
Abstract
Carcinomas arising from embryonic adrenal rests are rare with only a handful of reported cases. We report a case of an adrenocortical carcinoma arising from an adrenal rest located between the bladder and prostate in a 51 year-old man. The patient presented following a year of rectal pain and constipation. Computed tomography (CT) scan revealed a 9 cm pelvic mass that appeared to arise from the soft tissue between the bladder and prostate, with displacement of the organs and narrowing of the rectal lumen, suspected to be a sarcoma. The surgically resected specimen showed a well-circumscribed, partially encapsulated tumor measuring 10.0 cm in greatest dimension. Both adrenal glands were identified intraoperatively. Grossly, the lesion was heterogeneous tan-brown to yellow, hemorrhagic and necrotic. Histology revealed sheets and nests of high-grade pleomorphic tumor cells with abundant clear to vacuolated cytoplasm with areas of necrosis, a high mitotic index (>10 mitoses/10 HPF) and foci suspicious for lymphovascular invasion. Adjacent adrenal cortical-type tissue was identified. Immunohistochemical stains revealed the tumor cells were weakly and focally positive for MiTF, Melan-A, inhibin and synaptophysin, and negative for CKAE1/AE3, HMB-45, calretinin, EMA, SMA, chromogranin, PAX8, MDM2 and CDK4. Based upon the morphologic and immunohistochemical profile, this was diagnosed as an adrenocortical carcinoma, arising in an adrenal rest. To our knowledge, no such tumor has been previously described in this location.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Morgagni in 1740 first described yellowish nodules resembling adrenal tissue adjacent to the gland [1–3]. Over a hundred years later in 1856, Piccolominus was the first to report accessory adrenal tissue [2, 4]. Adrenal rests, also known as ectopic or accessory adrenal tissue are fragments that break-off during embryological development. The adrenal cortex arises from the coelomic mesoderm of the urogenital ridge and the medulla arises from neural crest tissue which invaginates into the cortical tissue during embryology [3, 5, 6]. Depending upon when the break occurs, determines what type of tissue will remain, such that closer to the gland proper will result in cortex with or without medulla and more distant to the gland will result in cortex only [3, 7].
Adrenal rests can occur anywhere along the embryological path of migration usually related to gonadal descent, such as in the retroperitoneum, kidneys, broad ligament, ovaries, spermatic cord, epididymis and testis. [2, 7] However, they have also been described elsewhere such as in intracranial and spinal locations and within the gastrointestinal system. [8–10] Adrenal rests are much more common in neonates and children (50%), and rarely persist into adulthood (1%) as functioning tissue or a neoplasm as it generally undergoes atrophy within a few years. [3, 6, 7, 11] However, it is exceptional for a malignancy to arise from an adrenal rest, with only a few cases reported. We present a case of an adrenocortical carcinoma arising from an adrenal rest located between the prostate and bladder with a review of the English literature.
Case Report
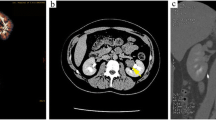
A 51 year-old male with no significant medical history presented with rectal pain and constipation for 12 months duration. A computed tomography (CT) scan revealed a 9.0 cm pelvic mass that appeared to arise within the soft tissue between the prostate and bladder, causing organ displacement and narrowing of the rectal lumen. Based upon the radiologic features, it was suspected to be a sarcoma. A resection of the neoplasm was performed requiring dissection off both the bladder and prostate with a partial colectomy, due to adherence to the rectosigmoid colon. Both of the adrenal glands were identified intraoperatively and were grossly unremarkable.
The specimen showed a well-circumscribed, partially encapsulated tumor measuring 10.0 cm in greatest dimension. Grossly, the lesion was heterogeneous, tan-brown to yellow, hemorrhagic and necrotic. Histologic examination revealed sheets and nests of high-grade, pleomorphic cells with abundant eosinophilic to clear and vacuolated cytoplasm, with areas of necrosis and a high mitotic index (>10 mitoses/10 high-power field) (Fig. 1). Foci suspicious for lymphovascular invasion were also identified. Adjacent adrenal cortical-type tissue was also present, often in a lobular architecture. Immunohistochemical stains revealed the tumor cells were focally positive for MiTF, Melan-A, inhibin and synaptophysin. The tumor cells were negative for CKAE1/AE3, HMB-45, calretinin, EMA, SMA, chromogranin, PAX8, MDM2 and CDK4. Based upon the morphologic and immunohistochemical profile, this was diagnosed as an adrenocortical carcinoma (ACC), arising in an adrenal rest. The post-operative course was unremarkable, and he received adjuvant radiation and chemotherapy with mitotane. He had no evidence of disease at 9 months follow-up.

AACC arising in an adrenal rest. a Low-power view of the lobulated architecture (H&E stain, ×20). b Background adrenal cortical-type tissue (H&E stain, ×20). c–d Sheets of high-grade, pleomorphic tumor cells with abundant eosinophilic and clear to vacuolated cytoplasm (H&E stain, ×100 and ×200). Tumor cells were focally positive for e Melan-A and f inhibin immunostains (×100)
Discussion
Tumors arising from adrenal rests are uncommon and most are functional, resulting in an endocrinopathy, and are often diagnosed pre-operatively [11]. Infrequently are they non-functional, usually discovered incidentally or at time of autopsy [11]. Malignancies arising from adrenal rests are extremely rare with only a handful of cases reported and their clinicopathologic features are summarized in Table 1 [9, 11–21]. Malignant tumors arising from adrenal rests have been described in 13 patients, including our current case at a mean age of 36.4 years (0.4–65 years) with an equal female to male ratio (7:6). The tumors were located in the retroperitoneum (n=5), testis/scrotum (n=3), liver (n=2), kidney (n=1), spinal cord (n=1) and pelvis (n=1). Eight (62%) tumors were functioning, with patients most commonly presenting with Cushing’s syndrome.
Histologically, the differential diagnosis of ACC is broad and includes metastatic renal cell carcinoma (RCC), hepatoid variant of yolk sac tumor (YST), melanoma, malignant leydig cell tumor and liposarcoma [20]. Rarely, extra-adrenal neoplasms such as hepatic and Leydig cell tumors have been reported to produce ectopic cortisol, adrenocorticotropic (ACTH) and cortisol-releasing factor (CRF) [9, 22]. The pattern of immunohistochemical findings such as positive inhibin, Melan-A, MiTF and synaptophysin markers, suggest an adrenal cortex origin of the tumor cells and are expressed in ACC and help to exclude other malignancies in the differential diagnosis [20, 22].
Based upon our review of the literature, 11 of 13 cases (85%) underwent surgical resection with one case treated with chemotherapy alone (8%) and 5 (38%) cases treated with adjuvant chemotherapy and/or radiotherapy. Surgical resection is the mainstay of treatment with potential for cure in ACC [20, 23]. The 5 and 10-year survival in patients who underwent resection for ACC was 26–38% and 7%, respectively [23–25]. The patients with early mortality, were found to have higher rates of cortisol-secreting tumors, positive resection margins and higher stage with nodal or synchronous distant metastasis [23–25]. The importance of surgery was further confirmed by long-term survival attained with repeat resection of local or distant tumor recurrence [23].
In our review, 6 (50%) patients were diagnosed with tumor recurrence and/or metastases, of which 5 died of disease at a mean of 6.3 months (6 days-16 months) [9, 13–16, 22]. Five patients were without evidence of disease at a mean follow-up period of 26.4 months (2.25–120 months). All 5 patients underwent surgical resection for a primary tumor without evidence of nodal or distant metastasis, of which 2 were treated with adjuvant chemotherapy and/or radiotherapy [11, 12, 17, 19, 20].
The role of adjuvant chemotherapy and radiation is limited and unclear. Mitotane is the most common chemotherapeutic agent used to treat ACC with limited response [20, 26]. Tumors which do show response may obtain prolonged survival, with significant benefit found in patients not cured surgically or with an increased risk of recurrence [20, 25, 26]. Moreover, additional studies have found a significantly longer recurrence-free survival in patients treated with adjuvant mitotane therapy after radical surgery [26].
Adjuvant radiotherapy remains controversial with studies showing conflicting results, some revealing an advantage with significant reduction of local recurrence, while others showing no added benefit [27–29]. Functioning carcinomas with production of steroids may also benefit from treatment with agents such as ketoconazole by blocking adrenal steroid synthesis, such as the case reported by Contreras and colleagues [17].
The prognosis of patients with ACC is poor, with recurrence and metastasis being common [20, 26]. The management of patient’s with more advanced disease in which surgical resection is not optional or curative may benefit from a combination of loco-regional resection, chemoembolization, radiofrequency (RFA) and/or systemic chemotherapy [26]. The combination of cytotoxic chemotherapy plus mitotane may also be beneficial in a subset of patients with advanced or metastatic disease with reduced progression-free survival [26].
Conclusion
In summary, we report the unique occurrence of an adrenocortical carcinoma arising from an adrenal rest within the pelvis, located between the prostate and bladder. Frank features of histologic malignancy were present. Although the occurrence of malignancies arising from adrenal rests is rare, pathologists should be aware that they can occur, particularly within any location along the path of embryologic migration of the genitourinary tract.
References
Morgagni, G.B.: Cited by Wiesel, quod vidae.
Abell I. Primary Hypernephroma of the Liver. Ann Surg. 1928;87:829–836.
Schechter DC. Aberrant adrenal tissue. Ann Surg. 1968;167:421–426.
Pepere, A.: Tumeur primitive du foie originaire des germes aberrants de la capsule serrenale. Arch. De med. Exper. Et d’anat. Path., Par., 1902, vol. xiv, pp.765–808.
Keene MF. Observations on the Development of the Human Suprarenal Gland. J Anat. 1927;61:302–324.
Anderson JR, Ross AH. Ectopic adrenal tissue in adults. Postgrad Med J. 1980;56:806–808.
Barwick TD, Malhotra A, Webb JA, et al. Embryology of the adrenal glands and its relevance to diagnostic imaging. Clin Radiol. 2005;60:953–959.
Wiener MF, Dallgaard SA. Intracranial adrenal gland; a case report. AMA archives of pathology. 1959;67:228–233.
Wallace EZ, Leonidas JR, Stanek AE, et al. Endocrine studies in a patient with functioning adrenal rest tumor of the liver. The American journal of medicine. 1981;70:1122–1125.
Cassarino DS, Santi M, Arruda A, et al. Spinal adrenal cortical adenoma with oncocytic features: report of the first intramedullary case and review of the literature. International journal of surgical pathology. 2004;12:259–264.
Goren E, Engelberg IS, Eidelman A. Adrenal rest carcinoma in hilum of kidney. Urology. 1991;38:187–190.
Yokoyama H, Adachi T, Tsubouchi K, et al. Non-functioning adrenocortical carcinoma arising in an adrenal rest: immunohistochemical study of an adult patient. Tohoku J Exp Med. 2013;229:267–270.
Akishima-Fukasawa Y, Yoshihara A, Ishikawa Y, et al. Malignant adrenal rest tumor of the retroperitoneum producing adrenocortical steroids. Endocr Pathol. 2011;22:112–117.
Rodriguez FJ, Scheithauer BW, Erickson LA, et al. Ectopic low-grade adrenocortical carcinoma in the spinal region: immunohistochemical and molecular cytogenetic study of a pediatric case. The American journal of surgical pathology. 2009;33:142–148.
Engel FL, McPherson HT, Fetter BF, et al. Clinical, Morphological and Biochemical Studies on a Malignant Testicular Tumor. The Journal of clinical endocrinology and metabolism. 1964;24:528–542.
Morimoto Y, Hiwada K, Nanahoshi M, et al. Cushing's syndrome caused by malignant tumor in the scrotum: clinical, pathologic and biochemical studies. The Journal of clinical endocrinology and metabolism. 1971;32:201–210.
Contreras P, Altieri E, Liberman C, et al. Adrenal rest tumor of the liver causing Cushing's syndrome: treatment with ketoconazole preceding an apparent surgical cure. The Journal of clinical endocrinology and metabolism. 1985;60:21–28.
Ney RL, Hammond W, Wright L, et al. Studies in a patient with an ectopic adrenocortical tumor. The Journal of clinical endocrinology and metabolism. 1966;26:299–304.
Raith L, Karl HJ. Pregnancy in ectopic adrenal carcinoma. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme. 1969;1:149–150.
Bani-Hani KE. Primary non-functional extra-adrenal adrenocortical carcinoma. Saudi Med J. 2003;24:301–304.
Transactions of the Philadelphia Academy of Surgery-Stated Meeting March 7, 1932. Annals of surgery. 1933;97:146–155.
Jain SH, Sadow PM, Nose V, et al. A patient with ectopic cortisol production derived from malignant testicular masses. Nat Clin Pract Endocrinol Metab. 2008;4:695–700.
Tran TB, Postlewait LM, Maithel SK, et al. Actual 10-year survivors following resection of adrenocortical carcinoma. Journal of surgical oncology. 2016.
Tritos NA, Cushing GW, Heatley G, et al. Clinical features and prognostic factors associated with adrenocortical carcinoma: Lahey Clinic Medical Center experience. The American surgeon. 2000;66:73–79.
Icard P, Goudet P, Charpenay C, et al. Adrenocortical carcinomas: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons study group. World journal of surgery. 2001;25:891–897.
Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma. The New England journal of medicine. 2007;356:2372–2380.
Habra MA, Ejaz S, Feng L, et al. A retrospective cohort analysis of the efficacy of adjuvant radiotherapy after primary surgical resection in patients with adrenocortical carcinoma. The Journal of clinical endocrinology and metabolism. 2013;98:192–197.
Fassnacht M, Hahner S, Polat B, et al. Efficacy of adjuvant radiotherapy of the tumor bed on local recurrence of adrenocortical carcinoma. The Journal of clinical endocrinology and metabolism. 2006;91:4501–4504.
Sabolch A, Feng M, Griffith K, et al. Adjuvant and definitive radiotherapy for adrenocortical carcinoma. International journal of radiation oncology, biology, physics. 2011;80:1477–1484.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
None.
Rights and permissions
About this article

Cite this article
Cornejo, K.M., Afari, H.A. & Sadow, P.M. Adrenocortical Carcinoma Arising in an Adrenal Rest: a Case Report and Review of the Literature. Endocr Pathol 28, 165–170 (2017). https://doi.org/10.1007/s12022-017-9472-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12022-017-9472-9