
Abstract
Coma is an acute failure of neuronal systems governing arousal and awareness and represents a neurological emergency. When encountering a comatose patient, the clinician must have an organized approach to detect easily remedial causes, prevent ongoing neurologic injury, and determine a hierarchy of diagnostic tests, treatments, and neuromonitoring. Coma was chosen as an Emergency Neurological Life Support (ENLS) protocol because timely medical and surgical interventions can be life-saving, and the initial work-up of such patients is critical to establishing a correct diagnosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Coma is characterized by the absence of arousal (wakefulness, vigilance) and of awareness of self and environment [1]. Comatose patients have closed eyes, do not speak, and do not arouse to verbal, tactile, or noxious stimulus. Some causes of coma are readily identified while others may require extensive testing to discover an etiology.
Diagnostic and therapeutic steps should occur simultaneously. An organized and sequential plan can form the basis for discovering common causes of unresponsiveness and prioritizing studies for less common causes of coma [2].
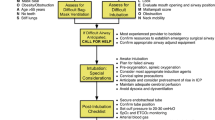
The Emergency Neurological Life Support (ENLS) suggested algorithm for the initial management of coma is shown in Fig. 1. Suggested items to complete within the first hour of evaluating a patient with coma are shown in Table 1.

ENLS coma protocol
Unresponsive Patient
Coma may be operationally defined as an eyes-closed state with reflexive, non-purposeful or absent responsiveness to environmental stimuli. The examiner determines the level of responsiveness with stimuli of increasing intensity. A verbal cue, such as “Are you OK?” or “What is your name?”, may be used first. Other auditory stimuli may include a handclap or other loud noises. Escalation of stimulation with tactile stimulation of body parts that have large cortical representations, such as the face, follow if needed.
If there is no clear response with these approaches, noxious stimuli may be applied that should be intense but not cause tissue injury. Recommended maneuvers include sternal rub, nail bed pressure, pressure applied to the supraorbital ridge, or pressure to the posterior aspect of the mandibular ramus. There is no evidence to support one maneuver over another.
An attempt by the examiner to open the eyelids of the patient is a simple test. Resistance by the patient to eyelid opening that increases with increasing effort by the examiner suggests a feigned or functional etiology of unresponsiveness. Another test of the veracity of unresponsiveness is arm-dropping; the patient’s arm, suspended over his or her face, is released. In a conscious patient without motor deficits, the falling arm will be moved and not contact the face.
ABCs and C-Spine
The unconscious patient’s airway, breathing and circulation should be quickly assessed and concurrently treated (see the Airway, Ventilation, and Sedation protocol). Ensuring patency of the airway is an overriding initial priority to allow oxygenation and ventilation. The patient’s cervical spine should be immobilized if there is a possibility of injury. A rapid initial survey should follow, looking for injury or other notable physical findings of the head and neck, chest, abdomen, and extremities.
Intravenous (IV) access should be established quickly. Bedside blood glucose testing should be performed in all unconscious patients. If the blood glucose is <70 mg/dL, 50 ml of 50 % dextrose should be administered intravenously. Thiamine (100 mg) should be given intravenously with the dextrose in patients at risk for nutritional deficiency (e.g., chronic ethanol users, bariatric surgery patients, patients with malabsorption states). If there is clinical suspicion of opioid toxicity (e.g., history of illicit drug use, apnea or bradypnea, small pupils), naloxone 0.4–2 mg IV should be administered and repeated as needed, up to 4 mg. Other antidotes, such as physostigmine, may be administered for anticholinergic toxicity in selected patients.
General and Neurologic Assessment
A general physical examination should be performed, including assessment of vital signs. If hypotension is present, the cause should be pursued while fluid repletion is started. Blood pressure elevation in the comatose patient may be a sign of an underlying life-threatening process, such as intracranial hypertension or stroke, which must be identified and treated. Recommendations for the management of blood pressure in stroke are discussed in the Ischemic Stroke protocol and in published guidelines [3]. A search for signs of trauma and other conditions that might require emergent surgical management are central goals of the initial survey.
The symmetry or focal nature of neurological findings is a critical differentiating characteristic in coma assessment. Asymmetric findings on physical examination suggest a focal brain lesion or disturbance. Unconscious patients with a unilateral dilated un-reactive pupil, asymmetric eye movements, or asymmetric motor responses should be rapidly evaluated with imaging to identify a potential herniation syndrome or stroke.
Symmetric posturing, either extensor (“decerebrate”) or flexor (“decorticate”), may occur in either structural or metabolic coma. Generalized or symmetric findings raise the possibility of a toxic or metabolic process, or a lesion involving brainstem or diencephalic arousal centers is a possibility. Psychoactive and anti-epileptic drugs have been associated with depressed vestibulo-ocular responses.
The neurological assessment of the unconscious patient has four parts [1]: level of consciousness, brainstem assessment, and assessment of motor and breathing patterns. Arousal is assessed by looking for spontaneous opening of the eyes, visual fixation or visual pursuit (tracking), and spontaneous and purposeful movements of the extremities.
The level of consciousness can be expressed quantitatively by the Glasgow Coma Scale (GCS) (see Table 2) [4]. The GCS is most valuable for trending sequential examination responses of a particular patient. However, the GCS has many limitations, as it does not account for alterations in brainstem function, hemiparesis, or aphasia. Moreover, patients with identical total GCS scores may have very different clinical presentations due to different combinations in the motor, visual, and eye sub-scores. Therefore, recording the total score and sub-scores is recommended. The Full Outline of Unresponsiveness (FOUR) score incorporates more detailed information on brainstem responses and has been validated in a variety of clinical settings [5, 6].
Testing of cranial nerves is valuable to assess the afferent limb of the reflex; brainstem nuclei and interconnections; and efferent tracts [2]. Brainstem responses include pupils (size, reactivity, and symmetry should be determined in all cases), corneal reflex, visual threat response, oculocephalic reflex (Doll’s eyes assessment only if no suspicion of cervical trauma or instability), vestibulo-ocular reflex (cold caloric testing), gag reflex, and cough reflex. Pinpoint pupils are suggestive of pontine damage, usually from hemorrhage or infarction. Enlarged and un-reactive pupils suggest damage to the midbrain or focal compression of the third nerve. Spontaneously roving eyes suggest cortical depression and an intact brainstem. Skew or dysconjugate resting gaze may occur with structural or metabolic processes. Jerky, nystagmoid movement may indicate non-convulsive status epilepticus. Fundoscopy may reveal retinal hemorrhages or papilledema, suggesting elevated intracranial pressure.
Cold caloric testing should only be performed after disease or trauma to the external auditory canal and tympanum have been ruled out. This is a reflex arc involving cranial nerve VIII, medial longitudinal fasciculus, parapontine reticular formation (pons), frontal eye field projections, and the efferent motor neurons of cranial nerves III and VI. In the comatose patient with functioning brainstem, afferent (VIII), and efferent (III, VI) cranial nerves, the response is that of tonic deviation of both eyes toward the side of cold irrigation. An asymmetric caloric response is consistent with a structural abnormality. Nystagmus is not seen in the comatose patient. In the patient who is awake, a rapid corrective eye deflection in the direction away from the stimulus, mediated via the frontal eye fields, is observed. Caloric testing may be helpful to unmask pseudocoma or psychogenic coma; presence of the corrective eye deflection is suggestive of wakefulness.
Motor function is assessed by observing any spontaneous movements or posturing, the motor response to verbal command, and the response to noxious stimulation. Muscle tone of the extremities may be assessed by passive movement of the limbs. The examiner should distinguish purposeful from reflex activity. Examples of purposeful activity include following of commands, pushing the examiner away, reaching for the tracheal tube, or localizing to noxious stimulation. Examples of reflexive activity include withdrawal, or abnormal flexion or extensor posturing to noxious stimulation. Deep tendon and cutaneous reflexes should be performed with particular attention to briskness and symmetry of findings.
Breathing patterns may have localizing value: after airway assessment and stabilization, breathing patterns observed may include central neurogenic hyperventilation from lesions of the pons or midbrain, or cluster (Biot’s) breathing from lesions of the pons. Medullary lesions are suggested by the absence of spontaneous breathing or ataxic breathing.
Following this initial assessment, unconscious patients should be triaged into likely structural or toxic–metabolic causes of coma—a critical early distinction, since structural coma may require emergent surgical intervention and/or invasive neuromonitoring (see Tables 3, 4).
Focused History/PMH
Historical information, elicited from witnesses, friends, family, co-workers, or emergency medical services (EMS) personnel, will often suggest the cause of coma. EMS personnel may have valuable details about the circumstances in which the patient was found, since they are trained to perform brief information gathering, including a quick search for pill bottles and any suicide notes, at the scene.
The time course of the alteration in consciousness may be helpful in suggesting an etiology. An abrupt onset of symptoms suggests a stroke, seizure, or a cardiac event with impaired cerebral perfusion. A more gradual onset of coma suggests a metabolic or possibly infectious process. Past medical, surgical, and psychiatric history; alcohol or illicit drug use history; and any environmental toxic exposures should be included in information gathering. Medication history is paramount; not only may this suggest a possibility of overdose, but current medications provide valuable clues to the medical history in the absence of any detailed information. The electronic medical record may provide rapid access to the patient’s past medical history if the patient can be reliably identified.
Stat Labs
Unless a readily reversible cause of unresponsiveness, such as hypoglycemia, has been discovered and corrected, additional laboratory work should be obtained. Serum chemistries, basic hematological panel, and blood gas analysis should be considered, as well as co-oximetry in selected patents. Toxicologic testing, such as ethanol level and urine toxicology screen, should be obtained (note that some toxins which cause unconsciousness are not detectable in common toxicologic screens, and that substances tested for in toxicologic screens vary among institutions). Microbiologic studies, including cultures of blood and urine may be helpful.
Initial Formulation: Structural, Non-Structural, or Unclear Causes of Coma
The differential diagnosis of coma is broad. Information obtained with initial stabilization, general physical examination, neurological assessment, focused history, and stat laboratory results will typically allow sorting of patients into likely structural or non-structural causes of coma and suggest whether and what additional testing is needed. If there is any concern for a structural etiology of coma, or if the cause of coma cannot be identified after initial assessment, cranial computed tomography (CT) should be sought immediately.
Brain Imaging
Non-contrast cranial CT should be obtained emergently in unconscious patients with presumed structural cause of coma and in patients with an unclear cause of coma after initial assessment. CT allows discovery of potential causes such as focal hypodensity suggestive of a cerebral infarct; intracranial hemorrhage; brain mass; brain edema; and acute hydrocephalus.
If acute ischemic stroke is being considered, CT angiography and CT perfusion can provide valuable information on the cerebral vasculature and regional perfusion. Non-contrast CT imaging in the hyperacute phase of ischemic stroke is often normal; in this setting, clinical diagnosis of stroke is still valid. Ischemic stroke does not typically cause coma acutely unless it occurs within arousal systems located in the brainstem or diencephalon (e.g., basilar artery thrombosis); sub-acutely, coma may develop due to progression of a hemispheric infarct with transtentorial herniation. When a central nervous system (CNS) infection is being considered, cranial CT with and without contrast may be ordered to evaluate for abscess, extra-axial fluid collections, hydrocephalus, hemorrhagic changes, and infarctions prior to lumbar puncture and cerebrospinal fluid analysis.
Non-structural Coma
Common non-structural causes of coma include anoxic-ischemic encephalopathy, seizures, metabolic alterations, endocrinopathies, systemic infections, CNS infections, overdose of medications, illicit drug and alcohol use, and exposure to toxins (Table 4). Treatment is guided by the underlying etiology.
Where appropriate, specific antagonists or antidotes should be administered. For example, the opioid toxidrome should prompt administration of naloxone as discussed in the ABCs and C-Spine section above. Acetaminophen ingestion is treated with N-acetylcysteine. In some cases, a metabolic encephalopathy may evolve toward a structural process, such as such as acute liver failure leading to cerebral edema and herniation.
In patients with new seizures or change in seizure pattern, a structural cause must be carefully searched for with CT and magnetic resonance imaging (MRI) if the CT is negative. CNS infections, such as bacterial meningitis, may have no structural correlation present on contrast CT scan (though the test should be obtained to exclude brain abscess). Where there is high suspicion of acute bacterial meningitis, appropriate antibiotics and dexamethasone should be administered before CT and lumbar puncture.
Persisting Uncertainty
If diagnostic uncertainty persists after initial diagnostic steps, non-contrast CT scan should be obtained. Lumbar puncture is performed if there is suspicion of CNS infection, inflammation, or complications of lymphoma or other cancers. In addition, when there is clinical suspicion of subarachnoid hemorrhage, lumbar puncture should be obtained if the CT is negative for subarachnoid hemorrhage. MRI is obtained if there is a presumption of hyperacute ischemic stroke or when the cause of coma is not explained by other tests.
A few less common causes of coma deserve special mention. Non-convulsive status epilepticus may be suspected if there is a seizure history or if a seizure was observed in the clinical course. There may be subtle physical examination findings, such as an eyelid twitch or finger movement, but the patient does not have tonic–clonic activity. In these cases, EEG is required for diagnosis.
Cerebellar hemorrhage may cause rapid unresponsiveness from brainstem compression. A history of sudden headache followed by inability to walk, or severe nausea and vomiting, may be key to diagnosis. Non-contrast CT is diagnostic.
Ischemic stroke involving the basilar artery may produce sudden unresponsiveness [7]. Abnormal eye findings may be present on examination. CT-angiography may reveal the basilar clot, and the non-contrast CT may show a hyperdense basilar artery.
Communication
When communicating to an accepting or referring physician about this patient, consider including the key elements listed in Table 5.
References
Plum F, Posner JB. The diagnosis of stupor and coma. 3rd ed. Philadelphia: F. A. Davis Co; 1980.
Stevens RD, Bhardwaj A. Approach to the comatose patient. Crit Care Med. 2006;34:31–41.
Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115:e478–534.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Wijdicks EF, Rabinstein AA, Bamlet WR, Mandrekar JN. FOUR score and Glasgow Coma Scale in predicting outcome of comatose patients: a pooled analysis. Neurology. 2011;77:84–5.
Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: the FOUR score. Ann Neurol. 2005;58:585–93.
Ferbert A, Bruckmann H, Drummen R. Clinical features of proven basilar artery occlusion. Stroke. 1990;21:1135–42.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huff, J.S., Stevens, R.D., Weingart, S.D. et al. Emergency Neurological Life Support: Approach to the Patient with Coma. Neurocrit Care 17 (Suppl 1), 54–59 (2012). https://doi.org/10.1007/s12028-012-9755-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9755-4