
Abstract
Background
We asked whether continuous intracranial pressure (ICP) monitoring data could provide objective measures of the degree and timing of intracranial hypertension (ICH) in the first week of neurotrauma critical care and whether such data could be linked to outcome.
Methods
We enrolled adult (>17 years old) patients admitted to our Level I trauma center within 6 h of severe TBI. ICP data were automatically captured and ICP 5-minute means were grouped into 12-hour time periods from admission (hour 0) to >7 days (hour 180). Means, maximum, percent time (% time), and pressure-times-time dose (PTD, mmHg h) of ICP >20 mmHg and >30 mmHg were calculated for each time period.
Results
From 2008 to 2010, we enrolled 191 patients. Only 2.1 % had no episodes of ICH. The timing of maximum PTD20 was relatively equally distributed across the 15 time periods. Median ICP, PTD20, %time20, and %time30 were all significantly higher in the 84–180 h time period than the 0–84 h time period. Stratified by functional outcome, those with poor functional outcome had significantly more ICH in hours 84–180. Multivariate analysis revealed that, after 84 h of monitoring, every 5 % increase in PTD20 was independently associated with 21 % higher odds of having a poor functional outcome (adjusted odds ratio = 1.21, 95 % CI 1.02–1.42, p = 0.03).
Conclusions
Although early elevations in ICP occur, ICPs are the highest later in the hospital course than previously understood, and temporal patterns of ICP elevation are associated with functional outcome. Understanding this temporal nature of secondary insults has significant implications for management.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Severe traumatic brain injury (TBI) remains the leading cause of death following injury [1, 2]. At present, little can be done to treat the primary insult to the brain that occurs at the time of injury; therefore, management of severe TBI aims to mitigate secondary insults, targeting prevention and treatment of intracranial hypertension (ICH) and cerebral hypoperfusion (CH), which are well-known to be associated with worse outcome [3–13]. ICH develops mainly through an increase in cerebral edema and/or evolution of intracranial hemorrhage [14], and published opinion describes ICH developing “1–3 days” [15], “2–3 days” [16], “3–5 days” [14, 17], and “1–2 weeks” [18] after injury. A phenomenon of “delayed ICH,” or “secondary intracranial pressure (ICP) rise,” is also described as occurring at 3–10 days following injury [19]. Remarkably little objective data are available in the literature that describe when ICH actually occurs following TBI.
Given that high-quality, continuous electronic monitoring data on ICP are now routinely captured in the neuro-trauma critical care setting, we asked whether these data could be collated to provide objective metrics of ICH in the first 180 h (7 days) following severe TBI and whether these metrics could be linked to patient outcome.
Methods
Patient Population
Patients admitted to the R Adams Cowley Shock Trauma Center (STC), a level I regional trauma center located in Baltimore, Maryland, were prospectively enrolled from 1/1/2008 to 12/30/2010. Inclusion criteria were: age >17 years; TBI verified by computed tomography (CT); placement of a clinically indicated ICP monitor—typically on the basis of Glasgow Coma Scale score [20] ≤6 and positive CT; and data captured by vital signs data recording system (VSDR). This study was approved by the Institutional Review Board of the University of Maryland School of Medicine Human Research Protections Office.
Baseline demographics and injury-specific data, including mechanism of injury, abbreviated injury scale (AIS) scores, Injury Severity Score (ISS) [21], and predicted survival by TRISS methodology [22] were recorded. Admission and post-resuscitation GCS and need for craniotomy were also recorded. Marshall classification scores [23] were assigned to all admission head CTs by a blinded reviewer. Outcome measures included in-hospital mortality, TBI mortality (defined as brain death), and length of hospital and intensive care unit (ICU) stay. The Extended Glasgow Outcome Score (GOSE) [24], dichotomized to good versus bad outcome, was used to evaluate long-term functional outcome at >3 months post-injury, when these scores were available. GOSE of 1–4 was considered as poor outcome; GOSE of 5–8 was considered as good outcome. When structured GOSE scores were unavailable, dichotomized good versus poor outcome was assigned to study subjects based on outpatient follow-up at >3 month from injury.
Patient Management Protocol
At the STC, patients with severe TBI are managed according to an institutional protocol based on the Brain Trauma Foundation Guidelines [3]. The protocol targets maintenance of ICP <20 mmHg and cerebral perfusion pressure (CPP) >60 mmHg with adequate sedation and analgesia, head elevation (30–45°), mechanical ventilation targeting a PaCO2 of 35–40 mmHg, and maintenance of normovolemia, normotension, and normoxia. Initial therapies for episodes of ICH (ICP > 20 mmHg) include: insertion of intraventricular catheter (IVC) (Codman, Raynham, MA), increasing doses of sedation, and/or hyperosmolar therapy with mannitol or hypertonic saline. Second tier therapies for intractable ICH include: moderate hyperventilation (PaCO2 < 35 mmHg), barbiturate coma induction, decompressive craniectomy, and/or decompressive laparotomy [25, 26]. CH (CPP < 60 mmHg) is managed with aggressive treatment of ICH, volume administration, and vasopressors as appropriate.
Data Processing
Our monitoring techniques and high-resolution automated VSDR methods have been reported previously [13, 27]. Briefly, the VSDR collects real-time patient vital signs (VS) from the networked patient monitors (GE-Marquette-Solar-7000/8000) throughout the trauma center, including every-6-second waveform capture, and the collected data are compressed and transferred to a centralized VSDR server. Potential artifacts are cleaned by removing the VS data of the first and last minute of patient stay and extreme outliers and calculation of a moving median with a window-size of five data points (30 s). The cleaning procedure discards less than 1 % of data points. For ICP monitored through an IVC, the ICP readings are distorted by periodic drainage. Therefore, for this work, the piecewise cubic Hermite interpolation method (Matlab 7.7 R2008b; Math-works, Natick, MA) was used to recalculate the estimated ICP curve [13]. The first peak of the reading between drainage periods was discarded unless the subsequent data point 6 s later was within 10 % range.
From these data, we calculated the 5-minute means of ICP and grouped them into 12-hour time periods from admission (hour 0) to 7.5 days (hour 180) giving 15 time periods for evaluation. Patient ICP data were only included in a 12-hour time period if more than >50 % of the 5-min mean values were available. Means and maximum (max) ICP values were calculated over each 12-hour time period for each study subject’s duration of monitoring. Percent time (% time) and pressure-times-time dose (PTD, expressed as mmHg h) [13] >20 mmHg (%time20, PTD20) and >30 mmHg (%time30, PTD30) were also calculated for each time period. ICH was defined as any PTD20 (pressure-times-time dose >20 mmHg h) recorded as >0 mmHg h in any given 12-hour time period. Patients were stratified by overall mortality, TBI-specific mortality (defined as brain death), and functional outcome at 3 months.
Statistical Analysis
Demographic data were summarized as percentages and means and standard deviation of the mean (SD) as appropriate. For non-normally distributed data, medians and interquartile ranges (IQR) were calculated. Student’s t test was used to compare means of continuous data. For non-normally distributed continuous data, we used the non-parametric Wilcoxon rank-sum statistic and, to compare timing of ICH and outcome, logistic regression. All models were adjusted for biologically plausible confounders including gender, age, polytrauma (defined as non-head ISS >15), admission GCS, and ISS. In multivariate analyses, groups were stratified by early ICH (0–84 h) and late ICH (>84 h) as defined by the occurrence PTD20 in one or more of the 15 successive 12-hour time periods after admission. The probability of results being due to chance (p) less than 0.05 was considered statistically significant for all tests.
Results
Based on the above criteria, we enrolled 191 patients. Table 1 shows the demographics, injury characteristics, and outcomes for study subjects. Overall in-hospital mortality was 22.5 % (43/191), including two individuals for whom the family elected to withdraw care. TBI-specific mortality was 3.7 % (3/191). At hospital discharge, 148/191 patients were still alive. Of these, 25 (16.9 %) were lost to follow-up and excluded from functional outcome analysis. Review of demographics, method and degree of injury, and hospital outcome data on these individuals suggest no significant differences from the study population on whom complete follow-up data were available. Of the 123 survivors in whom functional outcome at >3 months was available, 95 (77.2 %) had good functional outcome. Table 1 shows the study subjects’ characteristics stratified by outcome. p values recorded in the fifth column of the table reflect statistical comparisons of each characteristic between, respectively, all those who died (second column) and those who died of TBI (third column) and all who died (second column) versus those who survived (fourth column). p values recorded in the far right column reflect statistical comparison of each characteristic among survivors with good versus poor outcome.
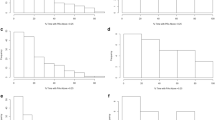
Available VS for the 191 study subjects yielded a total of 33,631 h (403,581 5-minute means) of data. Seventy patients had ICP data for more than 6 h (>50 %) for each of the 15 12-hour periods of monitoring. The total number of patients monitored at each time period is shown in Fig. 1, ranging from 191 patients at hours 12–24 to 71 patients at hours 168–180. Median ICP max for the study population over the 15 time periods of monitoring was 66.2 mmHg (IQR 24.6–40.1). Median mean ICP was 14.6 mmHg (IQR 9.8–18.2). Median %time20 was 10.4 % (IQR 2.1–31.3) and median %time30 was 0.8 % (IQR 0–5.3). Median PTD20 was 5.5 mmHg h (IQR 0.9–21.1) and median PTD30 was 0.32 mmHg h (IQR 0–3.3).

Proportion (%) of patients with intracranial hypertension (ICH) in each of the 15 successive 12-hour periods after admission. ICH is defined as pressure-times-time (mmHg h) dose (PTD) greater than 0
In actual clinical practice, patients without significant ICH typically have their ICP monitor removed earlier than those with ICH, so we first calculated the overall incidence of ICH in the study population. Only 4 of 191 patients (2.1 %) had no episodes of ICH, that is, no PTD20 recorded as greater than zero. Figure 1 shows the proportion of patients with ICH in each 12-hour period of monitoring. No differences were noted in the incidence of ICH in any given 12-hour period. Figure 2 shows, among the 70 total study subjects and 66 survivors for whom ICP data were available for the entire study period, the proportion of patients in any given 12-h period whose maximum PTD20 occurred in that period. Again, the percentage of patients whose maximum PTD20 occurred in any given 12-hour period was relatively equally distributed across the 15 12-hour periods.

Proportional distribution (%) of the occurrence of maximum pressure–time dose (PTD) of intracranial pressure (ICP) >20 mmHg among all patients (n = 70) and survivors (n = 66) over the 15 successive 12-hour periods after admission. Only includes patients with 7 full days of monitoring
Temporal patterns were noted in overall ICP elevation, as measured by mean and maximum elevation, %time20, %time3o, PTD20, and PTD30 across the 7 days of monitoring. As the data were non-normally distributed, medians were compared between the first 84 h (7 12-hour periods, 3.5 days) of monitoring and the subsequent 96 h (8 12-hour periods, 4 days) of monitoring. Median ICP, PTD20, %time20, and %time3o were all significantly higher in the 84—180-hour time period (Fig. 3).

Intracranial pressure (ICP, as mean and maximum median); intracranial pressure-times-time dose ≥20 mmHg hr (PTD20) and ≥30 mmHg hr (PTD30); and percent time ICP ≥20 mmHg (%time20) and ≥30 mmHg (%time30) in the first 84 h (<84 h) after admission versus the subsequent 4 days after admission (>84 h) * p < 0.01
In this study sample, ICH and mortality did not appear to be related. Compared to survivors, patients who died had no difference in median PTD20 (7.3 IQR 2.4–29.9 vs 7.6 IQR 2.4–16.0 mmHg h; p = 0.06) or PTD30 (1.4 IQR 0.4–6.1 vs 1.2 IQR 0.2–4.0 mmHg h; p = 0.05). Likewise, we noted no difference in median ICP max, mean ICP, %time20, or %time30 between survivors and those who died from any cause. Comparing the seven TBI deaths to the 148 survivors, only median ICP max was statistically different (68.9 IQR 51.5–69.5 vs 47.2 IQR 36.4–57.4 mmHg; p = 0.01). Patients who died in the hospital from any cause had no significant differences in temporal ICP patterns when compared to patients who survived to hospital discharge. Similarly, patients who died from their TBI had no temporal differences in ICPs over the 7 days of monitoring compared to survivors.
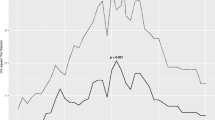
When we stratified the entire study cohort by functional outcome, including death among the levels of poor outcome, we saw no significant differences in overall ICP maximum, mean, % time, or PTD between those with good and those with poor functional outcome. Likewise, when stratified by good or bad functional outcome, survivors showed no significant differences in overall median ICP max, mean ICP, %time20, %time30, PTD20, or PTD30. However, survivors stratified by good or bad functional outcome did show dramatically different temporal patterns of ICP elevation (Fig. 4). Through the first 84 h of the study period, over the subsequent 96 h, it was essentially indistinguishable that survivors with poor functional outcomes had significantly greater PTD20. As assessed via multivariate analysis to control for baseline and injury characteristics, in the first 84 h after admission, higher PTD20 was not associated with functional status (adjusted odds ratio—aOR—1.01; 95 % CI 0.86–1.18; p = 0.9). However, in the 84—180-hour monitoring period, every 5 % increase in PTD20 was independently associated with 21 % greater odds of having a poor functional outcome (aOR 1.21; 95 % CI 1.02–1.42; p = 0.03).

Median pressure–time dose (PTD) of intracranial pressure (ICP) >20 mmHg h of survivors over 15 successive 12-hour periods after admission, stratified by functional outcome
Discussion
Despite conventional descriptions of the timing of ICH, remarkably little objective data have been published regarding the temporal arc of ICH after TBI. In this study, we used high-resolution continuous electronic ICP monitoring data to investigate the possible relationship of the timing of ICH to functional outcome after severe TBI. Not surprisingly, given the well-known association between malignant ICH and brain death, patients who died from their brain injury had higher maximum ICPs. However, we saw no association between overall dose or % time of ICP >20 mmHg and overall mortality or functional outcome, possibly as a consequence of sample size. We did find that survivors with poor functional outcomes at 3 months had a significant preponderance of ICH elevations in the second half of the first week of care (>84 h) when compared with those without such late-period elevations. Although maximum ICH was relatively evenly distributed among the first 7 days following injury, other measures of ICH, particularly % time above critical thresholds and dose, calculated as pressure-times-time, were significantly higher in the 84 to 180-hour time period of monitoring, when compared to the first 3½ days of monitoring, considerably later than has been understood. Our previous work suggests that pressure-times-time dose is both a more sensitive and a more specific marker of adverse outcome than more conventional ICP metrics [12, 13] and may at least partly explain our findings when compared with that of earlier researchers.
The objective measure of timing of the development and peak of ICH has important implications regarding not only duration of monitoring but also how we communicate with families about clinical deterioration. As noted by Stocchetti and colleagues [14], an appreciation for a more extended period of risk of ICH after TBI also has implications for interventional study design as a number of highly regarded randomized studies have only looked at the first 72 h of ICP control as a primary outcome measure [28, 29].
The evolution of increasing ICP over time following TBI has a number of potential sources [30]. Intracranial mass lesions causing elevated ICP tend to present relatively early following injury, as do ICP elevations from recurrent hemorrhage or progression of contusion [14, 31]. The development of cerebral edema following TBI is generally thought to begin immediately following the primary injury and then continue for 2–3 days [32]. Whether this edema is primarily vasogenic from blood–brain-barrier dysfunction or cytotoxic from increased cellular water content is a matter of significant debate in the literature [14, 16, 17, 30–32]. Regardless of the precise etiology of the edema, conventional opinion has been that this is a phenomenon that occurs soon after injury and reaches its peak within a few days. Delayed ICH has been reported [18, 19, 33] but typically as occurring in a minority of cases [19, 33]. The study by Stocchetti and colleagues cited above is the only one that specifically investigated the timing of elevations of ICP and found that mean ICP increased up to day 11 following injury. However, these researchers reported that only about 20 % of patients had their highest mean ICP after 5 days [14]. In our study, over 50 % of patients had their worst ICH after 84 h and 43 % of patients had their highest ICP after 5 days. These results are supported by earlier work from our institution looking at decompressive craniectomy for refractory ICH in which ~50 % of patients had their decompression done more than 3 days following injury [34]. Some of the differences seen in the current study over what has been reported previously may have to do with our use of automated continuous % time and PTD calculations as markers of ICH as opposed to just mean ICP or the highest recorded value which has been used in other studies [14, 32]. PTD, as captured by continuous automated VS recording, has been shown to be a better measure of ICH with respect to association with outcome [12, 13, 35]. Finally, iatrogenic, intensity-of-treatment factors may be involved, and we are actively exploring these issues in on-going work. However, as noted above, care at our center is highly protocolized and based on current Brain Trauma Foundation guidelines. If we were to establish a genuinely independent link between ICH and later-period treatment patterns, this will have important implications for ongoing clinical care quality assessment.
The association between ICH and functional outcome has been investigated with divergent results. Some studies have found that elevations in ICP are not associated with poor neuropsychological outcomes [36], while others have demonstrated significant short-term memory deficits in patients with ICP elevations [37]. Another study demonstrated an effect on memory function at 6 months which disappeared at 1 year following injury [38]. The association we found between temporal patterns of ICH and functional outcome has important implications. Whatever the source of this delayed ICH—more severe primary injury, less response to treatment, variations in treatment intensity, etc.—intensive prevention and treatment of ICP elevations are clearly indicated for longer than traditionally promulgated.
ICP >20 mmHg is the current threshold for active intervention [3], and detrimental effects of elevated ICP that occur above that level are well described [5]. The incidence of ICH in the current study was greater than 97 % in our severely brain injured study cohort. This is considerably higher than the 70 and 81 % reported elsewhere [5, 14]. The higher rates reported here are likely the result of differences in definition of ICH. In one study, ICH was defined as any ICP >20 mmHg for more than 5 min [14]. We chose to look at any episode of ICP >20 mmHg as our definition of ICH due to our previous work describing the detrimental effects of episodes of ICP >20 mmHg for even that short period of time [12]. In addition, probably due to disparate definitions, other studies have shown that the proportion of patients with ICH over each time period increased over the study period [14], whereas ours did not and remained relatively constant at 85–92 %.
Our work is clearly limited by a number of factors. The most obvious of these is sample size. Our inability to demonstrate statistically significant differences in a range of ICP metrics between those who died and those who lived is most likely due to this. In the current dataset, as noted above, we have not yet incorporated the concept of treatment intensity, which not only has important implications in management strategies but also important independent effects on the evolving physiology of injury. We are also limited in our ability to generalize our results to all TBI management as we have not included other critical markers of TBI progression and/or recovery such as clinical examination or CT findings. In addition, we examined only ICP as a measure of TBI severity. We did not examine other vital targets of TBI therapy like cerebral perfusion and cerebral oxygenation.
Conclusions
Despite numerous and diverse descriptions of the timing of ICH in the literature, little objective data accompany these descriptions. This study attempted to address that issue to provide some guidance about how long patients should undergo monitoring and what intensity of therapy may be indicated. Objective data on timing of ICH also help us communicate with families of TBI patients about expectations of disease progression. Although early ICH occurs, ICPs are the highest later in the hospital course than traditionally described. Patterns of ICP elevation are the same in the first 3–4 days but then differ significantly based on functional outcome. Understanding the temporal nature of secondary insults has significant implications into developing more evidence-based management approaches.
References
Sauaia A, Moore FA, Moore EE, et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38:185–93.
Dutton RP, Stansbury LG, Leone S, Kramer E, Hess JR, Scalea TM. Trauma mortality in mature trauma systems: are we doing better? An analysis of trauma mortality patters, 1197–2008. J Trauma. 2010;69(3):620–6.
Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons, Joint Section on Neurotrauma and Critical Care, AANS/CNS. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2007; 24 Suppl 1.S1–106.
Becker DP, Miller JD, Ward JD, Greenberg RP, Young HF, Sakalas R. The outcome from severe head injury with early diagnosis and intensive management. J Neurosurg. 1977;47:491–502.
Marmarou A, Anderson RL, Ward JD. Impact of ICP instability and hypotension on outcome in patients with severe head trauma. J Neurosurg. 1991;75:S59–66.
Narayan RK, Greenberg RP, Miller JD, et al. Improved confidence of outcome prediction in severe head injury. A comparative analysis of the clinical examination, multi-modality evoked potentials, CT scanning, and intracranial pressure. J Neurosurg. 1981;54:751–62.
Andrews PJ, Sleeman DH, Statham PF, et al. Predicting recovery in patients suffering from traumatic brain injury by using admission variables and physiological data: a comparison between decision tree analysis and logistic regression. J Neurosurg. 2002;97:326–36.
Clifton GL, Miller ER, Choi SC, Levin HS. Fluid thresholds and outcome from severe brain injury. Crit Care Med. 2002;30:739–45.
Juul N, Morris GF, Marshall SB, Marshall LF. Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury. The Executive Committee of the International Selfotel Trial. J Neurosurg. 2000;92:1–6.
Eisenberg HM, Frankowski RF, Contant CF, Marshall LF, Walker MD. High-dose barbiturate control of elevated intracranial pressure in patients with severe head injury. J Neurosurg. 1988;69:15–23.
Carter BG, Butt W, Taylor A. ICP and CPP: excellent predictors of long term outcome in severely brain injured children. Childs Nerv Syst. 2008;24:245–51.
Stein DM, Hu P, Brenner M, et al. Brief episodes of intracranial hypertension and cerebral hypoperfusion are associated with poor functional outcome following severe traumatic brain injury. J Trauma. 2011;71(2):364–74.
Kahraman S, Dutton RP, Hu P, et al. Automated measurement of “pressure times time dose” of intracranial hypertension best predicts outcome after severe traumatic brain injury. J Trauma. 2010;69:110–8.
Stochetti N, Colombo A, Ortolano F, et al. Time course of intracranial hypertension after traumatic brain injury. J Neurotrauma. 2007;24:1339–46.
Johnston IH, Johnston JA, Jennett B. Intracranial pressure changes following head injury. Lancet. 1970;1:433–6.
Donkin JJ, Vink R. Mechanisms of cerebral edema in traumatic brain injury: therapeutic developments. Curr Opin Neurol. 2010;23:293–9.
Marmarou A. Pathophysiology of traumatic brain edema: current concepts. Acta Neurochir. 2003;S86:S7–10.
Padayachy LC, Figali AA, Bullock MR. Intracranial pressure monitoring for traumatic brain injury in the modern era. Childs Nerv Syst. 2010;26:441–52.
Unterberg A, Kiening K, Schmiedek P, Lanksch W. Long-term observations of intracranial pressure after severe head injury. The phenomenon of secondary rise of intracranial pressure. Neurosurg. 1993;32:17–24.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81–4.
Baker SP, O’Neill B. The injury severity score: an update. J Trauma. 1976;16:882–5.
Boyd CR, Tolson MA, Copes WS. Evaluating trauma care: the TRISS method. Trauma Score and the Injury Severity Score. J Trauma. 1987;27:370–8.
Marshall LF, Marshall SB, Klauber MR, et al. The diagnosis of head injury requires a classification based on computed axial tomography. J Neurotrauma. 1992;9(Suppl 1):S287–92.
Wilson JTL, Pettigrew LEL, Teasdale GM. Structured interviews for the glasgow outcome scale and the extended Glasgow outcome scale: guidelines for their use. J Neurotrauma. 1998;15(8):573–85.
Joseph DK, Dutton RP, Aarabi B, Scalea TM. Decompressive laparotomy to treat intractable intracranial hypertension after traumatic brain injury. J Trauma. 2004;57(4):687–93.
Scalea TM, Bochicchio GV, Habashi N, et al. Increased intra-abdominal, intrathoracic, and intracranial pressure after severe brain injury: multiple compartment syndrome. J Trauma. 2007;62(3):647–56.
Kahraman S, Dutton RP, Hu P, et al. Heart rate and pulse pressure variability are associated with intractable intracranial hypertension after severe traumatic brain injury. J Neurosurg Anesthesiol. 2010;22(4):296–302.
Knoller N, Levi L, Shoshan I, et al. Dexanabinol (HU-211) in the treatment of severe closed head injury: a randomized, placebo-controlled, phase II clinical trial. Crit Care Med. 2002;30:548–54.
Maas AIR, Murray G, Henney H, et al. Efficacy and safety of dexanabinol in severe traumatic brain injury: results of a phase III randomized, placebo-controlled, clinical trial. Lancet Neurol. 2006;5:38–45.
Smith M. Monitoring intracranial pressure in traumatic brain injury. Anesth Analg. 2008;106(1):240–8.
Narayan RK, Maas AI, Servadei F, Tillinger MN, Marshall LF, Traumatic Intracerebral Hemorrhage Study Group. Progression of traumatic intracerebral hemorrhage: a prospective observational study. J Neurotrauma. 2008;25(6):629–39.
Unterberg AW, Stover J, Kress B, Kiening KL. Edema and brain trauma. Neuroscience. 2004;129:1021–9.
Bruce DA, Alavi A, Bilaniuk L, Dolinskas C, Obrist W, Uzzel B. Diffuse cerebral swelling following head injuries in children: the syndrome of “malignant brain edema”. J Neurosurg. 1981;54:170–8.
Barzό P, Marmarou A, Fatouros P, Hayasaki K, Corwin F. Contribution of vasogenic and cellular edema to traumatic brain swelling measured by diffusion-weighted imaging. J Neurosurg. 1997;87:900–7.
Sheth KN, Stein DM, Aarabi BA, et al. Intracranial pressure dose and outcome in traumatic brain injury. Neurocritical Care. 2013;18:26–32.
Lannoo E, Colardyn F, DeDeyne C, Vandekerckhove T, Jannes C, DeSoete G. Cerebral perfusion pressure and intracranial pressure in relation to neuropsychological outcome. Intens Care Med. 1998;24:236–41.
Uzzeli BP, Obrist WD, Dolinskas CA, Langfitt TW. Relationship of acute CBF and ICP findings to neuropsychological outcome in severe head injury. J Neurosurg. 1986;65:630–5.
Levin HS, Eisenberg HM, Gary HE, et al. Intracranial hypertension in relation to memory functioning during the first year after severe head injury. Neurosurgery. 1991;28(2):196–9.
Conflict of interest
None of the authors have any relevant financial interests to disclose.
Funding
Funded by W81XWH-07-2-0118.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stein, D.M., Brenner, M., Hu, P.F. et al. Timing of Intracranial Hypertension Following Severe Traumatic Brain Injury. Neurocrit Care 18, 332–340 (2013). https://doi.org/10.1007/s12028-013-9832-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-013-9832-3