), sensitivity 100% (40–100%), specificity 86% (65–97%), and PPV 57% (32–79%) for the detection of concurrent ICP > 25 mmHg. There was no statistically significant difference in the median highest measured ICPtcd between survivors (14 mmHg, IQR 9) and patients who died (17 mmHg, IQR 12, p = 0.80).

Scatter diagram of cerebral perfusion pressure estimated (CPPe) with transcranial Doppler (TCD) using the Czosnyka method versus cerebral perfusion pressure (CPP) measured with invasive monitoring

Scatter diagram of intracranial pressure estimated (ICPtcd) with transcranial Doppler (TCD) using the Czosnyka method versus intracranial pressure (ICP) measured with invasive monitoring

Bland–Altman curve of intracranial pressure (ICP) estimated using transcranial Doppler (ICPtcd) against ICP measured on concurrent invasive monitoring. SD standard deviation

Receiver operating characteristic (ROC) curve of intracranial pressure (ICP) estimated using transcranial Doppler (ICPtcd) for the detection of ICP > 20 mmHg on concurrent invasive ICP monitoring
Discussion
We evaluated the accuracy of noninvasive ultrasound-based techniques for the detection of intracranial hypertension in ALF. Both ONSD and TCD-PI proved inaccurate for the detection of concurrent ICP elevation and did not demonstrate a significant association with mortality. The estimated ICP, using the TCD CPPe method, demonstrated a high NPV for the exclusion of concurrent ICP elevation. Noninvasive estimation of ICP has always had appeal in the setting of ALF, a condition associated with both life-threatening intracranial hypertension and coagulopathy. In a study of 22 pediatric ALF patients in 2000, ONSD predicted mortality [21]. Subsequent studies of ONUS and TCD in ALF have mostly been confined to case reports or limited case series [22,23,24]. It is crucial, however, that any new diagnostic tool for the detection of a life-threatening condition, with therapies that have serious side effects, be validated against the gold standard—in this case, IICPM. Therein lies the challenge in the evaluation of noninvasive ICP measurement tools, since ALF is itself an uncommon disease and relatively few liver centers routinely perform IICPM. This is the only study thus far to have directly evaluated these bedside noninvasive techniques against the gold standard of concurrent invasive measurement in ALF.
The most important finding of our study is that ONSD is inaccurate for the detection of concurrent ICP elevation. ONUS has, perhaps, been the most promising and best studied of the available noninvasive ICP assessment tools. Several investigators, including our group, have reported that ONUS may accurately detect elevated ICP in critically ill patients with neurological illness [9,10,11,12,13,14,15]. The ONUS examinations in this study were performed by individuals with considerable experience with the technique. There are several possible reasons for the discrepancy between these prior studies and the current study. The pathophysiology of elevated ICP in ALF is fundamentally different from the mechanism in hydrocephalus, stroke or TBI. It is also possible that ONUS may not be as accurate for the detection of elevated ICP as some earlier studies have suggested. At least one other study has demonstrated poor correlation between ONSD and measured ICP in TBI [25]. The wide variation in optimal ONSD for the detection of elevated ICP, incomplete blinding in some studies (with the sonographer aware of the patient’s actual ICP, the clinical details leading up the examination or both), limited dynamic range of the measurement, potential influence of artifact, variations in technique, and a possible drop in accuracy in the setting of prolonged or fluctuating ICP elevation have all been reasons to consider ONUS an investigational tool rather than one that is ready for routine clinical use [9,10,11,12,13,14, 26,27,28]. Further prospective studies of ONUS, with multiple different sonographers, more complete blinding, and larger sample size (NCT02618226) are currently underway and may better define its role in clinical practice [29]. Given the very limited accuracy seen in our study, however, ONUS should not currently be used to guide clinical management in the setting of ALF.
The role of TCD in ALF has previously been investigated in small studies [30,31,32,33] and an elevated PI proposed as an indicator of poor outcome [30, 33]. The poor accuracy of TCD-PI for the detection of elevated ICP and prediction of outcomes in our study has several possible explanations. In this setting, the PI is used as a measure of distal resistance, caused by cerebral edema and elevated ICP. ALF is, however, associated with both vasodilatation and cerebral edema [2], and the combined effect on the distal vasculature, and therefore the PI, is unclear. In a study by de Riva et al., the TCD-PI was an imperfect predictor of cerebrovascular resistance [34]. An elevated PI has long been acknowledged to be a nonspecific finding, and the TCD-PI may be heavily influenced by the MAP and CO2 [20, 34, 35]. Our finding that the ICPtcd estimated using the CPPe technique may reliably exclude ICP elevation is promising but should be considered preliminary only and requires validation in a larger cohort. While other studies—primarily in TBI—have found ICPtcd to be accurate [16, 36, 37], larger studies are essential. The Bland–Altman analysis (Fig. 5) demonstrated a wide standard deviation, which may have considerable impact on the value of this tool in clinical practice. Changes in the MAP, an integral part of the formula and subject to much variability in ALF patients, may have a substantial impact on the derived CPPe. Factors such as pneumoperitoneum and the Trendelenburg position have been shown to elevate ICPtcd [38]. A multicenter study by Rasulo et al. did demonstrate a systematic overestimation of ICP using the CPPe technique [37]. While we did not find a similar systematic overestimation, ICPtcd may in fact be most useful as a screening tool to exclude intracranial hypertension. It is essential that future validation studies involve multiple sonographers, explicitly standardized technique and effective blinding, in addition to concurrent measurement with the gold standard. The inability of ICPtcd to predict mortality is not entirely surprising, since elevated ICP is no longer the leading cause of death in ALF [5, 39].
Since existing noninvasive tools are either inaccurate or need further evaluation, the optimal strategy for the detection of life-threatening intracranial hypertension in ALF is open to question. While several variables are associated with ICP elevation [39, 40], they are imperfect predictors. Elevations in ICP may not respond to first- and second-line therapies (TIL 1 and 2 measures) [5]. Ongoing assessment of ICP—either through direct measurement or some other forms of clinical evaluation—is therefore necessary. The clinical neurological examination alone is insufficient—a state of deep unresponsiveness may be a result of ICP elevation, or from the metabolic impact of hyperammonemia [2, 5]. Therapeutic measures should be initiated prior to the development of a significant pupillary asymmetry, which heralds cerebral herniation and potentially irreversible injury. Signs of diffuse cerebral edema on CT have also been shown in several studies to not predict sustained ICP elevation in this population [5, 41]. While no easy answer exists, our previously published experience suggests that, until an appropriate alternative is identified, intraparenchymal ICP monitoring can be performed in high-risk patients with a low rate of complications [5]. Strict adherence to a protocol that standardizes patient selection and comprehensive coagulopathy reversal is essential.
Our study has several limitations. This was a retrospective single-center study, although data entry was prospective. Our sample size was small, as is to be expected in any single-center study of ALF that involves the use of IICPM, and was insufficient for any meaningful multivariate analysis of predictors of sustained ICP elevation. However, this has been done in larger published studies [39, 40]. Acquisition of both ONUS and TCD images at the bedside were performed by individuals who were not blinded to the invasive ICP or CPP. The ONSD, however, was measured offline by an investigator blinded to both concurrent ICP and the clinical details of the patient. TCD measures used in the analysis (TAPV, EDV, and PI) were not measured offline from the waveforms by a blinded investigator. They were, however, derived automatically by the ultrasound machine software at the time of the examination and were therefore relatively objective measures and may not have been as prone to error from a lack of blinding as the ONSD. As previously mentioned, since this was not a prospectively designed study, we could not obtain the mean of 3 consecutive evaluations—the sonographer typically recorded only one optimal quality ONUS study from each eye, for clinical purposes. We chose the single highest noninvasive measure for the admission to evaluate against the simultaneously measured invasive gold standard because our primary goal was to evaluate the ability of these noninvasive tests to exclude intracranial hypertension (high negative predictive value). Only two patients died as a consequence of intracranial hypertension; therefore, noninvasive measures could not be studied as predictors specifically of death from cerebral edema or elevated ICP. There were insufficient serial noninvasive measures recorded in the database to study changes in these measures as predictors of intracranial hypertension or outcome.
In conclusion, in patients with ALF, ONUS, and TCD-PI were inaccurate for the detection of concurrent ICP elevation. ICPtcd using the TCD CPPe technique achieved a high negative predictive value for exclusion of ICP elevation on concurrent invasive monitoring. None of the noninvasive measures evaluated predicted mortality.
Change history
30 October 2018
The authors note that the number 14 was inadvertently omitted from the formula listed on page 5 of the article. It currently reads.
Abbreviations
- ALF:
-
Acute liver failure
- AUC:
-
Area under the curve
- CI:
-
Confidence interval
- CPP:
-
Cerebral perfusion pressure
- CPPe:
-
Cerebral perfusion pressure estimated using transcranial Doppler
- CT:
-
Computed tomography
- EDV:
-
End diastolic velocity
- ICP:
-
Intracranial pressure
- ICPtcd:
-
Intracranial pressure estimated using transcranial Doppler
- ICU:
-
Intensive care unit
- IICPM:
-
Invasive intracranial pressure monitoring
- IQR:
-
Interquartile range
- MAP:
-
Mean arterial pressure
- NaCl:
-
Sodium chloride
- ONSD:
-
Optic nerve sheath diameter
- ONUS:
-
Optic nerve ultrasound
- PI:
-
Pulsatility index
- POCUS:
-
Point of care ultrasound
- ROC:
-
Receiver operating characteristic
- TAPV:
-
Time-averaged peak velocity
- TBI:
-
Traumatic brain injury
- TCD:
-
Transcranial Doppler
- TCCS:
-
Transcranial color-coded sonography
- TIL:
-
Therapeutic intensity level
References
Stravitz RT, Kramer AH, Davern T, et al. Intensive care of patients with acute liver failure: recommendations of the U.S. Acute Liver Failure Study Group. Crit Care Med. 2007;35:2498–508.
Raghavan M, Marik PE. Therapy of intracranial hypertension in patients with fulminant hepatic failure. Neurocrit Care. 2006;4:179–89.
Shawcross DL, Wendon JA. The neurological manifestations of acute liver failure. Neurochem Int. 2012;60:662–71.
Vaquero J, Chung C, Blei AT. Brain edema in acute liver failure. A window to the pathogenesis of hepatic encephalopathy. Ann Hepatol. 2003;2:12–22.
Rajajee V, Fontana RJ, Courey AJ, Patil PG. Protocol based invasive intracranial pressure monitoring in acute liver failure: feasibility, safety and impact on management. Crit Care. 2017;21:178.
Karvellas CJ, Fix OK, Battenhouse H, et al. Outcomes and complications of intracranial pressure monitoring in acute liver failure: a retrospective cohort study. Crit Care Med. 2014;42:1157–67.
Munoz SJ, Rajender Reddy K, Lee W, Acute Liver Failure Study G. The coagulopathy of acute liver failure and implications for intracranial pressure monitoring. Neurocrit Care. 2008;9:103–7.
Hansen HC, Helmke K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: ultrasound findings during intrathecal infusion tests. J Neurosurg. 1997;87:34–40.
Dubourg J, Javouhey E, Geeraerts T, Messerer M, Kassai B. Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2011;37:1059–68.
Geeraerts T, Launey Y, Martin L, et al. Ultrasonography of the optic nerve sheath may be useful for detecting raised intracranial pressure after severe brain injury. Intensive Care Med. 2007;33:1704–11.
Karakitsos D, Soldatos T, Gouliamos A, et al. Transorbital sonographic monitoring of optic nerve diameter in patients with severe brain injury. Transplant Proc. 2006;38:3700–6.
Kimberly HH, Shah S, Marill K, Noble V. Correlation of optic nerve sheath diameter with direct measurement of intracranial pressure. Acad Emerg Med. 2008;15:201–4.
Moretti R, Pizzi B. Optic nerve ultrasound for detection of intracranial hypertension in intracranial hemorrhage patients: confirmation of previous findings in a different patient population. J Neurosurg Anesthesiol. 2009;21:16–20.
Rajajee V, Vanaman M, Fletcher JJ, Jacobs TL. Optic nerve ultrasound for the detection of raised intracranial pressure. Neurocrit Care. 2011;15:506–15.
Robba C, Cardim D, Tajsic T, et al. Ultrasound non-invasive measurement of intracranial pressure in neurointensive care: a prospective observational study. PLoS Med. 2017;14:e1002356.
Czosnyka M, Matta BF, Smielewski P, Kirkpatrick PJ, Pickard JD. Cerebral perfusion pressure in head-injured patients: a noninvasive assessment using transcranial Doppler ultrasonography. J Neurosurg. 1998;88:802–8.
Bellner J, Romner B, Reinstrup P, Kristiansson KA, Ryding E, Brandt L. Transcranial Doppler sonography pulsatility index (PI) reflects intracranial pressure (ICP). Surg Neurol. 2004;62:45–51.
Maas AI, Harrison-Felix CL, Menon D, et al. Standardizing data collection in traumatic brain injury. J Neurotrauma. 2011;28:177–87.
Eicke BM, Tegeler CH, Dalley G, Myers LG. Angle correction in transcranial Doppler sonography. J Neuroimaging. 1994;4:29–33.
Czosnyka M, Richards HK, Whitehouse HE, Pickard JD. Relationship between transcranial Doppler-determined pulsatility index and cerebrovascular resistance: an experimental study. J Neurosurg. 1996;84:79–84.
Helmke K, Burdelski M, Hansen HC. Detection and monitoring of intracranial pressure dysregulation in liver failure by ultrasound. Transplantation. 2000;70:392–5.
Krishnamoorthy V, Beckmann K, Mueller M, Sharma D, Vavilala MS. Perioperative estimation of the intracranial pressure using the optic nerve sheath diameter during liver transplantation. Liver Transpl. 2013;19:246–9.
Kim YK, Seo H, Yu J, Hwang GS. Noninvasive estimation of raised intracranial pressure using ocular ultrasonography in liver transplant recipients with acute liver failure: a report of two cases. Korean J Anesthesiol. 2013;64:451–5.
Seo H, Kim YK, Shin WJ, Hwang GS. Ultrasonographic optic nerve sheath diameter is correlated with arterial carbon dioxide concentration during reperfusion in liver transplant recipients. Transplant Proc. 2013;45:2272–6.
Strumwasser A, Kwan RO, Yeung L, et al. Sonographic optic nerve sheath diameter as an estimate of intracranial pressure in adult trauma. J Surg Res. 2011;170:265–71.
Teismann NA, Lenaghan P, Stein J, Green A. Will the real optic nerve sheath please stand up? J Ultrasound Med. 2012;31:130–1.
Hansen HC, Lagreze W, Krueger O, Helmke K. Dependence of the optic nerve sheath diameter on acutely applied subarachnoidal pressure—an experimental ultrasound study. Acta Ophthalmol. 2011;89:e528–32.
Rajajee V, Fletcher JJ, Rochlen LR, Jacobs TL. Comparison of accuracy of optic nerve ultrasound for the detection of intracranial hypertension in the setting of acutely fluctuating vs stable intracranial pressure: post hoc analysis of data from a prospective, blinded single center study. Crit Care. 2012;16:R79.
Optic nerve ultrasound in traumatic brain injury. Accessed December 12, 2017, https://clinicaltrials.gov/ct2/show/NCT02618226.).
Abdo A, Perez-Bernal J, Hinojosa R, et al. Cerebral hemodynamics patterns by transcranial doppler in patients with acute liver failure. Transplant Proc. 2015;47:2647–9.
Aggarwal S, Brooks DM, Kang Y, Linden PK, Patzer JF 2nd. Noninvasive monitoring of cerebral perfusion pressure in patients with acute liver failure using transcranial Doppler ultrasonography. Liver Transpl. 2008;14:1048–57.
Bindi ML, Biancofiore G, Esposito M, et al. Transcranial doppler sonography is useful for the decision-making at the point of care in patients with acute hepatic failure: a single centre’s experience. J Clin Monit Comput. 2008;22:449–52.
Kawakami M, Koda M, Murawaki Y. Cerebral pulsatility index by transcranial Doppler sonography predicts the prognosis of patients with fulminant hepatic failure. Clin Imaging. 2010;34:327–31.
de Riva N, Budohoski KP, Smielewski P, et al. Transcranial Doppler pulsatility index: what it is and what it isn’t. Neurocrit Care. 2012;17:58–66.
Zweifel C, Czosnyka M, Carrera E, de Riva N, Pickard JD, Smielewski P. Reliability of the blood flow velocity pulsatility index for assessment of intracranial and cerebral perfusion pressures in head-injured patients. Neurosurgery. 2012;71:853–61.
Cardim D, Czosnyka M, Donnelly J, et al. Assessment of non-invasive ICP during CSF infusion test: an approach with transcranial Doppler. Acta Neurochir (Wien). 2016;158:279–87.
Rasulo FA, Bertuetti R, Robba C, et al. The accuracy of transcranial Doppler in excluding intracranial hypertension following acute brain injury: a multicenter prospective pilot study. Crit Care. 2017;21:44.
Robba C, Cardim D, Donnelly J, et al. Effects of pneumoperitoneum and Trendelenburg position on intracranial pressure assessed using different non-invasive methods. Br J Anaesth. 2016;117:783–91.
Bernal W, Hyyrylainen A, Gera A, et al. Lessons from look-back in acute liver failure? A single centre experience of 3300 patients. J Hepatol. 2013;59:74–80.
Bernal W, Hall C, Karvellas CJ, Auzinger G, Sizer E, Wendon J. Arterial ammonia and clinical risk factors for encephalopathy and intracranial hypertension in acute liver failure. Hepatology. 2007;46:1844–52.
Munoz SJ, Robinson M, Northrup B, et al. Elevated intracranial pressure and computed tomography of the brain in fulminant hepatocellular failure. Hepatology. 1991;13:209–12.
Funding
There was no funding associated with this study.
Author information
Authors and Affiliations
Contributions
V.R., R.J.F., A.J.C. and P.G.P. designed the larger study from which this data was taken. V.R. developed the concept for the current paper. V.R. and C.A.W. collected the data. V.R. and C.A.W. analyzed the data. V.R., R.J.F. and C.A.W. wrote sections of the paper. All authors discussed the results and implications and edited the manuscript at all stages.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any conflicts of interest to disclose.
Ethical approval
Institutional review board approval was obtained for this study (HUM00139719).
Rights and permissions
About this article

Cite this article
Rajajee, V., Williamson, C.A., Fontana, R.J. et al. Noninvasive Intracranial Pressure Assessment in Acute Liver Failure. Neurocrit Care 29, 280–290 (2018). https://doi.org/10.1007/s12028-018-0540-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-018-0540-x