
Abstract
Amyloid is a characteristic histologic feature in medullary thyroid carcinomas (MTC). We utilized a novel mass spectrometry-based proteomic analysis to determine if we could identify specific proteins associated with amyloid in MTC. We studied 9 MTC (1 multiple endocrine neoplasia type 2A, 1 familial MTC, and 7 sporadic). Laser microdissection was utilized to sample the amyloid which was then trypsin digested and evaluated by liquid chromatography electrospray tandem MS (LC-MS/MS) which identified the presence of amyloidogenic proteins in all cases of MTC. High levels of calcitonin were identified in all 9 cases of MTC. Secretogranin-1 was identified in 6 of 9 MTC. Calcitonin gene-related peptide was identified in 4 of 9 cases of MTC. LC-MS/MS proteomic analysis provides a rapid, highly specific, and sensitive method for identification of the specific type of amyloid in these endocrine tumors. This approach may allow classification of different forms of endocrine amyloid present in neuroendocrine tumors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Amyloid is a characteristic histologic feature in endocrine tumors such as medullary thyroid carcinomas (MTC). Calcitonin has been described as a component of amyloid in MTC. Although amyloid can be readily detected by histochemical stains such as Congo red, the specific amyloid present in tumors is difficult to determine. Recently, mass spectrometry-based proteomic analysis has become increasingly used to subtype amyloid in a variety of clinical settings.
This technique was developed as subtyping of amyloid by the more common method of immunohistochemistry can be difficult due to high background staining due to serum contamination, epitope loss due to formalin fixation causing protein cross-linking, and lack of antibodies for all amyloid subtypes [1, 2]. The technique combines specific sampling by laser microdissection and tandem mass spectrometry-based proteomic analysis [1]. Proteins are isolated from the amyloid deposits, extracted, digested with trypsin, and then analyzed by liquid chromatography tandem mass spectrometry [2]. The resulting mass spectrometry spectra are compared with canonical protein sequence databases and filtered and identified with post-processing software indicating the specific peptides and associated proteins [2].
Mass spectrometry-based proteomic analysis has been used to subtype amyloid in subcutaneous fat aspirates identifying variable gene usage in immunoglobulin light chains and variant peptides in hereditary amyloidosis [3]. This technique has also been used to diagnose and type kidney diseases with amyloid including uncommon and familial forms which are typed based on specific amyloidogenic proteins and immunoglobulins in immune complex and complement factors in complement-mediated glomerulonephritis [4]. In patients with monoclonal gammopathy and cardiac amyloid in which blood and urine studies for monoclonal proteins are inadequate to classify amyloid type, this technique can be used to classify amyloid on endomyocardial biopsies [5]. This technique has not been used to study amyloid in endocrine tumors. We utilized a mass spectrometry-based proteomic analysis to determine if we could identify specific proteins associated with amyloid in MTC.
Materials and Methods
Nine MTC were studied. One case was from a patient with multiple endocrine neoplasia type 2A, one case was from a patient with familial MTC, and seven cases were sporadic MTC. Hematoxylin and eosin-stained sections were evaluated for verification of histologic diagnosis. Clinical information was obtained by chart review.
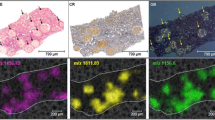
The specific methods of laser microdissection/mass spectrometry have been published previously [1]. Briefly, formalin-fixed paraffin-embedded tissue sections cut at 10 μm were stained with Congo red, and fluorescent light was used to identify areas of Congo red positivity (Fig. 1). In each case, Congo red-positive amyloid plaques were microdissected from the MTC. Four amyloid specimens from each case were evaluated. The collected tissue then was trypsin digested into peptides, reduced with dithiothreitol, and separated by nanoflow liquid chromatography–electrospray tandem mass spectrometry (LC-MS/MS) using a ThermoFinnigan LTQ Orbitrap Hybrid Mass Spectrometer (Thermo Electron, Bremen, Germany) coupled to an Eksigent nanoLC-2D HPLC system (Eksigent, Dublin, CA, USA). The resulting LC-MS/MS data was correlated to theoretical fragmentation patterns of tryptic peptide sequences from the Swissprot database using Scaffold (Mascot, Sequest, and X!Tandem search algorithms). Peptide identifications were accepted if they could be established at greater than 90.0 % probability, and protein identifications were accepted if they could be established at greater than 90.0 % probability and contain at least two identified spectra. The identified proteins were subsequently examined for the presence or absence of amyloid-related peptides.

a Sporadic medullary thyroid with amyloid carcinoma in a 65-year-old male (H&E, 10×). b Sporadic medullary thyroid carcinoma with amyloid in a 66-year-old male (H&E, 10×). c Medullary thyroid carcinoma with amyloid in a 61-year-old male with multiple endocrine neoplasia type 2A. d Congo red apple green birefringence with polarization in medullary thyroid carcinoma from a 61-year-old male with multiple endocrine neoplasia type 2A
Results
The clinical and pathologic findings are presented in Table 1. The patients ranged in age from 22 to 76 years of age, and 4 were female and 5 male. Of the 9 patients, 7 had sporadic MTC, one had familial MTC, and one had MTC in the setting of multiple endocrine neoplasia type 2A. Six of the nine had lymph node metastases at the time of diagnosis. Follow-up ranged from 2 to 12 years. LC MS/MS identified the presence of amyloidogenic proteins in all 9 cases of MTC. All 9 cases had high levels of amyloid signature proteins apolipoprotein A-IV and apolipoprotein E, and 5 of 9 also had serum amyloid P, indicating the material analyzed was amyloid. The correlation between these signature proteins and Congo red amyloid positivity was recently confirmed by Vrana et al. [3]. A mutation database search was also performed on the data from these 9 MTC, and no mutation was identified in the amyloid signature proteins [2].
High levels of calcitonin protein were identified in all cases of MTC. Katacalcin was also identified in all samples. A few peptides of secretogranin-1 were identified in 6 of 9 MTC, and a few peptides of calcitonin gene -peptide-beta (CGRP) were identified in 4 of 9 MTC.
Discussion
Amyloid is a characteristic feature of medullary thyroid carcinoma. Early descriptions of MTC include amorphous material that was identified as amyloid. By electron microscopy, amyloid fibrils have been identified in MTC, and amyloid was confirmed to be a product of the MTC cells by in vitro culture of medullary carcinoma cells [6]. Others have shown that the amyloid fibrils in MTC could not be distinguished from other forms of amyloid occurring naturally or experimentally [7]. Basement membranes were observed between tumor cells and stroma but were usually absent where MTC cells were contiguous with amyloid [6]. The formation of amyloid is predominantly extracellular in MTC [7]. Secretory granules have been identified closely related to the amyloid of MTC, suggesting that the granules may have a role in the formation of the amyloid [8].
Medullary thyroid carcinoma cells contain calcitonin, and calcitonin has been identified in the amyloid stroma by immunohistochemistry and immunofluorescence [9, 10]. Amyloid fibrils from two MTC demonstrated AMCT (amyloid medullary carcinoma of the thyroid) protein to be the major protein in MTC amyloid fibrils [10]. Two different components of amyloid were referred to as the P component which was immunologically homogeneous, and the AMCT protein, which was “immunologically distinct and did not react with various antisera against known amyloid fibril proteins” [10]. The degraded MTC amyloid fibrils and the isolated AMCT protein reacted with antiserum raised against the MTC amyloid proteins but not with other amyloid proteins [10]. Sequence analysis identified the portion of the AMCT protein to be calcitonin, but the molecular weight of the AMCT protein was larger than calcitonin and thought to possibly be a prohormone of calcitonin [10]. A subsequent study directly evaluated the component of MTC after denaturation of amyloid utilizing matrix-assisted laser desorption ionization-time of flight mass spectrometry analysis [11]. Rather than the alternatively processed prohormone of calcitonin as was suggested by prior authors [10], Khurana et al. [11] reported “full-length calcitonin is the sole constituent of amyloid in MTC.” The authors noted it would be “much better to perform MS/MS analysis to say with complete authority that calcitonin is involved in amyloid formation in MTC tissue” and attempted MS/MS but were not able to obtain satisfactory results which they attributed most likely due to insufficient sample size [11].
By liquid chromatography electrospray tandem MS, we were able to demonstrate calcitonin protein in all 9 cases of amyloid in the MTCs in our study. All four amyloid specimens from each case showed calcitonin protein in all 9 cases of MTC. (Pro)calcitonin is the precursor protein of ACal fibril protein in C-cell thyroid tumors [12]. Our analysis identified peptides mapping to both calcitonin and katacalcin (Fig. 2). Calcitonin and katacalcin were identified in all samples and showed complete coverage. These peptides were independently mapped to the calcitonin precursor entry in the Swiss protein database which is a concatenated sequence containing the signaling peptide (amino acids 1–25), the propeptide (amino acids 25–82), calcitonin protein (amino acids 85–116), and katacalcin protein (amino acids 121–141). Katacalcin is a member of the calcitonin gene family and is a calcium-lowering hormone. Katacalcin flanks calcitonin in the human calcitonin precursor—which is cleaved into calcitonin and katacalcin. The amyloid fibril proteins are designated protein A followed by the abbreviated form of the precursor protein [12]. Thus, “A” with suffix of “Cal” or “ACal” for the fibril protein in C-cell thyroid tumors. The full-length sequences for both calcitonin and katacalcin were detected via mass spectrometry indicating the proteins were intact and not truncated. The proteins were also detected in the absence of any variable modification allowance in the bioinformatics software suggesting the proteins lack any significant amidation, glycosylation, or other post-translational modifications.

Sequence coverage of the calcitonin precursor identified by laser microdissection mass spectrometry. Yellow highlights indicate identified amino acids
Calcitonin and katacalcin are not unique as proteins to be identified in the amyloid state. There are approximately 50 disorders associated with misfolding of normal functional peptides and proteins that can result in aggregates such as amyloid [13]. The amyloid state has been described as “generic” as can be adopted by many proteins and peptides and is not associated with a specific amino acid sequence [13]. Proteinaceous deposits in misfolding diseases have amyloid characteristics, but the sequences, native structures, and protein functions do not have obvious similarities [13, 14]. The specific mechanism for calcitonin and katacalcin to be in the amyloid state in some cases of MTC remains unclear. Protein concentrations in these tumors could be associated the amyloid state. Thermodynamic studies have shown that conversion into the amyloid state will take place when its free energy is lower than that of its native state and the stability of the amyloid state is dependent on the protein concentration [13]. Maintenance of solubility, free energy barriers with transitions between states, rates of synthesis and degredation, interactions with chaperones, or other modifications may have a role.
Secretograin-1 was identified in 6 of 9 MTC and calcitonin gene-related peptide in 4 of 9 MTC in our study. The finding of only a few peptides each of secretogranin-1 and calcitonin gene-related peptide in a subset of the cases in our study is unclear. As there were only a few signals of these peptides, their significance to the amyloid remains uncertain. It is possible that they may be associated with the amyloid, but it is also possible that they may be artifact or contaminant as they were seen at low levels and not in every case and not in every sample of each case where it was identified—unlike calcitonin which was identified at high levels in every sample of every case. Secretogranin-1 (chromogranin-B) is a neuroendocrine secretory granule protein and member of the chromogranin/secretogranin family [15]. Calcitonin gene-related peptide-beta (CGRP) was identified in 4 of 9 MTC. This peptide is part of the calcitonin family of peptides. The mitogen-activated protein kinases signaling pathway and cytokines are involved in regulating the CGRP gene [16, 17]. CGRP receptors are identified in many tissues, and CGRP is associated with the cardiovascular system, with pain, vasodilation, cutaneous epithelium, and wound healing, among many other roles [18, 19].
In conclusion, we utilized a novel mass spectrometry-based proteomic analysis and identified calcitonin associated with amyloid in all 4 samples in each of all 9 cases of MTC (1 multiple endocrine neoplasia type 2A, 1 familial MTC, and 7 sporadic MTC) studied. LC-MS/MS proteomic analysis provides a rapid, highly specific, and sensitive method for the analysis of the specific type of amyloid in these tumors. This approach may allow for the classification of different forms of endocrine amyloid present in neuroendocrine tumors.
References
Vrana JA, Gamez JD, Madden BJ et al. Classification of amyloidosis by laser microdissection and mass spectrometry-based proteomic analysis in clinical biopsy specimens. Blood 114(24):4957–4959, 2009.
Dasari S, Theis JD, Vrana JA et al. Clinical proteome informatics workbench detects pathogenic mutations in hereditary amyloidoses. J Proteome Res. 13(5):2352–23588, 2014
Vrana JA, Theis JD, Dasari S, et al. Clinical diagnosis and typing of systemic amyloidosis in subcutaneous fat aspirates by mass spectrometry-based proteomics. Haematologica. 99(7):1239–1247, 2014.
Sethi S, Vrana JA, Theis JD, Dogan A. Mass spectrometry based proteomics in the diagnosis of kidney disease. Curr Opin Nephrol Hypertens. 22(3):273–80, 2013.
Maleszewski JJ, Murray DL, Dispenzieri A, et al. Relationship between monoclonal gammopathy and cardiac amyloid type. Cardiovasc Pathol. 22(3):189–194, 2013.
Albores-Saavedra J, Rose GG, Ibanez ML et al. The amyloid in solid carcinoma of the thyroid gland: staining characteristics, tissue cultures and electron microscopic observations. Lab Invest 13:77–89, 1964.
Meyer JS. Fine structure of two amyloid-forming medullary carcinomas of thyroid. Cancer 21(3):406–425, 1968.
Meyer JS, Hutton WE, Kenny AD. Medullary carcinoma of thyroid gland. Subcellular distribution of calcitonin and relationship between granules and amyloid. Cancer 31(2):433–41, 1973
Arnal-Monreal FM, Goltzman D, Knaack J, Wang NS, Huang SN. Immunohistologic study of thyroidal medullary carcinoma and pancreatic insulinoma. Cancer 40(3):1060–1070, 1977.
Sletten K, Westermark P, Natvig JB. Characterization of amyloid fibril proteins from medullary carcinoma of the thyroid. J Exp Med 143(4):993–998, 1976.
Khurana R, Agarwal A, Bajpai VK, et al. Unraveling the amyloid associated with human medullary thyroid carcinoma. Endocrinology 145(12):5465–5470, 2004.
Sipe JD, Benson MD, Buxbaum JN, Ikeda, S, Merlini G, Saraiva MJM, Westermark P. Nomenclature 2014: Amyloid fibril proteins and clinical classification of the amyloidosis. Amyloid 21(4):221–224, 2014.
Knowles TPJ, Vendruscolo M, Dobson CM. The amyloid state and its association with protein misfolding diseases. Nat Rev Mol Cell Biol 15:384–396, 2014.
Chiti F and Dobson CM. Protein misfolding, functional amyloid, and human disease. Annu Rev Bioch 75:333–366, 2006.
Benedum UM, Lamouroux A, Konecki DS, et al. The Primary structure of human secretogranin I (chromogranin B): comparison with chromogranin A reveals homologous terminal domains and a large intervening variable region. EMBO J 6(5): 1203–1211, 1987.
Durham P and Russo A. Stimulation of the calcitonin gene-related peptide enhancer by mitogen-activated protein kinases and repression by an antimigraine drug in trigeminal ganglia neurons. J Neurosci 23(3):807–815, 2003
Schafers M, Svensson CI, Sommer C, Sorkin LS. Tumor necrosis factor-alpha induces mechanical allodynia after spinal nerve ligation by activation of p38 MAPK in primary sensory neurons. J Neurosci 23(7):2517–2521, 2003.
Arulmani U, VanDenBrink AM, Villalon CM, Saxena PR. Calcitonin gene-related peptide and its role in migraine pathophysiology. Eur J Pharmacol 500(1–3):315–330, 2004.
Russell FA, King R, Smillie SJ, et al. Calcitonin gene-related peptide: physiology and pathophysiology. Brain Physiological Reviews 94(4):1099–1142, 2014.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Erickson, L.A., Vrana, J.A., Theis, J. et al. Analysis of Amyloid in Medullary Thyroid Carcinoma by Mass Spectrometry-Based Proteomic Analysis. Endocr Pathol 26, 291–295 (2015). https://doi.org/10.1007/s12022-015-9390-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12022-015-9390-7