
Abstract
Some previously reported cases of brain evisceration in catastrophic craniocerebral injuries showed the presence of brain swelling. The aim of this study was to observe the occurrence of focal or diffuse brain swelling in such cases in order to explain the underlying mechanism. An observational autopsy study included 23 adults, 18 males and 5 females, whose average age was 48 ± 22 years (range: 19–89 years) and who died as the result of catastrophic craniocerebral injury with brain evisceration. In all the examined cases, either focal (12 cases) or diffuse (11 cases) brain swelling was present. Grossly visible brain contusions (either cortical or deep) were rarely present – only in 6 out of 23 cases, while microscopic brain contusions were observed in 22 out of 23 cases, with 1 remaining case of microscopic subarachnoid bleeding. Blood aspiration in the lungs, as a vital reaction, was noted in 20 out of 23 cases. Microscopic examination showed absence of edema in 20 cases and mild edema in only 3 cases, while microscopic signs of moderate or severe edema were absent. Brain swelling in cases of brain evisceration likely represents a biomechanical reaction (i.e. decompression) due to a sudden decrease in intracranial pressure. The rapidity of death, together with marked absence of microscopic signs of edema, suggests that this is not a form of biological response to injury, but rather a pure physical phenomenon, strictly in a living person. In such cases, the occurrence of brain swelling and parenchymal microbleeding should be considered vital reactions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
All pathologists who perform autopsies frequently observe the flattening of the gyri and narrowing of the sulci in their everyday work. These are caused by brain swelling which is not uncommon, either as a contributor to the cause of death or just as a phenomenon coexisting with a remote cause of death (e.g. metabolic disturbances). Diffuse brain swelling denotes a generalized increase in the volume of the brain, usually resulting from vasodilatation or edema. Vasodilatation, which may occur following a severe head injury, is a failure of the normal vasomotor control system followed by increased cerebral blood volume that results in brain swelling. Cerebral edema is defined as an abnormal accumulation of fluid in the cerebral parenchyma that produces an increase in cerebral volume. It may be vasogenic (due to blood–brain barrier dysfunction), cytotoxic (due to cellular injury involving endothelial cells, glia and neurons) or interstitial (due to abnormal flow of cerebrospinal fluid), but the combination of these mechanisms is the most common [1,2,3]. Expanding processes, such as subdural hematomas, cerebral tumors, abscesses and hematomas, may result in focal brain swelling [2].
However, some previously reported cases showed the presence of the flattening of the gyri and narrowing of the sulci, hence, the presence of brain swelling, in cases where there was obviously not enough time for either vasodilatation or development of edema, because death occurred virtually instantaneously due to brain evisceration following catastrophic craniocerebral injuries [4,5,6]. Radiological studies and animal models suggested that the development of brain swelling required a relatively small amount of time, but one measured in tens of minutes following a brain trauma [7,8,9]. However, although in forensic cases with the open cranium and brain evisceration this amount of time was measured in seconds, the signs of either focal or diffuse brain swelling were grossly visible and the reasons for this remained unclear.
The aim of this study was to observe the occurrence of focal or diffuse brain swelling in cases of brain evisceration resulting from a catastrophic craniocerebral injury in order to explain the underlying mechanism and significance of brain swelling.
Material and methods
An observational autopsy study was conducted over a three-year period. The study comprised cases of adults who died as the result of a catastrophic craniocerebral injury with brain evisceration. All the deceased died at the scene. Autopsy reports, police records and heteroanamnestic data for each deceased person were analyzed and evaluated with regard to sex, age and circumstances and manner of death. During autopsy, the present parts of the brain were examined and analyzed for the presence of focal or diffuse brain swelling. Due to severity of the injury, in some cases only parts of the brain were available for examination. That is why the brain weight was not measured. We also examined the presence of macroscopically visible brain swelling, i.e. flattening of the gyri and narrowing of the sulci. If brain swelling was present only in some parts of the examined brain tissue, we considered that to be focal brain swelling. However, if brain swelling was present in all the examined parts of the brain (regardless of the fact that sometimes only part of the brain was present), we considered it to be diffuse brain swelling. Brain tissue was also examined for the presence of macroscopically visible brain contusions. Furthermore, we examined the lungs for the presence of blood due to aspiration as one of the fastest vital reactions.
Tissue samples were taken from the swollen parts and then fixed with 10% formaldehyde, embedded in paraffin, and treated with routine hematoxylin-eosin staining. The slides were further microscopically analyzed according to generally accepted morphologic criteria for cerebral edema (pallor of the myelin, distention of perivascular and pericellular spaces, loose or sieve-like appearance of myelinated areas, rarefaction of subpial spaces, vacuolar appearance of the gray matter neuropil). Using a combination of these signs, the proposed grading was the following: no edema – 0; mild edema – 1+; moderate edema – 2+; severe edema – 3+ [10, 11]. The slides were also microscopically analyzed for the presence of tissue injury (bleeding).
The obtained data were statistically analyzed using Pearson’s chi-square test in order to estimate the differences. A p value less than 0.05 was considered significant, and less than 0.01 highly significant.
Results
The sample consisted of 23 subjects, 18 males and 5 females (χ2 = 7.348, df = 1, p = 0.007), whose average age was 48 ± 22 years (range: 19–89 years). There were 12 cases of accidents (6 car occupants, 5 pedestrians and 1 case of a work accident) and 11 cases of suicide (7 cases of jumping from great heights, 1 case of jumping in front of a train and 3 cases of gunshot head injuries with a rifle in the form of a Krönlein’s shot [12]).
In 18 out of 23 cases, parts of the brain were missing due to severity of the injury; therefore, only parts of the brain were available for examination. The entire brain was available for autopsy in 5 cases. In all the examined cases, some degree of grossly visible brain swelling in the form of flattened gyri and narrowed sulci was observed: either focal (12 cases) – engaging only part of each examined brain tissue or diffuse (11 cases) – engaging (almost) complete brain (or part of the brain available for examination) (Fig. 1), with no significant differences between the two (χ2 = 0.04, df = 1, p > 0.05). Grossly visible brain contusions (either cortical or deep) were rarely present – only in 6 out of 23 cases (χ2 = 5.261, df = 1, p = 0.022). As a vital reaction, blood aspiration was noted in the lungs in 20 out of 23 cases (χ2 = 11,152, df = 1, p < 0.001).

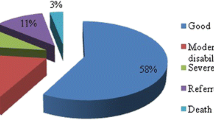
A 24-year-old male fatally injured in a traffic accident as a car driver. Macroscopic appearance of a the head injury and b focal brain swelling. c Microscopic appearance of the brain with microbleeding and no microscopic signs of edema
Microscopic examination showed absence of edema in 20 cases (Fig. 1c) and mild edema in only 3 cases (Fig. 2a), while microscopic signs of moderate or severe edema were not present in the examined samples (χ2 = 45.167, df = 3, p < 0.001).

a One of the three cases with a mild microscopic edema (a 24-year-old female, a car occupant who died in a traffic accident) with pale, loose or sieve-like appearance of myelinated areas. b Microbleeding in brain tissue as a marker of vitality. c Microscopically visible bleeding in subarachnoid space, also as a marker of vitality
In all six cases in which brain contusion was macroscopically observed, microscopic examination also showed the presence of parenchymal brain injury. However, in an additional 16 cases (in which no brain contusions were observed macroscopically) there were microscopic signs of injury in the form of parenchymal microbleeding (Fig. 2b), accounting for the total of 22 cases with (macroscopic and/or microscopic) signs of brain injury. In the one remaining case we could not identify any brain contusions (regardless of severe tissue destruction present), but there were signs of microscopic subarachnoid bleeding (Fig. 2c).
Discussion
Brain swelling and cerebral edema are common reactions of the brain to injuries of different etiology. Simple swelling of the brain is a relatively common finding in deaths encountered in medicolegal practice, especially in relatively quick (asphyxial) deaths. The pathophysiology of this condition is not clear, but, in simple terms, it includes an increase in the volume of the brain, usually related to an increase in the amount of intravascular blood. Histological examination may show congestion of intracerebral vessels with perivascular hemorrhages. Some authors differentiate between this condition and true cerebral edema or congestive brain swelling with raised intracranial pressure [13]. Congestive brain swelling can occur as a result of an increase in the amount of intravascular blood, predominantly in the capillary and post-capillary bed, causing an increase in brain volume. If congestive brain swelling is prolonged, vasogenic cerebral edema supervenes with water accumulation in the extracellular spaces [13].
Both brain swelling and brain edema represent forms of secondary brain injury (together with hypoxic-ischemic brain injury and secondary parenchymal bleeding), unlike the primary lesions, such as brain contusions, parenchymal lacerations, diffuse axonal injury, etc. [14]. Therefore, they do not occur immediately, but require a certain amount of time. In injuries with brain evisceration resulting from a catastrophic craniocerebral injury, there is not enough time for the development of any of the classical reactions to injury, listed in classical textbooks as “typical” secondary reactions to injury, either of neurons or of glial cells: acute neuronal injury (“red neurons”), subacute and chronic neuronal injury (“degeneration”), axonal reaction, presence of inclusions, gliosis, etc. [1,2,3, 13, 14]. The speed of brain swelling following a blunt craniocerebral trauma has been the subject of debate amongst forensic pathologists. Some suggest that the swelling may be a rapid process, while others think that it may on occasion occur much more slowly [4]. However, the term “rapid” used in this sense does not mean that this process takes seconds, but at least tens of minutes. Some case reports describe a “quite rapid” development of brain swelling in children, as early as 1 h and 17 min following trauma [15]. In experimental animal models the period is even shorter, showing a significant rise in intracranial pressure in the first 10 min after traumatic injury, followed by a slow decrease in the following 60 min [8].
However, in cases of brain evisceration, brain swelling cannot be explained by these mechanisms. In the presented study, as in the previously reported cases [4,5,6], death was practically instantaneous, and in all the cases either focal or diffuse brain swelling occurred immediately. Based on their presented case reports, Byard et al. [4], as well as Kachan et al. [5], suggested reactive vasodilatation as the probable mechanism, given that it was unlikely that there would have been enough time for the development of significant interstitial edema in the seconds between the impact, injury and death. To our knowledge, the present study is the first one to include a series of cases with brain evisceration due to catastrophic craniocerebral injury and explore the (macroscopic and microscopic) presence and mechanism of instantaneous brain swelling. As we suggested in one of our previous case reports [6], we believe that a mechanism either different from or additional to reactive vasodilatation is responsible for this phenomenon.
The usual intracranial pressure (ICP) in adults is 5 to 15 mmHg (60 to 180 cm H2O), and its normal upper limit is about 20 mmHg (2.7 kPa) [3, 14, 16]. This means that the intracranial pressure is positive, i.e. (slightly) higher than the atmospheric pressure. In a severe blunt head injury, the cranium opens at the moment of injury and sudden decompression occurs. This leads to instantaneous leveling of the intracranial and atmospheric pressures, literally causing physical tissue expansion and, therefore, brain tissue swelling, observed by the naked eye as the flattening of the gyri and narrowing of the sulci. The difference between the intracranial and atmospheric pressures could additionally be increased by an enormous amount of kinetic energy being transferred to the head in cases of severe or catastrophic head injuries, causing brain evisceration and abruptly and quickly increasing the difference between pressures, i.e. abruptly increasing the intracranial pressure. We are not sure whether the injury lasted long enough for reactive vasodilatation, because it was measured in just a couple of seconds, at the most, but this study can neither exclude nor confirm this mechanism. If reactive vasodilatation was part of the brain swelling mechanism in such cases, that would (at least) slightly increase the weight of the brain. However, even if we could have measured the brain, we would not be able to prove the brain weight increase, which is why the question of involvement of reactive vasodilatation in the mechanism of brain swelling in cases of brain evisceration remains open.
The mechanism of momentary decompression of brain tissue is supported by histological examination of the injured tissue. Histological parameters of brain swelling/edema are often considered imprecise with significant inter-observer or intra-observer differences, and some of the signs mentioned in older textbooks are nowadays commonly considered to be fixation and preparation artefacts, e.g. perivascular clearing or neuronal contraction, with widening of perineuronal and perivascular spaces [13, 17]. However, even these (imprecise) criteria were markedly absent in our sample, with the absence of microscopic signs of edema in 20 cases and the presence of signs of mild edema in only 3 cases, which might have been caused by something else rather than the brain injury. The most prominent finding in these 3 cases was slightly loose or sieve-like appearance of myelinated areas, i.e. white matter. In the examined samples, perivascular clearing, listed as one of the possible fixation artifacts [13, 17], was present to a very small degree in a small portion of blood vessels, indicating that it is probably more pronounced in a real brain edema; however, this finding should be interpreted very carefully taking into consideration all other findings. All of the aforementioned findings suggest that grossly visible brain swelling is a biomechanical rather than a biological phenomenon.
The absence of grossly visible brain contusions (17 out of 23 cases) speaks in favor of the rapidity of death. On the other hand, the presence of microscopic brain injury (parenchymal injury in 22 cases and subarachnoid bleeding in the one remaining case) speaks not so much of the severity of injury or rapidity of death as of vitality of brain injury. Additionally, blood aspiration, as another vital reaction, was slightly less present compared to microscopic brain contusions, but also occurred in a vast majority of cases (20 out of 23). Brain swelling in cases of brain evisceration due to catastrophic craniocerebral injury also seems to be a vital reaction. One would not expect pathologists to see focal or diffuse brain swelling as a consequence of the opening of the skull during autopsy. After death, all the pressures inside the human body, including the one inside the cranial cavity, are equalized with the pressure of external environment, i.e. intracranial pressure is no longer higher than the atmospheric pressure, but becomes equal to it. Although we do not know the exact moment after death when this happens, it probably occurs very shortly after death. Therefore, no decompression and rapid swelling occur during autopsy.
Brain swelling is not commonly observed in neurosurgical procedures immediately after craniotomy, which makes the mechanism of decompression questionable. One of the possible reasons for absence of decompressive brain swelling in neurosurgical operations is the slow, gradual change of pressure during craniotomy, as opposed to the sudden and abrupt change of pressure in cases of brain evisceration, especially taking into consideration the fact that the normal, physiological intracranial pressure is relatively low. At the beginning of the surgery, all of the conditions are strictly controlled by physicians who use appropriate therapy and place the patient’s head in appropriate position. However, we found several papers describing brain swelling shortly after craniotomy which might (at least partially) be attributed to decompression during craniotomy [18, 19]. Nevertheless, if blunt force acts on a living person, further pressuring the head and additionally increasing intracranial pressure, at the moment when the skull breaks the level of decompression might be even higher and brain swelling more obvious and possibly diffuse, rather than focal.
The current study suggests that focal or diffuse brain swelling in cases of brain evisceration due to catastrophic craniocerebral trauma likely represents a biomechanical reaction (i.e. decompression) as the result of a sudden decrease in intracranial pressure. The rapidity of death, together with marked absence of microscopic signs of edema, suggests that this is not a form of biological response to injury, but rather a pure physical phenomenon, strictly in a living person. In such cases, the occurrence of brain swelling and parenchymal microbleeding should be considered vital reactions, meaning that the victim was alive when craniocerebral injury was inflicted, especially in cases with concurrent causes of death due to multiple region injuries.
Key points
-
1.
Focal or diffuse brain swelling is common in cases of brain evisceration due to catastrophic craniocerebral injury.
-
2.
Brain swelling in cases of brain evisceration likely represents a biomechanical reaction (i.e. decompression) due to a sudden decrease in intracranial pressure, with or without reactive vasodilatation.
-
3.
Macroscopic brain swelling in cases of brain evisceration is not accompanied by microscopic signs of brain edema.
-
4.
Macroscopic brain swelling in cases of brain evisceration may be considered a vital reaction, together with other signs of vitality, such as brain parenchymal microbleeding and blood aspiration.
References
Kumar V, Abbas AK, Aster JC, editors. Robbins and Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier; 2014.
Cross SS, editor. Underwood’s pathology - a clinical approach. 6th ed. London: Churchill – Livingstone Elsevier; 2013. https://doi.org/10.1117/12.2006447.
Herrington CS, editor. Muir’s textbook of pathology. 15th ed. Boca Raton: CRC Press – Taylor & Francis Group; 2014.
Byard RW, Vink R. Speed of development of cerebral swelling following blunt cranial trauma. J Forensic Legal Med. 2013;20:598–600. https://doi.org/10.1016/j.jflm.2012.12.004.
Kanchan T, Geriani D, Savithry KSB. Is cerebral swelling following cranio-cerebral trauma instantaneous? An insight into the Byard and Vink proposition. Forensic Sci Med Pathol. 2014;11:117–8.
Nikolić S, Živković V. Regarding instantaneous cerebral swelling following severe cranio-cerebral trauma with brain evisceration. Forensic Sci Med Pathol. 2015;11:321–2. https://doi.org/10.1007/s12024-015-9657-9.
Byard RW, Bhatia KD, Reilly PL, Vink R. How rapidly does cerebral swelling follow trauma? Observations using an animal model and possible implications in infancy. Leg Med (Tokyo). 2009;11(Suppl. 1):S128–31.
Byard RW, Gabriellian L, Helps SC, Thornton E, Vink R. Further investigations into the speed of cerebral swelling following blunt cranial trauma. J Forensic Sci. 2012;57:973–5. https://doi.org/10.1111/j.1556-4029.2012.02109.x.
Barzo P, Marmarou A, Fatouros P, Hayasaki K, Corwin F. Contribution of vasogenic and cellular edema to traumatic brain swelling measured by diffusion-weighted imaging. J Neurosurg. 1997;87:900–7. https://doi.org/10.3171/jns.1997.87.6.0900.
Yates AJ, Thelmo W, Pappius HM. Postmortem changes in the chemistry and histology of normal and edematous brains. Am J Pathol. 1975;79:555–64.
Poirier J, Gray F, De Girolami U. Escourolle and Poirier manual of basic neuropathology. 4th ed. Philadelphia: Elsevier; 2004.
Nikolić S, Živković V. Suicidal Krönlein shot with a home manufactured firearm. Forensic Sci Med Pathol. 2015;11:297–9. https://doi.org/10.1007/s12024-015-9666-8.
Whitwell H. Forensic neuropathology. London: Hodder Arnold; 2005.
Oehmichen M, Auer RN, Koenig GK. Forensic neuropathology and associated neurology. Berlin: Springer; 2009. https://doi.org/10.1016/j.forsciint.2009.05.020.
Willman KY, Bank DE, Senac M, Chadwick DL. Restricting the time of injury in fatal inflicted head injuries. Child Abuse Negl. 1997;21:929–40. https://doi.org/10.1016/S0145-2134(97)00054-9.
McCance KL, Huether SE. Pathophysiology: the biologic basis for disease in adults and children. 8th ed. St. Louis: Elsevier; 2019. https://doi.org/10.1016/j.ecl.2019.05.008.
Mills SE, editor. Histology for pathologists. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. https://doi.org/10.1086/BBLv222n2pviii.
Whittle IR, Viswanathan R. Acute intraoperative brain herniation during elective neurosurgery: pathophysiology and management considerations. J Neurol Neurosurg Psychiatry. 1996;61:584–90. https://doi.org/10.1136/jnnp.61.6.584.
Nho JS, Choi SE, Yi JW, Kang JM. Intraoperative acute brain swelling when performing indirect anastomosis in a patient with moyamoya disease - a case report. Korean J Anesthesiol. 2010;59(Suppl):S191–3. https://doi.org/10.4097/kjae.2010.59.S.S191.
Funding
This work was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia, Grant No. 45005.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors hereby declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Živković, V., Cvetković, D., Obradović, D. et al. Mechanism of brain swelling in cases of brain evisceration due to catastrophic craniocerebral injury – an autopsy study. Forensic Sci Med Pathol 16, 107–112 (2020). https://doi.org/10.1007/s12024-019-00207-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-019-00207-1