
Abstract
Background
Advances in intensive care medicine have increased survival rates of patients with critical neurological conditions. The focus of prognostication for such patients is therefore shifting from predicting chances of survival to meaningful neurological recovery. This study assessed the variability in long-term outcome predictions among physicians and aimed to identify factors that may account for this variability.
Methods
Based on a clinical vignette describing a comatose patient suffering from post-anoxic brain injury intensivists were asked in a semi-structured interview about the patient’s specific neurological prognosis and about prognostication in general. Qualitative research methods were used to identify areas of variability in prognostication and to classify physicians according to specific prognostication profiles. Quantitative statistics were used to assess for associations between prognostication profiles and physicians’ demographic and practice characteristics.
Results
Eighteen intensivists participated. Functional outcome predictions varied along an evaluative dimension (fair/good–poor) and a confidence dimension (certain–uncertain). More experienced physicians tended to be more pessimistic about the patient’s functional outcome and more certain of their prognosis. Attitudes toward quality of life varied along an evaluative dimension (good–poor) and a “style” dimension (objective–subjective). Older and more experienced physicians were more likely to express objective judgments of quality of life and to predict a worse quality of life for the patient than their younger and less experienced counterparts.
Conclusions
Various prognostication profiles exist among intensivists. These may be dictated by factors such as physicians’ age and clinical experience. Awareness of these associations may be a first step to more uniform prognostication.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Neurological injury is a major cause of long-term morbidity for patients admitted to intensive care units (ICU). It has been estimated that one-third of patients admitted to the ICU suffer from neurological syndromes detrimental to their health outcome [1]. Ongoing advances in critical care medicine have resulted in an ever increasing ability to preserve life in these critically ill patients. These advances have shifted the focus of prognostication in the ICU for a large proportion of patients from chance of survival to chance of survival with a meaningful neurological recovery. As a result, meetings with family members of ICU patients often center on predictions of long-term neurological outcome. Clear communication of accurate prognostic information during these meetings is vital for informed decision-making and has been identified as a crucial aspect of neurocritical care and a duty of physicians [2]. Prognostication is not an exact science, however. Opinions regarding patients’ prognosis may differ among physicians which can create challenges for end-of-life (EOL) decision-making [3, 4].
This hypothesis-generating study aimed to assess potential variability in prognostication among physicians and gain insight into factors that may account for this variability. We approached this task in two steps. First we sought to identify prognostic profiles that exist among physicians by analyzing physicians’ responses to a semi-structured interview centered on a clinical vignette of a comatose patient. Qualitative content analysis was used to identify prognostic profiles in an open way without restricting the approach to a priori categories. Secondly, using standard statistical approaches, we searched for specific associations between prognostic profiles and physician characteristics such as clinical experience, age, gender, and medical subspecialty to generate hypotheses.
Methods
All neurointensivists and general medicine intensivists at two tertiary hospitals were invited to participate in this study. Hospitals were selected for both theoretical (e.g., presence of neurointensivists) and practical (e.g., geographical proximity) reasons. Physicians were identified based on information provided by heads of clinical units and contact information available online. Up to two phone calls and two email invitations were sent. Research ethics approval from both participating institutions was obtained.
Responding intensivists participated in this two-part study involving a questionnaire and a semi-structured interview. The questionnaire surveyed for age, gender, ethnicity (as defined by American census categories), medical specialty and sub-specialty, and clinical experience. Physicians then read a clinical vignette featuring the case of a comatose patient suffering from post-anoxic brain injury (Table 1) and participated in a semi-structured two-part audio-taped interview which lasted approximately for 45 min. During the first part of the interview, respondents were asked to present and discuss their perceived prognosis and expected outcome for the patient described in the vignette. The questions were: What is the prognosis and outcome for this patient? What is the projected quality of life for this patient? What physical, mental, and social deficits is the patient likely to experience if treatment succeeds? The second part of the interview explored four sets of fundamental factors that can influence physician decision-making: professional experience; personal background; patient characteristics; and contextual factors. Physicians were asked to rate those factors from 1 (most important) to 4 (least important). We then guided the interview to further explore these four topics using specific sub-questions. All interviews were transcribed verbatim and subsequently analyzed using the QSR Nvivo 7 (Doncaster, Australia) qualitative software package. Using a (conventional) thematic qualitative content analysis approach, a coding scheme was generated [5–7]. This is called the “open-coding” phase and involved iterative readings and analysis of a diversified sample of interviews. This open coding then set the way for “axial coding” where all codes are applied to all of the interviews. One author (M-JD) first coded the material, another (ER) reviewed all coding; disagreements were discussed, and consensus was achieved. This enabled us to identify domains of prognostic variability and to determine specific prognostication profiles. Associations between these prognostication profiles and physicians’ demographic and practice characteristics were then examined using the Mann U Whitney test for continuous variables and Fisher’s exact test for categorical variables. Results were interpreted as statistically significant at an alpha of 0.05 and as showing a trend with P values in the 0.05–0.1 range.
Results
Forty-one intensivists from two tertiary healthcare institutions were invited to participate and 18 (44%) agreed. Their demographic and practice characteristics are listed in Table 2.
Profiles of Functional Outcome Prediction
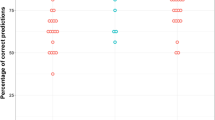
Physicians differed in their assessment of long-term functional outcome for the patient described in the clinical vignette (Fig. 1). First, there was variability in predicting functional outcome along an evaluative dimension. When asked to predict the overall long-term functional outcome for the patient portrayed in the vignette, responses ranged from fair/good to poor. Similar variability was observed among physicians’ predictions of impairments in three specific domains (cognitive, social, and motor skills). For example, while some physicians predicted motor impairments, others thought the patient would likely be free of any (Supplementary Table). Second, there was variability in predicting overall long-term functional outcome along a confidence dimension. The responses of two-thirds of the interviewed physicians indicated considerable uncertainty of their functional outcome predictions, whereas one-third of the physicians’ statements reflected reasonable certainty of their prognosis.

Predicted long-term functional outcome for patient in vignette (see Table 1)
Consequently, profiles of functional outcome prediction, following the evaluative and confidence dimensions described above, could be categorized according to the following prognostic quadrants: (1) physicians who felt fairly confident that the prognosis was fair/good; (2) those who felt that the prognosis was fair/good but were uncertain; (3) those who felt fairly confident that the prognosis was poor; and (4) those who believed the prognosis was poor but were uncertain of this (Fig. 1). Physicians representing each of these four views were identified, but the most prevalent opinion was the fourth quadrant, i.e., expressing concern about a poor prognosis with marked uncertainty (39%; n = 7/18).
Assessment of physician characteristics that may be associated with prognostication profiles showed two trends (Table 3). First, whereas 90% of physicians who had treated ≥20 similar patients in their practice predicted poor outcome, only 50% of physicians who had treated <20 similar patients predicted poor outcome (P = 0.09). Second, physicians who were certain about their prognosis had been in practice for longer (median 11, IQR 7.5–12.75) than those who were uncertain (median 3.5, IQR 1–10.75; P = 0.1) (Table 3). Thus, physicians with more experience tended to be more pessimistic about the patient’s functional outcome and more certain of their prognosis. Differences in functional outcome prediction were not associated with differences in physicians’ age, gender, ethnicity, medical subspecialty, and experience with long-term follow-up in an ambulatory care setting.
Profiles of Quality of Life Prediction
Attitudes toward the quality of life of the patient featured in the clinical vignette varied considerably. Variation was observed along two dimensions: an evaluative dimension (good or poor) and a “style” dimension (objective or subjective) (Figure 1 and Table 4). Eight physicians expressed objective (third person) judgments about quality of life, i.e., quality of life that could be judged “objectively” as poor (n = 7) or fair/good (n = 1). Ten physicians fell into the “subjective” category. These respondents considered quality of life to be too subjective to comment on and, hence, resisted the question to predict the patient’s quality of life. When these physicians were asked to predict quality of life in the questionnaire, despite their feeling that it is a subjective matter, three predicted a poor quality of life, six a fair/good quality of life, and one physician refused to respond.
Physicians who predicted a poor long-term quality of life were older (median 45 years, IQR 39–54 years) than physicians who predicted a fair/good quality of life (median 37 years, IQR 37–41 years; P = 0.04). In addition, trends suggested that physicians who predicted a poor long-term quality of life had spent more years in practice, seen a greater number of similar patients, and were less likely to see patients in long-term follow-up (0.05 < P < 0.1; Table 3). Physicians who felt that quality of life could be predicted objectively tended to be older and tended to have spent more years in practice than their counterparts who felt that quality of life is too subjective to be predicted (P = 0.06 and 0.06, respectively; Table 3).
Self-Reported Factors Influencing Prognostication and EOL Decision-Making
There was little variability among physicians in the ranking of factors that influence their prognosis and EOL decision-making. Physicians considered patient characteristics and preferences most important among the four possibilities (average rank value = 1.2 ± 0.5) and placed professional experience (average rank value = 1.9 ± 0.6) second. The impact of their own personal background (average rank value = 3.3 ± 0.7) and their work environment (average rank value = 3.5 ± 0.5) were ranked as less important. The potential influence of these two factors was often dismissed: “My personal background and experience are irrelevant (…) my religion doesn’t matter, my ethical construct doesn’t matter and I often very importantly highlight that.” Physicians who acknowledged some level of influence of contextual factors (n = 12) frequently spoke about positive features of their environment such as the good resources available to them in an academic center and did not emphasize the potential negative aspects (e.g., possible pressures to use new technologies because of practice in an academic environment).
When physicians were asked to present their wishes regarding continuation of life support if they were in the patient’s situation, seven physicians (39%) indicated that they would have desired withdrawal of life-support for themselves. Three of these seven physicians (43%) would have recommended withdrawal of life-support on the patient if the patient’s preferences were not known. In contrast, none of the 11 physicians (0%) who would have wanted continuation of life-support for themselves supported withdrawal of life-support on the vignette patient (P = 0.043). No significant associations were found between physicians’ personal preferences regarding continuation of life-support if they were in the patient’s situation and their prognostic profile (Table 3).
Discussion
This study coupled quantitative and qualitative research methodologies to capitalize on the unique strengths of both. Although this approach is supported by Giacomini and Cook in 2000 [8, 9] it remains an under-explored research approach in neurology. The qualitative methodology was used to explore, without a priori hypothesis, in which ways physicians differ in terms of prognostication of critically ill neurological patients and to identify discrete prognostication profiles. Subsequently, a quantitative research approach was used to explore which physicians’ demographic or practice characteristics may be associated with these prognostication profiles.
Our qualitative results demonstrate variability in several prognostic domains among physicians. Based on long-term outcome predictions for a patient with severe anoxic brain injury and an uncertain prognosis, functional outcome predictions varied along an evaluative axis (ranging from fairly good to poor functional outcome) and a confidence axis (ranging from certain to uncertain); quality of life predictions varied along an evaluative axis (ranging from poor to “reasonably good” quality of life) and a style axis (ranging from objective opinions to refusal to comment because quality of life was viewed to be the patient’s prerogative). Physicians readily acknowledged that patient characteristics and preferences as well as their professional experience have an influence on their prognostication. However, they did not generally feel that their own personal background or their work environment played a major role in their prognostication and EOL decisions.
The hypothetical clinical circumstances of the patient featured in the vignette were chosen to reflect clinical scenario in which the clinical outcome is uncertain. This uncertainty was built in because the goal was not to determine the accuracy of the physicians’ predictions, but instead to elicit a variety of opinions regarding long-term outcome predictions that could be used to identify domains of prognostic variability and prediction of quality of life among the interviewed physicians. The unique strength of the qualitative research method is that variability was evaluated without being limited to specific a priori hypothesis. The domains of prognostic variability were therefore not pre-specified, but followed from a qualitative assessment of physicians’ responses to open-ended interview questions. As a result variability was identified not only in certain relatively predictable domains (e.g., variability regarding functional outcome along an evaluative axis from fair/good to poor), but also in less predictable domains (e.g., variability regarding quality of life along a style axis ranging from objective to subjective).
Based on our quantitative analyses, older physicians predict a poorer prognosis and quality of life for the vignette-patient. Several other associations between physician characteristics and their prognostic profile showed interesting trends (P values in the range of 0.05–0.1) in this study that was not powered to determine such associations with statistical significance. First, more experienced physicians tended to be more pessimistic about the patient’s functional outcome and more certain of their prognosis. Second, physicians who predicted poor quality of life were older, had spent more years in practice, seen a greater number of similar patients, and were less likely to see patients in long-term follow-up. Third, physicians who felt that quality of life could be predicted objectively tended to be older and to have spent more years in practice. Notably, no significant associations were found between the physicians’ intensive care subspecialty (neurology versus medical) and their prognostic profiles. Also, no significant associations were found between physicians’ preference regarding continuation of life-support on themselves, if they would be in the patient’s situation, and their prognostic profiles. However, physicians who preferred withdrawal of life-support for themselves were significantly more likely to recommend withdrawal of life-support for the patient featured in the vignette than physicians who would have preferred continuation of life-support for themselves.
Given the variability in predicting prognosis and quality of life observed in this study it is foreseeable that a patient’s family can be exposed to physicians that present different prognoses, and express various levels of certainty and diverging approaches to predicting quality of life. This variability, notably variability regarding recommendations for withdrawal of life support and its relationship to physicians’ own preferences, merits attention given that communication with families can impact the EOL decision-making process and experience [10].
Physicians who were interviewed for this study ranked four sets of factors according to their importance in terms of influencing prognosis and EOL decision-making. Patient characteristics and preferences and the physicians own personal experience were ranked highly. This is consistent with the results of our quantitative analyses that suggested several associations between physicians experience and their prognostic profile. Factors such as work environment and personal background were uniformly ranked low and strong influence of these factors was often dismissed. This stands in contrast to the results of previous studies that assessed factors influencing prognostication [11–20]. These studies found that independently of patient characteristics, the personal background of the physician (e.g., age, religious beliefs) and contextual factors such as practice location influence EOL care and decision-making in the intensive care setting. The fact that physicians do not acknowledge or seem unaware of these potential influences raises the concern that physicians entertain an idealized, overly objective view of their own decision-making process that does not fully recognize potential influences and biases.
Our study has important limitations and drawbacks that need to be taken into consideration. The number of participants is limited and the study was not powered to test for differences in characteristics between physicians belonging to various prognostic profiles. Failure to detect such differences is therefore no proof that they indeed do not exist. The study’s sample was also too small to determine the independence of associations in a multi-variable model. In addition, differences and trends that were observed in this study may have been due to chance since we did not adjust the P value for multiple comparisons and this study should therefore be viewed as hypothesis generating. The selection of on institutions located in one geographical location may have introduced selection bias. Future studies are therefore needed to confirm or refute the hypotheses raised by our study. Finally, although as a research method clinical vignettes have the advantage of controlling for the features of a case [21, 22], they limit the amount of information conveyed to respondents.
The results of this study support the need for ongoing research on prognostication for critically ill neurological patients. The domains of prognostic variability that were identified in our study can be used as a starting point for future research in this field. The associations between specific prognostication profiles and physician characteristics that were identified in this study should be examined in studies with larger sample sizes. Future studies are also necessary to determine the accuracy of outcome predictions in patients with severe brain injury as this was not addressed by our study. Finally, trials could be designed to determine if interventions, such as routine discussions regarding prognostication among physicians with different levels of clinical experience and formal feedback to physicians who do not see their patients once they leave the hospital, result in more uniform and accurate prognostication. In the interim, enhanced awareness of the variability that exists among physicians regarding prognostication and prediction of quality of life as well as acknowledgment of the factors that may be responsible for this variability could be first steps toward more consistent and concerted communication of prognosis in patients with critical neurological conditions.
References
Razvi SSM, Bone I. Neurological consultation in the medical intensive care unit. J Neurol Neurosurg Psychiatr. 2003;74(Suppl III):iii16–23. doi:10.1136/jnnp.74.suppl_3.iii16.
Bernat JL. Ethical aspects of determining and communicating prognosis in critical care. Neurocrit Care. 2004;1:107–17. doi:10.1385/NCC:1:1:107.
Kua JKH, Parker G, Lee C, Jorm AF. Beliefs about outcomes for mental disorders: a comparative study of primary health practitioners and psychiatrists in Singapore. Singapore Med J. 2000;41(11):542–7.
Robertson DW. Ethical theory, ethnography, and differences between doctors and nurses in approaches to patient care. J Med Ethics. 1996;22:292–9. doi:10.1136/jme.22.5.292.
Creswell JW. Qualitative inquiry and research design: choosing among five approaches. Thousand Oaks, CA: Sage; 2007.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;9(9):1277–88.
Forman J, Damschroder L. Qualitative content analysis. Adv Bioeth. 2008;11(9):39–63.
Giacomini MK, Cook DJ. Users’ guides to the medical literature: XXIII. Qualitative research in health care B. What are the results and how do they help me care for my patients? Evidence-based medicine working group. JAMA. 2000;284:478–82. doi:10.1001/jama.284.4.478.
Giacomini MK, Cook DJ. Users’ guides to the medical literature: XXIII. Qualitative research in health care A. Are the results of the study valid? Evidence-based medicine working group. JAMA. 2000;284:357–62. doi:10.1001/jama.284.3.357.
Jeffrey D. Patient-centred ethics and communication at the end of life. Oxford: Radcliffe Publishing; 2005.
Keenan SP, Busche KD, Chen LM, Esmail R, Inman KJ, Sibbald WJ. Withdrawal and withholding of life support in the intensive care unit: a comparison of teaching and community hospitals. The Southwestern Ontario Critical Care Research Network. Crit Care Med. 1998;26:245–51. doi:10.1097/00003246-199802000-00018.
Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158:1163–7.
Cook DJ, Guyatt GH, Jaeschke R, et al. Determinants in Canadian health care workers of the decision to withdraw life support from the critically ill. Canadian Critical Care Trials Group. JAMA. 1995;273:703–8. doi:10.1001/jama.273.9.703.
Asch DA, Faber-Langendoen K, Shea JA, Christakis NA. The sequence of withdrawing life-sustaining treatment from patients. Am J Med. 1999;107:153–6. doi:10.1016/S0002-9343(99)00198-9.
Cook DJ, Giacomini M, Johnson N, Willms D. Life support in the intensive care unit: a qualitative investigation of technological purposes. Canadian Critical Care Trials Group. CMAJ. 1999;161:1109–13.
Marcin JP, Pollack MM, Patel KM, Sprague BM, Ruttimann UE. Prognostication and certainty in the pediatric intensive care unit. Pediatrics. 1999;104:868–73. doi:10.1542/peds.104.4.868.
Marcin JP, Pretzlaff RK, Pollack MM, Patel KM, Ruttimann UE. Certainty and mortality prediction in critically ill children. J Med Ethics. 2004;30:304–7. doi:10.1136/jme.2002.001537.
Rocker GM, Cook DJ, Shemie SD. Practice variation in end of life care in the ICU: implications for patients with severe brain injury. Can J Anaesth. 2006;53:814–9.
Rebagliato M, Cuttini M, Broggin L, et al. Neonatal end-of-life decision making: physicians’ attitudes and relationship with self-reported practices in 10 European countries. JAMA. 2000;284:2451–9. doi:10.1001/jama.284.19.2451.
Randolph AG, Zollo MB, Wigton RS, Yeh TS. Factors explaining variability among caregivers in the intent to restrict life-support interventions in a pediatric intensive care unit. Crit Care Med. 1997;25:435–9. doi:10.1097/00003246-199703000-00011.
Veloski J, Tai S, Evans AS, Nash DB. Clinical vignette-based surveys: a tool for assessing physician practice variation. Am J Med Qual. 2005;20:151–7. doi:10.1177/1062860605274520.
Peabody JW, Luck J, Glassman P, Dresselhaus TR, Lee M. Comparison of vignettes, standardized patients, and chart abstraction: a prospective validation study of three methods for measuring quality. JAMA. 2000;283:1715–22. doi:10.1001/jama.283.13.1715.
Acknowledgments
The authors would like to acknowledge the contribution of all volunteer participants for their time and openness as well as Tessa Watt for research assistance. Support for this research comes from the Social Sciences and Humanities Research Council of Canada (E.R.) the Institut de recherches cliniques de Montréal (E.R.), the Fonds de la recherche en santé du Québec (E.R.), the Canadian Institutes of Health Research (E.R.), and the National Institutes of Health/National Institute of Neurological Disorders and Stroke, (R01 #NS045831, J.I. and K23 NS051372, M.L.).
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Racine, E., Dion, MJ., Wijman, C.A.C. et al. Profiles of Neurological Outcome Prediction Among Intensivists. Neurocrit Care 11, 345–352 (2009). https://doi.org/10.1007/s12028-009-9225-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-009-9225-9