
Abstract
Objective
This study assessed whether early levels of biomarkers measured in CSF within 24-h of severe TBI would improve the clinical prediction of 6-months mortality.
Methods
This prospective study conducted at two Level 1 Trauma Centers enrolled adults with severe TBI (GCS ≤8) requiring a ventriculostomy as well as control subjects. Ventricular CSF was sampled within 24-h of injury and analyzed for seven candidate biomarkers (UCH-L1, MAP-2, SBDP150, SBDP145, SBDP120, MBP, and S100B). The International Mission on Prognosis and Analysis of Clinical Trials in TBI (IMPACT) scores (Core, Extended, and Lab) were calculated for each patient to determine risk of 6-months mortality. The IMPACT models and biomarkers were assessed alone and in combination.
Results
There were 152 patients enrolled, 131 TBI patients and 21 control patients. Thirty six (27 %) patients did not survive to 6 months. Biomarkers were all significantly elevated in TBI versus controls (p < 0.001). Peak levels of UCH-L1, SBDP145, MAP-2, and MBP were significantly higher in non-survivors (p < 0.05). Of the seven biomarkers measured at 12-h post-injury MAP-2 (p = 0.004), UCH-L1 (p = 0.024), and MBP (p = 0.037) had significant unadjusted hazard ratios. Of the seven biomarkers measured at the earliest time within 24-h, MAP-2 (p = 0.002), UCH-L1 (p = 0.016), MBP (p = 0.021), and SBDP145 (0.029) had the most significant elevations. When the IMPACT Extended Model was combined with the biomarkers, MAP-2 contributed most significantly to the survival models with sensitivities of 97–100 %.
Conclusions
These data suggest that early levels of MAP-2 in combination with clinical data provide enhanced prognostic capabilities for mortality at 6 months.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Brain injury resulting from traumatic, ischemic and/or chemical etiology is an international health concern with significant morbidity and mortality [1]. Approximately 1.7 million people sustain a traumatic brain injury (TBI) annually [2]. In 2010, the Center for disease control (CDC) estimated the economic burden of TBI, including direct and indirect medical costs, to be approximately $76.5 billion. Furthermore, many injuries are under-reported and the true incidence and cost of TBI are likely much higher [1]. According to the CDC, a TBI is defined as being “…caused by a bump, blow or jolt to the head or a penetrating head injury that disrupts the normal function of the brain.” [2]. Unlike other organ-based diseases where rapid diagnosis employing biomarkers can guide treatment of various diseases, no such rapid, definitive diagnostic tests exist for TBI at this time.
Research has shown evidence for the involvement of protein processes that contribute to secondary injury after brain trauma [3, 4]. Advances in protein identification and quantification technologies [5] have provided opportunities to measure neuronal damage. Together with clinical assessment, the quantitative evaluation of neuronal biomarkers measured within 24 h from either cerebrospinal fluid (CSF) and/or blood could assist in the determination of injury severity, provide specifics to anatomical and cellular pathology of the injury, and could alter clinical management. Although there are a number of biochemical markers that have been investigated in TBI, the most extensively studied among these are glial protein S-100 beta (β) [6–16], neuron-specific enolase (NSE) [17–22], and myelin basic protein (MBP) [20, 23–26] Other promising biomarkers include alpha-II-spectrin breakdown products [27–30], Ubiquitin C-terminal Hydrolase-L1 (UCH-L1) [31–34], and microtubule-associated protein (MAP-2) [35].
The International Mission on Prognosis and Analysis of Clinical Trials in TBI (IMPACT) used prospectively collected individual patient data from 11 studies in 8,509 patients with severe or moderate TBI, to develop prognostic models from data available at admission. External validation of the models was conducted on 6,681 patients from the Medical Research Council Corticosteroid Randomization after Significant Head Injury (MRC CRASH) trial [36]. The strongest predictors of outcome were age, pupillary reactivity and GCS motor score (IMPACT Core model score). The performance improved by adding CT characteristics, secondary insults such as hypotension and hypoxia to the Core (IMPACT Extended Model Score) and further improved by including the laboratory parameters of glucose and hemoglobin (IMPACT Lab Model Score).
We hypothesized that together with clinical attributes and radiographic evaluation, neuronal biomarkers would add to long-term mortality prediction in patients with severe TBI. This study assessed whether early levels of biomarkers measured in CSF within 24 h of injury would improve IMPACT prediction of mortality at 6 months in patients with severe TBI.
Methods
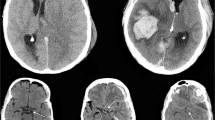
This prospective controlled cohort study enrolled a convenience sample adult patients (>18 years of age) with closed head injuries with a GCS score of <8. From March 2007–August 2011, patients were enrolled at two Level 1 trauma centers in Gainesville, Florida (Shands Hospital, University of Florida) and Houston, Texas (Ben Taub General Hospital, Baylor College of Medicine). Patients met inclusion criteria if they were ≥18 years old with a non-penetrating head injury and had a GCS <8 requiring the placement of an intraventricular catheter (IVC). Patients were excluded if they had a history of pre-existing end-stage organ disease or severe psychiatric illness. All patients had a computerized tomography (CT) scan done as part of their routine evaluation per hospital protocol.
Cerebrospinal fluid samples were obtained within 24 h of admission at 6, 12, 18, and 24 h post-injury by collection from the IVC reservoir that had been emptied 1 h prior to collection. Samples were then stored on ice for up to 12 h before being centrifuged and frozen at −80 °C as 1 ml serum aliquots for future analysis at Banyan Biomarkers Inc. (Alachua, FL, USA). The initial CT scan performed in the emergency department for each patient was reviewed by a single board certified neuroradiologist blinded to the patient’s clinical examination and outcome. The principal scoring system used in the CT interpretation was the Rotterdam Score [36]. The Rotterdam CT score was developed for prognostic purposes in TBI to determine the risk for mortality. It is based on CT findings of basal cistern compression, midline shift, presence of an epidural hematoma, and the presence of either intraventricular blood and/or traumatic subarachnoid hemorrhage. The primary outcome measure was mortality at 6 months post-injury. Because patients were unconscious upon eligibility determination, a 24-h waiver of consent was granted by the IRB. If informed consent could not be obtained from the patient’s legally authorized representative within 24 h, samples were discarded and the patient withdrawn from the study. Control subjects were patients without TBI (n = 21) requiring CSF drainage for other medical conditions such as for routine anesthetic or surgical management (e.g. endovascular aortic aneurysm stent repair, selected orthopedic procedures) or chronic hydrocephalus. Based on our previous work with UCH-L1 [32], the minimum number of control patients required to detect a difference between control and TBI patients was 14 given a power a power of 80 % and a significance level (alpha) of 0.05.
The study was approved by the Institutional Review Boards of the University of Florida and Baylor College of Medicine as well as the University of Houston Committee for the Protection of Human Subjects.
Biomarker Analysis
A number of known and relatively novel brain injury protein biomarkers were selected for this study. They include neuronal cell body injury marker Ubiquitin C-terminal hydrolase-L1 (UCH-L1), breakdown products of axonally enriched αII-spectrin (SBDP150 and SBDP145 produced by necrosis-linked calpain protease and SBDP120 produced by the apoptosis-linked caspase-3 protease), dendritic injury marker microtubule-associated protein-2 (MAP-2), glial marker S100b and demyelination marker myelin basic protein (MBP) [37–39]. The table in the appendix describes the Lower (LLoD) and Upper (ULoD) limits of detection for each of the seven biomarkers. Imputed values were used for concentrations below the LLoD by calculating half of lowest level measured. Appendix 1 describes how biomarker analysis was performed in the lab on each of the seven biomarkers.
Data Analysis
Data were analyzed using descriptive statistics and were assessed for distribution and variance. The IMPACT scores were calculated for each patient (1) Core IMPACT score (age, pupillary reactivity and GCS motor score), (2) Extended IMPACT score (core + hypoxia, hypotension, CT findings), and (3) Lab IMPACT score (Extended + glucose and hemoglobin) to determine risk of mortality at 6 months [36]. Biomarkers were also examined independently for prediction of 6 month mortality. Correlations between the biomarkers were assessed using Spearman’s rho. A comparison of biomarker levels between TBI and control subjects was performed using the Mann–Whitney U test. Data were assessed for equality of variance and distribution. Logarithmic transformations were conducted on non-normally distributed data. We examined the association between the biomarkers and the risk of 6 month mortality using multivariable proportional hazards (Cox) models. Variables included in the Cox proportional hazards models were the Core, Extended and Lab IMPACT scores, as well as the levels of each of the seven biomarkers measured within 24 h of injury. Different combinations of IMPACT scores and biomarkers were modeled. Area under the ROC curve (AUC) was calculated to determine performance of each model in predicting 6-months mortality. Analysis of the biomarkers included performance of each biomarker at 12-h post-injury and earliest CSF samples (mixture of samples obtained at 6, 12, 18 and 24 h post-injury). Significance was set at p ≤ 0.05.
Results
There were at total 152 patients enrolled, 131 were TBI patients and 21 were control patients. Characteristics of the TBI patients are described in Table 1. Control patients were a mean age of 73 (SD8) (range 56–85), 68 % were male, and 5 % were Asian, 5 % Black, 5 % Hispanic and 85 % were white. The enrolled TBI patients were a mixture of those with isolated head injury and multiple traumas. In Table 2 types and severity of concomitant injuries, based on the abbreviated injury scale (AIS), are compared in those who survived and did not survive to 6 months. Concomitant injuries were equally distributed among the two groups with no statistically significant differences except for thoracic trauma.
Of the 131 TBI patients, 110 had CSF collected for biomarker analysis within 24 h of injury (Fig. 1). Thirty (27 %) patients did not survive to 6 months. Of these, 5 patients (17 %) died within 48 h of injury, fourteen (47 %) died between 48 h to a week, seven (23 %) died between 1-week and 1-month, and 4 patients (13 %) died between 1 to 3-months. No patients died between 3–6 months. Twenty one patients (70 %) of patients’ deaths were directly associated with their TBI and the other 9 (30 %) had concomitant injuries or complications that may have contributed to their deaths in addition to the TBI. Two patients (7 %) died of brain death, 4 (13 %) died of traumatic/cardiac arrest, 6 (20 %) died from TBI complications, 13 (43 %) remained in a vegetative state and/or had care withdrawn, and 5 (17 %) died from non-neurological complications. Initial levels of biomarkers drawn within 24 h of injury are compared in those who did and did not survive to 6 months (Fig. 2).

Flow diagram

Comparison of initial biomarker levels in patients who survived and did not survive over 6 months. Bar graphs represent mean values with standard errors. A comparison of the earliest 24-h level of each biomarker in patients who survived versus those who died within 6-months post-injury reveals that survivors had significantly lower biomarker levels than non-survivors
The temporal profile of the biomarkers in the first 24 h after injury, taken at 6 h intervals, is shown in Fig. 3. The biomarkers were all significantly elevated compared to controls (p < 0.001) and each showed different patterns of elevation. UCH-L1, S100B and SBDP150 decreased gradually over 24 h. MBP had a more labile pattern of a rapid rise followed by a rapid fall and a subsequent rise. MAP-2 and SBDP145 remained consistently elevated, with minor peaks and toughs. Interestingly, SBDP120 only began to rise after 12 h. In Fig. 4 the temporal profile of each biomarker is compared in patients who did and did not survive to 6 months. The peak (maximum) levels of UCH-L1, SBDP145, MAP-2, and MBP were significantly higher in those who did not survive to 6 months (p < 0.05). The correlations between the seven biomarkers are listed in Table 3. The highest correlation was found between MAP-2 and UCH-L1 (rho = 0.81).

Temporal profile of biomarkers over 24 h in TBI patients compared to control subjects. Lines represent mean values with standard errors. All biomarkers are significantly elevated in TBI patients compared to control subjects (p < 0.001). The number of available samples at each time-point was 21 controls, 23 at 6-h, 57 at 12-h, 83 at 18-h, and 89 at 24-h. MAP-2 and SBDP120 levels were multiplied by 10 in order to show their patterns more clearly on the graph

Temporal profile of biomarkers over 24 h in all TBI patients who did and did not survive to 6 months. Lines represent mean values with standard errors. There are higher peaks of biomarkers in those who did not survive to 6 months compared to those who did survive
We evaluated the biomarkers at a discrete time-point (12-h post-injury) and also at the earliest time-point the sample was available at in the first 24 h (“earliest” level was mixture of samples taken at 6, 12, 18 and 24 h post-injury). The rationale for the 12 h time-point was that many severe TBI patients are stabilized and admitted and have a ventriculostomy in place for fluid sampling by 12 h. The rationale for the “earliest” time-point is practice variation. Some clinicians may have access to samples earlier or later than 12 h so taking the “earliest” sample is most reflective of how the biomarker samples would be obtained in clinical practice. In our cohort there were 57 patients who had 12-h samples available for analysis and 110 patients with an “earliest time-point” available. The distribution of sample times in the “earliest time-point” group included 69 (63 %) enrollment samples (taken at the time of the ventriculostomy), 11 (10 %) samples taken at 6 h post-injury, 15 (14 %) samples at 12 h post-injury, 10 (9 %) samples at 18 , and 5 (5 %) samples at 24 h.
Survival analysis was conducted to assess the IMPACT models and biomarkers, both independently and in combination. At the 12-h post-injury there were 57 patients with biomarker data available. Of the three IMPACT Clinical Models (Core, Extended and Lab), the Extended Model had the highest unadjusted hazard ratio for mortality at 6 months 1.03 (95 % CI 1.01–1.05) (p < 0.001) and was selected for further analysis (Table 4). Of the seven biomarkers measured at 12 h post-injury (N = 57), the ones with the most significant unadjusted hazard ratios were MAP-2 (p = 0.004), UCH-L1 (p = 0.024), and MBP (p = 0.037) (Table 4). When the IMPACT Extended Model was combined with the biomarkers, MAP-2 was the only biomarker that contributed significantly to the survival model (Table 5). IMPACT Extended Model and MAP-2 yielded adjusted hazard ratios of 1.04 (1.01–1.06) (p = 0.001) and 2.14 (1.31–3.50) (p = 0.002) respectively. There was no further benefit to including additional biomarkers.
At the “earliest” 24-h time-point there were 110 patients with biomarker data available for analysis. Concordant with the 12-h time-point, the Extended IMPACT Model had the highest unadjusted hazard ratio for mortality at 6 months 1.03 (95 %CI 1.02–1.05) (p < 0.001) and was selected for further analysis (Table 4). Of the seven biomarkers measured at the earliest time post-injury (N = 110), the ones with the most significant unadjusted hazard ratios were MAP-2 (p = 0.002), UCH-L1 (p = 0.016), MBP (p = 0.021), and SBDP145 (0.029) (Table 4). When the IMPACT Extended Model was combined with the biomarkers, MAP-2 was the only biomarker that contributed significantly to the survival model (Table 5). IMPACT Extended Model and MAP-2 yielded adjusted hazard ratios of 1.03 (1.01–1.04) (p = 0.001) and 1.43 (1.04–1.95)(p = 0.026) respectively. There was no further benefit to including additional biomarkers.
We explored cutoff points for IMPACT and MAP-2 derived from the ROC Curves for predicting mortality at 6 months. This exploratory analysis was intended to maximize the sensitivity. Using the 12 h time-point, the combination of an IMPACT Extended risk of death ≥24 % or MAP-2 level >1.0 ng/ml yielded a sensitivity of 100 %, a specificity of 19 % and a negative predictive value of 100 % (Table 6). Using the earliest 24 h level, the same combination of an IMPACT Extended risk of death ≥24 % and MAP-2 level >1.0 ng/ml yielded a sensitivity of 97 %, a specificity of 20 %, and a negative predictive value of 92 % (Table 6). Sensitivity of 12-h MAP-2 levels (without IMPACT) provided a sensitivity of 87 % and a specificity of 30 % (Table 6). Sensitivity of the earliest MAP-2 levels (without IMPACT) provided a sensitivity of 83 % and a specificity of 31 % (Table 6).
Discussion
This study describes a cohort of non-penetrating severe TBI patients who underwent clinical and biomarker evaluation within 24 h of injury. Clinical IMPACT models were used to assess 6 month outcome using baseline clinical data [36]. IMPACT models were originally developed using a patient cohort of 8,509 patients with moderate and severe TBI and have subsequently been validated [40]. The early prediction of outcome in TBI allows for baseline risk establishment and clinical considerations for patient care. Our hypothesis was that initial neuronal biomarkers measured in CSF would improve upon the clinical IMPACT prediction models of mortality. We found that, indeed, biomarkers contributed significantly to the clinical IMPACT models, particularly MAP-2. In fact, biomarkers had predictive ability, independent of the clinical models. In practice, this would be especially useful when certain pieces of clinical information and CT evaluation are not readily available at the time of assessment.
Depending on the hospital center or the patient’s condition, CSF may be accessible at different times during the first 24 h after injury. Therefore, the analysis included biomarker evaluation at a discrete time-point (12-h post-injury) and at the earliest available sample time-point within 24 h (“earliest” level). The rationale for these two different types of analyses was to see how the biomarkers could be applied clinically. The results had better sensitivity using a single time-point analysis than the “earliest” time-point yet both provided important prognostic information to the clinical models. We suspect that because a number of CSF samples in the “earliest time point” group were obtained at or before 6-h post-injury, levels were not given as much time to become elevated as they were at 12-h, leading to reduced sensitivity. This underscores the need to evaluate biomarkers at multiple time-points within the first 24 h. The next step in determining optimal times for clinical use of each biomarker will be to formally assess temporal profiles by conducting biokinetic analyses. Much like biomarkers for other organ diseases, there is a pattern of release, peak and duration that is specific to each biomarker. For example, in myocardial ischemia troponin may not appear until 3–6 h after the start of ischemia. So, if troponin is measured at 1 h, the results will not be as accurate.
Although there are a number of biochemical markers that have been investigated in TBI, the most extensively studied among these are glial protein S-100 beta (β) [6–16], neuron-specific enolase (NSE) [17–22], and myelin basic protein (MBP) [20, 23–26] S100β is the major low affinity calcium binding protein in astrocytes [41] and it is considered a marker of astrocyte injury or death. Alpha-II-spectrin (280 kDa) is the major structural component of the cortical membrane cytoskeleton and is particularly abundant in axons and presynaptic terminals [42, 43]. It is also a major substrate for both calpain and caspase-3 cysteine proteases [44, 45]. Evaluation of these breakdown products in humans with severe TBI, are encouraging [27–30]. A promising candidate biomarker for TBI currently under investigation is Ubiquitin C-terminal Hydrolase-L1 (UCH-L1). UCH-L1 was previously used as a histological marker for neurons due to its high abundance and specific expression in neurons [46]. Clinical studies in humans with severe and mild TBI have confirmed that UCH-L1 is significantly elevated after injury and is associated with important clinical outcomes [31–34]. Another unexplored neurobiomaker is microtubule-associated protein (MAP-2). It is a dendritic marker of both acute damage and chronic neuronal regeneration after injury and can be detected in serum of survivors after severe TBI [35].
Although these biomarkers were collected from CSF, many are or have become available for use in serum [34, 47, 48]. Recently, Czeiter et al. [47] evaluated three biomarkers, including glial fibrillary acidic protein (GFAP), Ubiquitin C-terminal hydrolase (UCH-L1) and αII-spectrin break down product of 145 kDa (SBDP145) in a cohort of 45 severe TBI patients. They compared the biomarkers only to the IMPACT Core model and showed that biomarkers improved outcome prediction. Accordingly, our results also show the value of adding biomarkers to clinical parameters. We explored seven distinct biomarkers in a larger cohort of patients, together with all three IMPACT clinical models (Core, Extended, and Lab). The biomarker that consistently improved prognostic performance in our large cohort was MAP-2, a biomarker that has not been assessed in any other acute clinical TBI trial to date. MAP-2 is a relatively novel biomarker in human TBI and is a major component of cytoskeleton family proteins. It is localized predominantly in dendrites and is associated with promoting microtubule assembly and stability [49, 50]. It has been shown to be altered following TBI in animal models and is associated with dendritic damage [51, 52].
We performed an exploratory analysis of cutoff points for IMPACT and MAP-2 based on the points from the ROC to determine sensitivity and specificity of the model using both discrete 12-h levels and earliest 24-h levels. The combination of IMPACT and MAP-2 yielded a sensitivity of 100 % for predicting mortality with a specificity of 19 %. Using the same cutoff points, we also assessed the performance of MAP-2 alone and found a sensitivity of between 83–87 % with a much higher specificity of 30 %. There is always a trade-off between sensitivity and specificity and we chose to maximize sensitivity at the expense of the specificity. With a high sensitivity the biomarkers would be useful in “ruling out” (i.e. low risk of) mortality if levels were below the threshold, suggesting good chances for survival at 6-months. The converse would not be true however. The importance of these findings is that clinicians could make management decisions with the help of a readily available biomarker, as is done with cardiac ischemia, renal dysfunction or liver dysfunction. In practice, this would be especially useful when certain pieces of clinical information and CT evaluation are not readily available at the time of assessment.
Limitations
While these data are encouraging, the authors recognize there are limitations to this study. Clinical management dictated when the ventriculostomy was placed and therefore, patients had a variable number of samples available for analysis at the different time points during the first 24 h. The most common surgically placed monitors for intracranial pressure monitoring in severe TBI patients are intraventricular catheters (ventriculostomy). However, intraparenchymal catheters are becoming an increasingly popular alternative to ventriculostomy for in many countries as they are easier to use, less invasive and can be inserted in the ICU by non-neurosurgeons [53]. Since the purpose of the study was to identify biomarkers that are related to outcome in CSF, intraventricular catheters were the logical choice for study purposes. More importantly, it was standard of care at the participating institutions. Now that we’ve identified promising biomarkers in CSF, the same biomarkers are being examined in blood, where they could have more widespread application. As an exploratory analysis these results provide a starting point for larger studies that can validate these results. This is an important step forward in the management of patients with brain injuries, similar to the use of blood lactate levels in predicting mortality in critically ill patients [54, 55].
Although the overall mortality rate in our study seems higher than average there is a lot of variability in mortality rate in TBI studies, depending on initial injury severity. In 2011, Lingsma et al. examined between-center differences in outcome after moderate and severe TBI as part of the International Mission on Prognosis and Clinical Trial Design in TBI (IMPACT), and found mortality rates in the different studies ranged from 17 % to 44 % with an average of 27 % [56]. Based on published data, the patients in our study are fairly typical for a severe TBI study, and the outcomes are fairly typical for these patients as well even if they are at the higher end of what is reported.
There is a significant age difference between TBI subjects and control subjects in our study. Control subjects were patients without TBI requiring CSF drainage for other medical conditions such as for routine anesthetic or surgical management (e.g. endovascular aortic aneurysm stent repair, selected orthopedic procedures) or chronic hydrocephalus. Accordingly, they had a tendency of being older. However, it has been shown that older adults have higher levels of neuronal biomarker at baseline [57]. Therefore, older controls are actually a more robust control group as there levels are higher.
Additionally, there is a need to further explore these biomarkers in subpopulations of patients with TBI who have concomitant diagnoses of dementia, Parkinson’s disease, stroke or prior TBI. Based on the current results, we cannot recommend a change in patient management. However, if validated, biomarker levels could be used to determine severity of injury, stratify patients into clinical trials and gauge effectiveness of therapy. Accordingly, they would be helpful in discussing prognosis with families and making decisions about futility of care earlier. Additionally, biokinetic analyses of these data will be crucial in quantifying the temporal patterns of each biomarker.
Conclusions
These data suggest that early CSF levels of MAP-2 in combination with clinical data provide enhanced prognostic capabilities for mortality at 6 months in patients with severe TBI. These findings have implications for improved clinical decision-making early after injury. Further validation of these findings in a larger cohort of patients will be required before clinical implementation.
References
Corrigan JD, Selassie AW, Orman JA. The epidemiology of traumatic brain injury. J Head Trauma Rehabil. 2010;25(2):72–80.
Faul M, Xu L, Wald MM, et al. Traumatic Brain Injury in the United States. In: Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2010.
Gaetz M. The neurophysiology of brain injury. Clin Neurophysiol. 2004;115(1):4–18.
Pineda JA, Wang KK, Hayes RL. Biomarkers of proteolytic damage following traumatic brain injury. Brain Pathol. 2004;14(2):202–9.
Haskins WE, Kobeissy FH, Wolper RA, et al. Rapid discovery of putative protein biomarkers of traumatic brain injury by SDS-PAGE-capillary liquid chromatography-tandem mass spectrometry. J Neurotrauma. 2005;22(6):629–44.
MisslerU. S-100 protein and neuron-specific enolase concentrations in blood as indicators of infarction volume and prognosis in acute ischemic stroke. Stroke. 1997;28:1956–60.
Ytrebo LMNG, Korvald C, et al. Renal elimination of protein S-100beta in picgs with acute encephalopathy. Scand J Clin Lab Invest. 2001;61:217–25.
Jonsson HJP, Hoglund P, Alling C, Blomquist S. The elimination of S-100b and renal function after cardiac surgery. J Cardiothorac Vasc Aneth. 2000;14:698–701.
Usui AKK, Abe T, Murase M, Tanaka M, Takeuchi E. S-100ao protein in blood and urine during open-heart surgery. Clin Chem. 1989;35:1942–4.
Raabe A, Grolms C, Seifert V. Serum markers of brain damage and outcome prediction in patients after severe head injury. Br J Neurosurg. 1999;13(1):56–9.
Haimoto H, Hosoda S, Kato K. Differential distribution of immunoreactive S100-a and S100-b proteins in normal nonnervous human tissues. Lab Invest. 1987;57:489–98.
Woertgen C, Rothoerl RD, Holzschuh M, et al. Comparison of serial S-100 and NSE serum measurements after severe head injury. Acta Neurochir (Wien). 1997;139(12):1161–4 discussion 1165.
Romner B, Ingebrigtsen T, Kongstad P, et al. Traumatic brain damage: serum S-100 protein measurements related to neuroradiological findings. J Neurotrauma. 2000;17(8):641–7.
Korfias S, Stranjalis G, Boviatsis E, et al. Serum S-100B protein monitoring in patients with severe traumatic brain injury. Intensive Care Med. 2007;33(2):255–60.
Vos PE, Jacobs B, Andriessen TM, et al. GFAP and S100B are biomarkers of traumatic brain injury: an observational cohort study. Neurology. 2010;75(20):1786–93.
Berger RP, Pierce MC, Wisniewski SR, et al. Serum S100B concentrations are increased after closed head injury in children: a preliminary study. J Neurotrauma. 2002;19(11):1405–9.
Bw M. A soluble protein characteristic of the nervous system. Biochem Biophys Res Commun. 1965;19:739–44.
Donato R. Functional roles of S100 proteins, calcium-binding proteins of the EF-hand type. Biochim Biophys Acta. 1999;1450:191–231.
Cooper E. Neuron-specific enolase. Int J Biol Markers. 1994;4:205–10.
Yamazaki Y, Yada K, Morii S, et al. Diagnostic significance of serum neuron-specific enolase and myelin basic protein assay in patients with acute head injury. Surg Neurol. 1995;43(3):267 discussion 270–261.
de Kruijk JR, Leffers P, Menheere PP, et al. S-100B and neuron-specific enolase in serum of mild traumatic brain injury patients. A comparison with health controls. Acta Neurol Scand. 2001;103(3):175–9.
Naeimi ZS, Weinhofer A, Sarahrudi K, et al. Predictive value of S-100B protein and neuron specific-enolase as markers of traumatic brain damage in clinical use. Brain Inj. 2006;20(5):463–8.
Berger RP, Adelson PD, Pierce MC, et al. Serum neuron-specific enolase, S100B, and myelin basic protein concentrations after inflicted and noninflicted traumatic brain injury in children. J Neurosurg. 2005;103(1 Suppl):61–8.
Wang KK, Ottens AK, Liu MC, et al. Proteomic identification of biomarkers of traumatic brain injury. Expert Rev Proteomics. 2005;2(4):603–14.
Berger RP, Beers SR, Richichi R, et al. Serum biomarker concentrations and outcome after pediatric traumatic brain injury. J Neurotrauma. 2007;24(12):1793–801.
Beers SR, Berger RP, Adelson PD. Neurocognitive outcome and serum biomarkers in inflicted versus non-inflicted traumatic brain injury in young children. J Neurotrauma. 2007;24(1):97–105.
Pineda JA, Lewis SB, Valadka AB, et al. Clinical significance of alphaII-spectrin breakdown products in cerebrospinal fluid after severe traumatic brain injury. J Neurotrauma. 2007;24(2):354–66.
Brophy GM, Pineda JA, Papa L, et al. alphaII-Spectrin breakdown product cerebrospinal fluid exposure metrics suggest differences in cellular injury mechanisms after severe traumatic brain injury. J Neurotrauma. 2009;26(4):471–9.
Mondello S, Robicsek SA, Gabrielli A, et al. alphaII-spectrin breakdown products (SBDPs): diagnosis and outcome in severe traumatic brain injury patients. J Neurotrauma. 2010;27(7):1203–13.
Berger RP, Hayes RL, Richichi R, et al. Serum concentrations of ubiquitin C-terminal hydrolase-L1 and alphaII-spectrin breakdown product 145 kDa correlate with outcome after pediatric TBI. J Neurotrauma. 2012;29(1):162–7.
Siman R, Toraskar N, Dang A, et al. A panel of neuron-enriched proteins as markers for traumatic brain injury in humans. J Neurotrauma. 2009;26(11):1867–77.
Papa L, Akinyi L, Liu MC, et al. Ubiquitin C-terminal hydrolase is a novel biomarker in humans for severe traumatic brain injury. Crit Care Med. 2010;38(1):138–44.
Brophy GM, Mondello S, Papa L, et al. Biokinetic Analysis of Ubiquitin C-Terminal Hydrolase-L1 (UCH-L1) in Severe Traumatic Brain Injury Patient Biofluids. J Neurotrauma. 2011;28(6):861–70.
Papa L, Lewis LM, Silvestri S, et al. Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention. J Trauma Acute Care Surg. 2012;72(5):1335–44.
Mondello S, Gabrielli A, Catani S, et al. Increased levels of serum MAP-2 at 6-months correlate with improved outcome in survivors of severe traumatic brain injury. Brain Inj. 2012;26(13–14):1629–35.
Steyerberg EW, Mushkudiani N, Perel P, et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 2008;5(8):e165 discussion e165.
Zhang Z, Mondello S, Kobeissy FH, et al. Protein biomarkers for traumatic and ischemic brain injury: from Bench to Bedside. Transl Stroke Res. 2011;2(4):455–62.
Papa L, Robinson G, Oli M, et al. Use of Biomarkers for Diagnosis and Management of Traumatic Brain Injury Patients. Expert Opin Med Diagn. 2008;2(8):937–45.
Papa L. Exploring the Role of Biomarkers for the Diagnosis and Management of Traumatic Brain Injury Patients. In: Man TK, Flores RJ, editors. Proteomics - Human Diseases and Protein Functions. 1st ed. Veinna: In Tech Open Access Publisher; 2012.
Perel P, Arango M, Clayton T, et al. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ. 2008;336(7641):425–9.
Xiong H, Liang WL, Wu XR. Pathophysiological alterations in cultured astrocytes exposed to hypoxia/reoxygenation. Sheng Li Ke Xue Jin Zhan. 2000;31(3):217–21.
Goodman SR, Zimmer WE, Clark MB, et al. Brain spectrin: of mice and men. Brain Res Bull. 1995;36(6):593–606.
Riederer BM, Zagon IS, Goodman SR. Brain spectrin(240/235) and brain spectrin(240/235E): two distinct spectrin subtypes with different locations within mammalian neural cells. J Cell Biol. 1986;102(6):2088–97.
Wang KK, Posmantur R, Nath R, et al. Simultaneous degradation of alphaII- and betaII-spectrin by caspase 3 (CPP32) in apoptotic cells. J Biol Chem. 1998;273(35):22490–7.
McGinn MJ, Kelley BJ, Akinyi L, et al. Biochemical, structural, and biomarker evidence for calpain-mediated cytoskeletal change after diffuse brain injury uncomplicated by contusion. J Neuropathol Exp Neurol. 2009;68(3):241–9.
Jackson P, Thompson RJ. The demonstration of new human brain-specific proteins by high-resolution two-dimensional polyacrylamide gel electrophoresis. J Neurol Sci. 1981;49(3):429–38.
Czeiter E, Mondello S, Kovacs N, et al. Brain injury biomarkers may improve the predictive power of the IMPACT outcome calculator. J Neurotrauma. 2012;29(9):1770–8.
da Rocha AB, Schneider RF, de Freitas GR, et al. Role of serum S100B as a predictive marker of fatal outcome following isolated severe head injury or multitrauma in males. Clin Chem Lab Med. 2006;44(10):1234–42.
Chen LJ, Wang YJ, Tseng GF. Compression alters kinase and phosphatase activity and tau and MAP2 phosphorylation transiently while inducing the fast adaptive dendritic remodeling of underlying cortical neurons. J Neurotrauma. 2010;27(9):1657–69.
Diez-Guerra FJ, Avila J. Rapid dephosphorylation of microtubule-associated protein 2 in the rat brain hippocampus after pentylenetetrazole-induced seizures. Eur J Biochem. 1993;215(1):181–7.
Posmantur RM, Kampfl A, Taft WC, et al. Diminished microtubule-associated protein 2 (MAP2) immunoreactivity following cortical impact brain injury. J Neurotrauma. 1996;13(3):125–37.
Kobeissy FH, Ottens AK, Zhang Z, et al. Novel differential neuroproteomics analysis of traumatic brain injury in rats. Mol Cell Proteomics. 2006;5(10):1887–98.
Khan SH, Kureshi IU, Mulgrew T, et al. Comparison of percutaneous ventriculostomies and intraparenchymal monitor: a retrospective evaluation of 156 patients. Acta Neurochir Suppl. 1998;71:50–2.
Iberti TJ, Leibowitz AB, Papadakos PJ, et al. Low sensitivity of the anion gap as a screen to detect hyperlactatemia in critically ill patients. Crit Care Med. 1990;18(3):275–7.
Hunter CL, Silvestri S, Dean M, et al. End-tidal carbon dioxide is associated with mortality and lactate in patients with suspected sepsis. Am J Emerg Med. 2013;31(1):64–71.
Lingsma HF, Roozenbeek B, Li B, et al. Large between-center differences in outcome after moderate and severe traumatic brain injury in the international mission on prognosis and clinical trial design in traumatic brain injury (IMPACT) study. Neurosurgery. 2011;68(3):601–7 discussion 607–608.
Ferguson I, Lewis L, Papa L. Neuronal Biomarkers may require age-adjusted norms. Ann Emerg Med. 2011;58(4):S213.
Liu MC, Akinyi L, Scharf D, et al. Ubiquitin C-terminal hydrolase-L1 as a biomarker for ischemic and traumatic brain injury in rats. Eur J Neurosci. 2010;31(4):722–32.
Mondello S, Papa L, Buki A, et al. Neuronal and glial markers are differently associated with computed tomography findings and outcome in patients with severe traumatic brain injury: a case control study. Crit Care. 2011;15(3):R156.
Mondello S, Gabrielli A, Catani S, et al. Increased levels of serum MAP-2 at 6 months correlate with improved outcome in survivors of severe traumatic brain injury. Brain Inj. 2012;26(13-14):1629–35.
Dutta S, Chiu YC, Probert AW, et al. Selective release of calpain produced alphalI-spectrin (alpha-fodrin) breakdown products by acute neuronal cell death. Biol Chem. 2002;383(5):785–91.
Nath R, Davis M, Probert AW, et al. Processing of cdk5 activator p35 to its truncated form (p25) by calpain in acutely injured neuronal cells. Biochem Biophys Res Commun. 2000;274(1):16–21.
Conflict of interest
Drs. Gabrielli, Hannay, Heaton, Robertson, Robicsek, and Schmalfuss have no competing financial interests.
Fundings
This study was funded by NIH RO1 NS052831 “Biochemical Markers of Severe Traumatic Brain Injury”. Drs. Brophy and Papa are consultants of Banyan Biomarkers, Inc. but receive no stocks or royalties from the company and will not benefit financially from this publication. Dr. Hayes and Wang own stock, receive royalties from Banyan Biomarkers Inc., and as such may benefit financially as a result of the outcomes of this research or work reported in this publication.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
See Table 7.
Ubiquitin C-terminal Hydrolase (UCH-L1)
UCH-L1 sandwich ELISA (swELISA) was performed in accordance with previously published studies [29, 32–34, 58–60]. Both mouse monoclonal antibody (capture antibody) and rabbit polyclonal antibody (detection antibody) were made in-house at Banyan Biomarkers Inc. against recombinant human UCH-L1 full-length protein and protein A purified. Plates were coated with capture antibody in 0.05 M sodium bicarbonate, pH 9.6 overnight at 4 °C. Blocking and washing buffer was Tris buffered saline with 0.05 % Tween-20 (v/v) (TBST). Antigen standard (UCH-L1 standard curve: 0.78–200 ng/mL; unknown samples: 10 µL of CSF) were incubated with detection antibody overnight and then added to the plate for 2 h. After washing, secondary anti-rabbit-IgG HRP (GE Healthcare) was added and incubated for 1 h. Plates were developed with substrate solution Ultra-TMB ELISA (Pierce# 34,028), stopped with acidic solution and read at 450 nm with a spectrophotometer (Molecular Device SpectraMax 190). The interassay CV was 2–8 % while intraassay CV was 2–11 % within the dynamic range. The limit of detection (LOD) was 0.03 ng/mL.
αII-Spectrin Breakdown Products 150 kDa (SBDP150), 145 kDa (SBDP145), 120 kDa (SBDP120)
SBDP150, SBDP145 and SBDP120 swELISAs were constructed similarly to those described previously [29]. Briefly, a 96-well plate was coated with 100 μL/well capture antibody (5ug/ml purified goat polyclonal anti-SBDP150 [28, 61] or 10ug/ml rabbit anti-SBDP145 or 10ug/ml anti-SBDP120 [62] overnight at 4 °C. Antigen used was partially purified human brain αII-spectrin for SBDP150 or recombinant glutathione-S-transferase– αII-spectrin (including the SBDP145 cleavage site in repeat 13–18) fusion protein cleaved with either calpain-1 (1: 40 ratio for 10 min at 4C) for SBDP145 production or with caspase-3 (1 : 20 ratio for 4 h at room temperature) for SBDP120. After blocking buffer (Startingblock T20-PBS), SBDP150 calibrator (10 × dilution factor, 1.17 ng/ml–300 ng/ml), SBDP145 calibrator (10X dilution factor, 1–500 ng/ml) and SBDP120 Calibrators (3X dilution factor, 0.9–120 ng/mL) or samples were added (CSF, 10 μL for SBDP150, SBDP145; 34 uL for SBDP120) with diluent (total volume 100 uL) to the wells. After washing, plates were incubated with affinity purified detection antibody (mouse monoclonal anti-αII-spectrin antibody (Biomol FG6090 or equivalent). If amplification was needed, biotinyl-tyramide solution (Perkin Elmer Elast Amplification Kit) was added, washed and followed by Streptavidin-HRP (1:500) in PBS with 0.02 % Tween-20 and 1 % BSA. Lastly, the wells were developed with chemiluminescent substrate solution (SuperSignal ELISA Femto, Pierce) for 1 min and read by a luminescence microplate reader (GloRunner DXL Luminometer, Turner BioSystems). The interassay and intraassay CV were <3–14 % within the assay dynamic range. The LOD was 1.54 ng/mL for SBDP150, 0.98 ng/mL for SBDP145 and 0.474 ng/mL for SBDP120.
Microtubule Associated Protein 2 (MAP-2)
MAP-2 sandwich ELISA was performed using 10 uL CSF for quantitative determination. Mouse MAb anti-MAP2A/2B (clone M13, Zymed #13-1,500) was used as capture antibody (5 ug/well) to coat the plate. Biofluid samples (10 uL CSF, or recombinant antigen as GST-fusion protein with residue 1,078–1,551 of MAP-2 at 0.10–6.67 ng/mL) were added with diluent (100 uL total) to microtiter plate wells. After 2 h incubation and washing, HRP-labeled mouse monoclonal anti-MAP-2 (clone AP20; BD Bioscience; #552,320) antibody was added. After washing, plates were developed with substrate solution Ultra-TMB ELISA (Pierce# 34,028), stopped with acidic solution and read at 450 nm with a spectrophotometer (Molecular Device SpectraMax 190). The interassay and intraassay CV were <15 % within the assay dynamic range. Limit of detection (LOD) was determined to be 0.054 ng/mL.
S100B
S100B sandwich ELISA was performed using 5–10 uL CSF for quantitative determination. Mouse monoclonal anti-S100b was used as capture antibody (3ug/well) to coat the plate. After blocking buffer, biofluid samples (5–10 uL CSF) or standard protein (S100beta, human brain protein, Fitzgerald, at 0.0039 ng/ml–0.5 ng/ml) were added. After 30 min incubation and washing, detection polyclonal antibody was used and incubated for 1 h (1 ug/ml and 100 ul/well), followed by HRP-conjugated anti-rabbit-HRP (Jacksonville ImmunoResearch lab) for 30 min. After washing, plates were developed with substrate solution Ultra-TMB ELISA (Pierce# 34,028), stopped with acidic solution, and read at 450 nm with a microplate spectrophotometer (Molecular Device SpectraMax 190). The interassay and intraassay CV were <10 % within the assay dynamic range with a limit of detection (LOD).
Myelin Basic Protein (MBP)
MBP assay was based on commercial MBP ELISA for CSF (iPOC) according to manufacturer’s instructions. Briefly, 50 uL of calibrator (0.13–36 ng/mL) or 4 uL CSF samples with diluent (to 50 uL) was used and incubated with plate with capture antibody (goat polyclonal anti-MBP) for 2 h. After washing, 50 uL detection mouse monoclonal antibody to MBP was added (50 uL) and incubated for 30 min, followed by HRP-enzyme-conjugated secondary donkey anti- mouse IgG antibody. After washing, 50 uL of chromogenic TMB substrate was used for 15 min. 100 uL stop solution was added and absorbance at 450 nm was measured with a spectrophotometer (Molecular Device Spectramax 190). The interassay and intraassay CV were <10 % within the assay dynamic range. The limit of detection was determined to be 0.13 ng/ml.
Rights and permissions
About this article

Cite this article
Papa, L., Robertson, C.S., Wang, K.K.W. et al. Biomarkers Improve Clinical Outcome Predictors of Mortality Following Non-Penetrating Severe Traumatic Brain Injury. Neurocrit Care 22, 52–64 (2015). https://doi.org/10.1007/s12028-014-0028-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-014-0028-2