
Abstract
Background
In patients with acute intracerebral hemorrhage (ICH), reduced platelet activity on admission predicts hemorrhage growth and poor outcomes. We tested the hypotheses that platelet transfusion improves measured platelet activity. Further, we hypothesized that earlier treatment in patients at high risk for hemorrhage growth and poor outcome would reduce follow-up hemorrhage size and poor clinical outcomes.
Methods
We prospectively identified consecutive patients with ICH who had reduced platelet activity on admission and received a platelet transfusion. We defined high-risk patients as per a previous publication, reduced platelet activity, or known anti-platelet therapy (APT) and the diagnostic CT within 12 h of symptom onset. Platelet activity was measured with the VerifyNow-ASA (Accumetrics, CA), ICH volumes on CT with computerized quantitative techniques, and functional outcomes with the modified Rankin Scale (mRS) at 3 months.
Results
Forty-five patients received a platelet transfusion with an increase in platelet activity from 472 ± 50 (consistent with an aspirin effect) to 561 ± 92 aspirin reaction units (consistent with no aspirin effect, P < 0.001). For high-risk patients, platelet transfusion within 12 h of symptom onset, as opposed to >12 h, was associated with smaller follow-up hemorrhage size (8.4 [3–17.4] vs. 13.8 [12.3–62.5] ml, P = 0.04) and increased odds of independence (mRS < 4) at 3 months (11 of 20 vs. 0 of 7, P = 0.01). There were similar results for patients with known APT.
Conclusions
In patients at high risk for hemorrhage growth and poor outcome, early platelet transfusion improved platelet activity assay results and was associated with smaller final hemorrhage size and more independence at 3 months.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Intracerebral hemorrhage (ICH) is frequently deadly or disabling, and has no approved treatment. Hemorrhage growth occurs in nearly one-third of patients, often occurs within hours of symptom onset [1], and is associated with increased morbidity and mortality [2]. Studies of acute treatment of ICH such as acute blood pressure control [3] and activated factor VII [4] necessarily focus on reducing hemorrhage growth as the proximate mechanism. The time from symptom onset to treatment is vital, with earlier treatment potentially able to prevent more hemorrhage growth.
The use of anti-platelet therapy (APT, e.g., aspirin or clopidogrel) and reduced platelet activity are associated with more intracranial bleeding and increased mortality in patients with ICH [5–7]. Reduced platelet activity is associated with hemorrhage growth and poor outcome in patients with a diagnostic CT within 12 h of ICH symptom onset [8]. Based on these data, platelet transfusion may be considered an experimental therapy for acute ICH [9, 10].
Patients with reduced coagulation factors (typically due to warfarin therapy) may be treated with fresh frozen plasma, prothrombin complex concentrates, and vitamin K, and the INR may be repeated until within the normal range [11]. Platelet transfusion may be an analogous treatment for patients who present with bleeding and reduced platelet activity. The recent ingestion APT might inactivate transfused platelets, so there is a need to verify an in vivo effect.
Safety of platelet transfusion is a separate concern: complications of packed red blood cell transfusion are well described [12], but complications after platelet transfusion other than sepsis [13] and alloimmunization [14] (and in patients without primary hematologic disease) have received less attention. We tested the hypothesis that platelet transfusion would lead to a change in measured platelet activity in patients with ICH, while prospectively collecting data on the incidence of adverse events. Further, we tested the hypotheses that earlier treatment would lead to smaller follow-up hemorrhage size and more frequent functional independence at follow-up in patients at high risk for hemorrhage growth and poor outcome.
Methods
Study Population
We prospectively enrolled consecutive patients with ICH and analyzed those who received a platelet transfusion. Patients with thrombocytopenia (platelet count < 100,000 per microliter), an inherited platelet defect, ICH due to trauma, ruptured aneurysms, arteriovenous malformation, vasculitis, or structural lesions were excluded. All patients were diagnosed by a board-certified vascular neurologist (RAB) or neurosurgeon (HHB) with confirmation by CT. Clinical data, laboratory data, and follow-up were prospectively recorded. The study was approved by the Institutional Review Board (IRB). Written informed consent to collect data and clinical outcomes was obtained from the patient or a legally authorized representative with the following exceptions: the patient died in hospital or no representative could be located for an incapacitated patient (in which case the IRB approved collection of data in a registry without consent), and in three patients who declined consent to record identifiers, where anonymous data through hospital discharge only were collected.
Medication Reconciliation
A dedicated ICU pharmacist reviewed the medication history with the patient (if able to provide this information) or next of kin as part of a mandatory medication reconciliation process [15]. We prospectively recorded the dose of aspirin and the use of clopidogrel or warfarin.
Assessment of Platelet Activity
We routinely measured platelet activity on admission and an hour after platelet transfusion. The VerifyNow-ASA (Accumetrics, CA) uses an optical detection system that measures platelet-induced aggregation as an increase in light transmittance. Citrated whole blood is exposed to lyophilized human fibrinogen-coated beads. Cationic propyl gallate is used to induce platelet activation without fibrin formation. The results are reported as aspirin reaction units (ARU), with ≤550 ARU indicative of reduced platelet activity due to aspirin.
Platelet Transfusion and Adverse Events
Platelet transfusion was given at the discretion of the attending physician. We prospectively recorded when a platelet transfusion was given and adverse events within 6 h: new core temperature of at least 100.4 F, new symptomatic dyspnea or radiographic pulmonary edema (within 24 h, correlated with the official interpretation), hypotension (systolic blood pressure < 100 mm Hg, new vasopressor requirement, or increase in pre-existing vasopressor dose by at least 25%), rash, or bacteremia attributable to transfusion.
Critical Care
Critically ill patients in the Neuro/Spine-ICU are cared for by a dedicated multi-disciplinary team including attending medical staff, house officers, an ICU pharmacist and critical care nurses. We followed published guidelines in place [16] for the management of blood pressure, routinely measured with an arterial catheter.
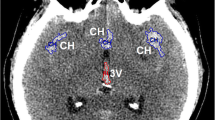
ICH Volume Calculations
ICH volumes on CT scan were computed with quantitative techniques, as previously described [8]. We prospectively recorded functional outcomes with the modified Rankin Scale (mRS) at 3 months a validated questionnaire [17, 18]. In brief, the mRS is assessed as 0 (no symptoms), 1 (no disability), 2 (mild disability), 3 (moderately severe disability and independent with a device), 4 (not independent), 5 (bed bound), or 6 (dead). Independence with a device or better at 3 months was defined as scores of <4, the standard used for earlier clinical trials of ICH [4].
Statistical Analysis
Normally distributed data are presented as mean ± SD, non-normally distributed data as median [Q1–Q3]. Data were compared with ANOVA (blood pressure between groups), paired t test (for repeated platelet activity measurements), Mann–Whitney U (for non-parametric statistics), χ2 (for categorical variables), or Fisher’s exact test (categorical variables where some assumptions of χ2 were not met) as appropriate. Calculations were performed with standard commercial software (PASW v. 18, IBM, Armonk, NY).
Results
There were 45 patients in the cohort. Seventeen (37%) patients received one pack (six “units”) of apheresis platelets in one transfusion, thirteen (28%) received more than one pack in a single transfusion, thirteen (28%) received two transfusions, and the remainder more than two transfusions. Demographics of the patient population are presented in Table 1. Patients with known APT use had reduced platelet activity on admission, 487 [445–531] ARU.
Platelet Activity
Platelet transfusion was associated with improved platelet activity after treatment, from 472 ± 50 to 561 ± 92 ARU (P < 0.001) after the first transfusion. The median pre-treatment result was consistent with an aspirin effect, while the post-treatment result was consistent with no aspirin effect. The median time to platelet transfusion was 10 [6.3–21] hours from symptom onset. Documented APT use was not associated with the change in the assay with platelet transfusion (P > 0.1). Platelet activity before and after platelet transfusion were not correlated to the number of platelet packs given (P > 0.1).
Adverse Events of Platelet Transfusion
Eight (16%) transfusions preceded an acute adverse event, hypotension in five and new fever in three. There were no instances of transfusion-related bacteremia, respiratory distress, or pulmonary edema.
Platelet Transfusion and Outcomes
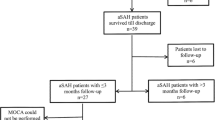
We further examined 32 patients we previously described as at particularly high risk for hemorrhage growth and poor outcome [8], namely, those patients with platelet activity ≤550 ARU and the diagnostic CT within 12 h of symptom onset. We classified these patients as receiving a platelet transfusion within 12 h of symptom onset, or after 12 h. The groups had similar age, severity of ICH, time to presentation, and blood pressure at baseline (Table 2). Similar results were obtained when platelet transfusion was categorized as within 6 h of symptom onset, 6–12 h, or after 12 h. The three patients also known to take warfarin all received a platelet transfusion within 12 h, one of whom died before 14 days (all had complete follow-up data). Excluding these patients did not meaningfully affect the analysis.
We repeated the analysis in patients with known APT use and the diagnostic CT within 12 h of symptom onset (i.e., substituting known APT use for reduced platelet activity), with similar results. Although, the number of patients was smaller (ten received a transfusion within 12 h, and five after 12 h of symptom onset), the results and significance were similar for initial hemorrhage size, final hemorrhage size, and dependence at 3 months.
Mortality and Withdrawal of Life Support
Fourteen patients died. Death occurred 8.8 [2.6–23.3] days after ICH symptom onset. One patient was dead by neurologic criteria 3.6 days after symptom onset, 2 had a cardiac arrest at median 5.7 days, 7 had withdrawal of life support at the request a legally authorized representative at 5.7 [3.6–11.1] days, and 4 died of other medical causes at 28.5 [23.3–37.3] days (P = 0.04 for difference in time to death between groups). The timing of platelet transfusion was not related to the mechanism of death, or time to death (P > 0.1).
Discussion
We found that platelet transfusion led to significant changes in platelet activity assays for patients with ICH and reduced platelet activity. Overall, platelet transfusion increased platelet activity from a measure consistent with an aspirin effect to one without aspirin effect, indicating a likely biologic effect of platelet transfusion. In patients, we previously identified as high risk for hemorrhage growth and poor outcome, platelet transfusion within 6 or 12 h of symptom onset was associated with smaller final hemorrhage size and improved odds of independence at 3 months. These preliminary data support the use of platelet transfusion as a potential treatment for ICH, but raise important concerns for patient safety and future research.
We used a point-of-care assay that has performed well compared to platelet aggregometry, the usual reference standard [19, 20]. This assay has low cost per use, can be repeated on demand after interventions, and does not require specialized technical personnel. Bleeding times have been a traditional bedside measure of platelet activity [14], however, they are no longer used at most institutions because of poor inter-rater reliability, potential scar formation, and discomfort to the patient and/or family.
Patients known to take APT reliably had low platelet activity. Restricting the analysis to patients with known APT use led to similar results, so known APT use might be a reasonable inclusion criterion for future research if platelet activity assay results are not available in a timely fashion. Two such studies are now underway [10, 21]. Ibuprofen and other NSAIDs might reasonably be taken for a new headache and affect measured platelet activity [22], but there is no other way to reliably detect their use in routine clinical care, and such patients might be missed without point-of-care testing (this is why we enrolled more patients with reduced platelet activity than known APT use). Patients with ICH often have depressed mental status or aphasia and are unlikely to be able to give a reliable medication history for over-the-counter medication. We are unlikely to be detecting patients with inherited disorders of platelet activity (e.g., von Willebrand disease) presenting with ICH because it is quite rare.
We found that while platelet transfusion is effective in increasing measured platelet activity, it is not an ideal agent for improving platelet activity due to a significant rate of acute adverse events. Hypotension could lead to cerebral ischemia [23], and fever has been linked to worse outcome in patients with acute ICH [24]. In addition, donor platelets cannot be collected to meet demand, and routine use for ICH might strain blood bank resources. We do not have data on other agents that might alter measured platelet activity, such as desmopressin or recombinant factor VII, although this might be studied in selected patients. We did not perform a controlled trial where patients had repeat platelet activity measurements after placebo or no treatment at a specified time, but such data would be helpful to clearly show interventions improve platelet activity in patients with ICH.
Other observational data have not found an association between platelet transfusion and improved outcomes in patients with ICH [25], but there was no specified maximum time to treatment or computerized volumetric data. One would expect earlier treatment to be more likely to improve outcomes, although we found similar results stratifying treatment as up to 6 h, or 12 h from symptom onset.
Mortality and poor outcome in ICH may be related to self-fulfilling prophecies and fewer medical interventions [26, 27]. We only examined patients who received a platelet transfusion because the decision not to transfuse may have indicated less aggressive care. The decision to transfuse platelets indicates a decision that the patient is likely to be salvageable, and we did not find any evidence that platelet transfusion after 12 h from symptom onset was associated with more frequent withdrawal of life support. Patients who received a platelet transfusion after 12 h had a higher rate of craniotomy for surgical decompression, so there is no reason to suspect these patients were not treated as intensely as those who received platelet transfusion within 12 h.
The reason for any delay in platelet transfusion is not clear, but variability in timing likely relates to the lack of a defined protocol for platelet transfusion. This is a potential source of bias, and prospective trials with a defined time to treatment are necessary to remove it. We are not the only institution to routinely transfuse platelets for patients with known APT use who have ICH or require a craniotomy, but multi-center data are lacking. Our data suggest that point-of-care testing of platelet activity would increase the number of patients who could be identified as having ingested APT around the time of ICH symptom onset.
Although data were collected prospectively, treatment was not randomized and the number of patients is too small for a robust multivariate analysis. The concordance of smaller final hemorrhage size and improved 3 month outcomes with earlier platelet transfusion lends credence to our findings and to proposed studies of platelet transfusion for acute ICH. These data do raise the concern of a substantial rate of serious adverse events related to platelet transfusion, however, and other platelet-activating therapies might be considered.
While admission blood pressure was similar between groups and routinely managed according to standard guidelines, we did not analyze blood pressure at multiple time points. Blood pressure and its control is a potential confounder of ICH volume growth [3], and should be controlled for in future research.
The use of warfarin might complicate our results because warfarin is associated with hematoma growth and worse outcomes in patients with ICH. All patients with known warfarin use received an early platelet transfusion, which would be expected to bias the results against a beneficial effect of platelet transfusion. Excluding these three patients did not affect the analysis.
At 3-months follow-up, we were able to locate 27 of 32 (84%) patients at high risk for hematoma expansion and poor outcome. It is possible that complete follow-up might have diminished the difference between groups.
In sum, we found platelet transfusion improved measured platelet activity, and platelet transfusion within 12 h of symptom onset was associated with reduced final hemorrhage size and increased odds of independence at 3 months. Clinical trials of platelet transfusion, or another platelet-activating therapy, are justified for acute ICH.
References
Brott T, Broderick J, Kathari R, Tomsick T, Sauerbeck L, Spilker J, Duldner J, Khoury J. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke. 1997;28:1–5.
Davis SM, Broderick J, Hennerici M, Brun NC, Diringer MN, Mayer SA, Begtrup K, Steiner T, Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology. 2006;66:1175–81.
Anderson C, Huang Y, Wang J, Arima H, Neal B, Peng B, Heeley E, Skulina C, Parsons M, Kim J, Tao Q, Li Y, Jiang J, Tai L, Zhang J, Xu E, Cheng Y, Heritier S, Morgenstern L, Chalmers J. Intensive blood pressure reduction in acute cerebral haemorrhage trial (interact): a randomised pilot trial. Lancet Neurol. 2008;7:391–9.
Mayer SA, Brun NC, Broderick J, Davis S, Diringer MN, Skolnick BE, Steiner T. Efficacy and safety of recombinant activated factor vii for acute intracerebral hemorrhage. New Engl J Med. 2008;358:2127–37.
Roquer J, Rodriguez-Compello A, Gomis M, Ois A, Munteis E. Previous anti-platelet therapy is an independent predictor of 30-day mortality after spontaneous supratentorial intracerebral hemorrhage. J Neurol. 2005;252:412–6.
Saloheimo P, Ahonen M, Juvela S, Pyhtinen J, Savolainen E, Hillborm M. Regular aspirin use preceding the onset of primary intracerebral hemorrhage is an independent predictor for death. Stroke. 2006;37:129–33.
Thompson BB, Bejot Y, Caso V, Castillo J, Christensen H, Flaherty ML, Foerch C, Ghandehari K, Giroud M, Greenberg SM, Hallevi H, Hemphill JC 3rd, Heuschmann P, Juvela S, Kimura K, Myint PK, Nagakane Y, Naritomi H, Passero S, Rodriguez-Yanez MR, Roquer J, Rosand J, Rost NS, Saloheimo P, Salomaa V, Sivenius J, Sorimachi T, Togha M, Toyoda K, Turaj W, Vemmos KN, Wolfe CD, Woo D, Smith EE. Prior antiplatelet therapy and outcome following intracerebral hemorrhage: a systematic review. Neurology. 2010;75:1333–42.
Naidech AM, Jovanovic B, Liebling S, Garg RK, Bassin SL, Bendok BR, Bernstein RA, Alberts MJ, Batjer HH. Reduced platelet activity is associated with early clot growth and worse 3-month outcome after intracerebral hemorrhage. Stroke. 2009;40:2398–401.
Morgenstern LB, Hemphill JC, Tamargo RJ, Anderson C, Becker K, Broderick JP, Connolly ES, Greenberg SM, Huang JN, MacDonald RL, Messe SR, Mitchell PH, Selim M. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2010;41:2108–29.
de Gans K, de Haan RJ, Majoie CB, Koopman MM, Brand A, Dijkgraaf MG, Vermeulen M, Roos YB. Patch: platelet transfusion in cerebral haemorrhage: study protocol for a multicentre, randomised, controlled trial. BMC Neurol. 2010;10:19.
Goldstein JN, Rosand J, Schwamm LH. Warfarin reversal in anticoagulant-associated intracerebral hemorrhage. Neurocrit Care. 2008;9:277–83.
Vlaar APJ, Binnekade JM, Prins D, van Stein D, Hofstra JJ, Schultz MJ, Juffermans NP. Risk factors and outcome of transfusion-related acute lung injury in the critically ill: a nested case–control study. Crit Care Med. 2010;38:771–8.
Morrow JF, Braine HG, Kickler TS, Ness PM, Dick JD, Fuller AK. Septic reactions to platelet transfusions. JAMA. 1991;266:555–8.
Platelet transfusion therapy—consensus conference. JAMA. 1987;257:1777–80.
Sorimachi T, Fujii Y, Morita K, Tanaka R. Predictors of hematoma enlargement in patients with intracerebral hemorrhage treated with rapid administration of antifibrinolytic agents and strict blood pressure control. J Neurosurg. 2007;106:250–4.
Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, Mayberg M, Morgenstern L, Ogilvy CS, Vespa P, Zuccarello M. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38:2001–23.
Wilson JTL, Hareendran A, Grant M, Baird T, Schulz UGR, Muir KW, Bone I. Improving the assessment of outcomes in stroke: use of a structured interview to assign grade on the modified Rankin scale. Stroke. 2002;33:2243–6.
Banks J, Marotta C. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091–6.
Karon B, Wockenfus A, Scott R, Hartman S, McConnell J, Santrach P, Jaffe A. Aspirin responsiveness in healthy volunteers measured with multiple assay platforms. Clin Chem. 2008;54:1060–5.
Lordkipanidze M, Pharand C, Schampaert E, Turgeon J, Palisaitis D, Diodati J. A comparison of six major platelet function tests to determine the prevalence of aspirin resistance in patients with stable coronary artery disease. Eur Heart J. 2007;28:1702–8.
Hillbom M, Huhtakangas J. Platelet transfusion in acute intracerebral hemorrhage. Clinicaltrials.Gov number nct00699621. Available at http://www.clinicaltrials.gov/ct2/show/NCT00699621?term=platelet+transfusion+intracerebral+hemorrhage&recr=Open&rank=1. Accessed 25 July 2008.
Goldenberg NA, Jacobson L, Manco-Johnson MJ. Brief communication: duration of platelet dysfunction after a 7-day course of ibuprofen. Ann Intern Med. 2005;142:506–9.
Vespa PM. Blood pressure after intracerebral hemorrhage: lower may not be safer. Crit Care Med. 2010;38:731–2.
Schwarz S, Hafner K, Aschoff A, Schwab S. Incidence and prognostic significance of fever following intracerebral hemorrhage. Neurology. 2000;54:354–61.
Creutzfeldt CJ, Weinstein JR, Longstreth WT Jr, Becker KJ, McPharlin TO, Tirschwell DL. Prior antiplatelet therapy, platelet infusion therapy, and outcome after intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2009;18:221–8.
Zahuranec DB, Brown DL, Lisabeth LD, Gonzales NR, Longwell PJ, Smith MA, Garcia NM, Morgenstern LB. Early care limitations independently predict mortality after intracerebral hemorrhage. Neurology. 2007;68:1651–7.
Becker KJ, Baxter AB, Cohen WA, Bybee HM, Tirschwell DL, Newell DW, Winn HR, Longstreth WT Jr. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology. 2001;56:766–72.
Acknowledgments
Northwestern University has applied for a use patent on desmopressin for the treatment of ICH based on peer-reviewed manuscripts by AMN; it is unclear if this has any financial value. The Office of Research at Northwestern University has determined that this does not pose a financial conflict of interest.
Conflict of interest
Andrew M. Naidech has received unrelated research support from Gaymar, Inc and Astellas Pharma US, and the Northwestern Memorial Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naidech, A.M., Liebling, S.M., Rosenberg, N.F. et al. Early Platelet Transfusion Improves Platelet Activity and May Improve Outcomes After Intracerebral Hemorrhage. Neurocrit Care 16, 82–87 (2012). https://doi.org/10.1007/s12028-011-9619-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9619-3