
Abstract
The proposed diagnostic criteria for poorly differentiated thyroid carcinoma (known as the Turin classification) were defined based on growth pattern (solid, trabecular, or insular) and high-grade morphologic features (nuclear pleomorphism, mitoses including abnormal forms, and coagulative tumor necrosis). The development of this classification specifically did not include tumors with oncocytic or Hürthle cell cytology, and only sparse literature describing poorly differentiated oncocytic carcinomas is available. In this study, we examined a cohort of 284 cases of oncocytic follicular carcinoma/Hürthle cell carcinoma (OFC/HCC) and identified 17 cases of oncocytic variant of poorly differentiated carcinoma (OV-PDTC) based on Turin criteria. Compared to minimally invasive and angioinvasive OFC/HCC, these tumors arose in older patients (range 44–88 years; average 71 years), were larger (average size 4.5 cm), and all had extensive vascular invasion (5–15 foci), and coagulative tumor necrosis and the tumor cells were arranged in a trabecular or solid growth pattern. All showed an admixture of oncocytic follicular/Hürthle cells arranged in solid and trabecular growth pattern. Aggregates of small sized cells with minimal eosinophilic cytoplasm, comprising 10–20 % of the entire tumor mass were also seen in 16/17 cases. Clinical follow-up was available in 12 cases and ranged from 6 to 120 months (average 41 months). Distant metastases were seen in 10/12 (83 %) patients; two had lung and one had bone metastases at the time of thyroid surgery, and four subsequently developed cervical lymph node metastases. Two patients died of disease, and ten are alive either with or free of tumor. The OV-PDTC is a distinct entity which can be identified based on Turin criteria and the presence of a distinct “small cell” component. It is frequently associated with regional recurrence and distant metastases and can lead to tumor-related demise.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Until the publication of the seminal papers [1, 2] defining and illustrating “insular thyroid carcinoma,” the concept and pathological features of poorly differentiated thyroid carcinoma were not uniformly recognized. Pathologists and clinicians believed tumors of follicular derivation were either well differentiated (papillary or follicular carcinoma) or anaplastic (undifferentiated) carcinoma. For most pathologists (despite some controversy), oncocytic follicular or Hürthle cell carcinomas were grouped with follicular thyroid carcinoma. Carcangiu et al. [1] and Sakamoto et al. [2] described and illustrated a group of tumors with clinical and pathologic features in between the two main existing categories. Carcangiu et al. termed these as “insular carcinoma” based on microscopic growth pattern [1]. In the next few decades, the concept of poorly differentiated carcinoma had been discussed in the literature in small case series [3, 4]; however, many pathologists still continued to classify these tumors as follicular carcinomas [5, 6].
In 2006, a group of internationally known thyroid pathologists defined “Turin criteria” for the diagnosis of poorly differentiated thyroid carcinoma (PDTC) [7]. These criteria include the following: (1) presence of a solid/trabecular/insular pattern of growth; (2) absence of the conventional nuclear features of papillary carcinoma; and (3) presence of at least one of the following features: mitotic activity ≥3/10 high-power fields (HPFs), tumor necrosis, and convoluted nuclei.
The criteria were applied to conventional follicular thyroid carcinoma and papillary thyroid carcinoma, but oncocytic type/Hürthle cell thyroid carcinoma (OFC/HCC) was excluded in that study. However, the World Health Organization (WHO) classification does recognize oncocytic variant of conventional PDTC based on Turin criteria [8]. Only one study has established that the Turin criteria can be applied to oncocytic carcinomas, and this classification can have prognostic implications [9]. The study found that OV-PDTC has shorter survival time and tumor-specific survival as compared to differentiated carcinomas. However, this study did not address the difference between the OV-PDTC and other types of oncocytic follicular thyroid carcinoma, such as minimally invasive and angioinvasive types but differentiated lesions. In this case series, we report our institutional experience with 17 cases of OV-PDTC.
Materials and Methods
The surgical pathology database of Hospital of the University of Pennsylvania and consultation databases of Drs. V. A. LiVolsi and ZW Baloch from Jan 2004 to July 2012 were searched and 284 cases of OFC/HCC (279 primaries and 5 recurrence or metastasis) were identified. There were 136 primary minimally invasive oncocytic carcinomas and 131 primary angioinvasive oncocytic carcinomas identified. The diagnosis of oncocytic lesion was based on greater than 70 % of the tumor showing oncocytic cells, i.e., round to polygonal cells with eosinophilic cytoplasm and round nuclei with prominent nucleoli. The diagnosis of minimally invasive carcinoma was rendered when the tumor showed broad-based invasion into and through the tumor capsule without evidence of angioinvasion, whereas the diagnosis of angioinvasive carcinoma was rendered when unequivocal tissue fragment(s) of tumor cells was present within the capsular vessels enveloped by endothelial cells and attached to the vessel wall. Seventeen patients (12 primaries, 5 neck recurrence and/or metastasis) with OV-PDTC were selected for this study. The available histologic slides were reviewed and the diagnoses were confirmed based on the Turin criteria. Clinical follow-up was obtained from electronic medical records. We compared OV-PDTC to the minimally invasive and angioinvasive oncocytic carcinomas by using Student’s t test, chi-squared test, and by analyzing features such as age, gender, tumor size, and follow-up data.
Results
Clinicopathologic Features
The 17 cases of OV-PDTC occurred in eight male and nine female patients with average age of 71 years (range from 44 to 88 years). The size of the primary intrathyroidal tumor was available in 15 cases (either measured from available slides and/or from pathology reports); 80 % were larger than 4.0 cm (average size 4.5 cm). In the 12 primary OV-PDTC examined, six were partially encapsulated and six were grossly invasive. Lymph node metastases were seen in two and distant metastases in three (two to lung and one to bone) patients at the time of thyroid resection. Two patients died of the disease (Table 1).
All tumors showed an admixture of oncocytic follicular/Hürthle cell arranged in solid and trabecular growth pattern (Fig. 1a, b). Extensive vascular invasion (5–15 foci) and tumor necrosis (Fig. 2) were noted in all except one case. The one case without necrosis was diagnosed as poorly differentiated carcinoma based on solid and trabecular growth pattern, marked nuclear pleomorphism, mitoses, and extensive vascular invasion. When present, the foci of necrosis were multifocal and comprised between 10 and 30 % of the total tumor size. These showed definite coagulative necrosis of tumor cells and were devoid of reactive changes such as granulation tissue formation and hemosiderin laden macrophages due to preoperative fine-needle aspiration. Nuclear pleomorphism was readily evident; this was characterized by large nuclei with bizarre shapes, irregular nuclear membranes, and dense chromatin (Fig. 3). None of the cases demonstrated convoluted nuclei as described by Volante and colleagues [9]. Interestingly, 16/17 (94 %) cases also had one or more aggregates of a distinct population of small sized cells with hyperchromatic irregular nuclei, lack of prominent nucleoli with scant eosinophilic cytoplasm, comprising 10–20 % of the entire tumor mass (Fig. 4). Four cases showed two to three mitotic figures/10 HPFs while 12 showed more than three mitoses/10 HPFs (Table 2).

Oncocytic poorly differentiated thyroid carcinoma. a, b Oncocytic tumor cells arranged in insular/solid and trabecular growth patterns (hematoxylin and eosin stain, 10× and 60×)

Spontaneous necrosis in oncocytic poorly differentiated thyroid carcinoma (hematoxylin and eosin stain, 40×)

Marked nuclear pleomorphism in oncocytic poorly differentiated thyroid carcinoma characterized by large nuclei with nuclear membrane changes and prominent nucleoli (hematoxylin and eosin stain, 60×)

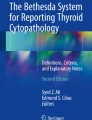
Small cell component in oncocytic poorly differentiated thyroid carcinoma characterized by small pleomorphic nuclei with even chromatin, lack of nucleoli and scant cytoplasm (hematoxylin and eosin stain, 60×)

Focal to absence of thyroglobulin immunostaining in a case of oncocytic poorly differentiated oncocytic follicular carcinoma (peroxidase immunostain, 40×)
Immunohistochemical stains were performed in seven cases in which tissue blocks were available, the poorly differentiated component demonstrated minimal to or lack of staining for thyroglobulin (Fig. 5). Ki-67 immunostaining was performed in three cases and showed 8–40 % proliferative index correlating with the increased mitotic count.
Statistical Analysis
We compared the OV-PDTC (17 cases) to minimally invasive (13 cases) and angioinvasive ODC/HCCA cases by employing Student’s t test and chi-squared test.
Gender
The ratios of male and female were 1:6, 1:2, and 1:1 for minimally invasive, angioinvasive, and OV-PDTC groups, respectively (Table 1). Statistically (p < 0.01, chi-squared test), there is a relationship between the gender and tumor subtype, with the advanced disease noted more frequently in male patients.
Age and Size
The average age was 54.3, 57.3, and 71 years for minimally invasive, angioinvasive, and OV-PDTC groups, respectively (Table 1). The Student’s t test showed no significant difference between minimally invasive and angioinvasive groups (p = 0.23). However, significant differences were noted between minimally invasive and PDTC (p < 0.001) and angioinvasive and OV-PDTC (p < 0.001) groups, respectively. The average size of the tumors was 2.78, 3.87, and 4.5 cm for minimally invasive, angioinvasive, and OV-PDTC groups, respectively (Table 1). There were significant differences between minimally invasive and angioinvasive (p < 0.001), angioinvasive and OV-PDTC (p = 0.008), and minimally invasive and OV-PDTC (p < 0.001) groups, respectively [10].
Clinical Follow-Up
The follow-up data was available in 18, 43, and 12 cases for minimally invasive, angioinvasive, and OV-PDTC, respectively (Table 2). The follow-up period ranged from 5 to 147 (average 105 months), 1–212 (average 57 months), and 4–120 months (average 51 months) for these three groups, respectively. One case (6 %) of minimally invasive group developed lung and lymph node metastases after 90 months. Ten patients (23 %) in the angioinvasive group developed either recurrences or remote metastases after 4–96 months of follow-up. Three patients with minimally invasive tumors (17 %) and 17 with angioinvasive lesions (40 %) have been lost to follow-up after 1 year without recurrence. The remaining patients in these two groups are alive either with or free of tumor. For OV-PDTC group, two patients suffered from recurrences and ten (10/12; 83 %) had distant metastases (lung, liver, brain, and/or bone) to one or more sites. Of these, two had lung, two had lymph node, and one had bone metastasis at the time of thyroid surgery. Subsequently, three patients developed cervical lymph node metastases and seven developed distant metastases. Two patients (17 %) died of the disease, and 10 (67 %) are alive either with tumor or are free of tumor. The remaining five patients were lost to follow-up after 1 year without disease.
The Student’s t test analysis data showed that there is no significant difference between OV-PDTC and angioinvasive carcinomas for the time to develop either recurrence or metastasis (p = 0.78). However, the recurrence and metastasis rate for OV-PDTC was higher than minimally and angioinvasive groups (p < 0.01, chi-squared test).
Discussion
In general, oncocytic change of cells is defined as cellular enlargement characterized by an abundant eosinophilic granular cytoplasm as a result of the accumulation of altered mitochondria [11, 12]. In the thyroid, these cells are often referred to as oncocytic follicular/Hürthle cells (OF/HC), which are characterized by large size, polygonal to square shape, distinct cell borders, voluminous granular, and eosinophilic cytoplasm, and a large hyperchromatic nucleus with prominent “cherry pink” nucleoli [13]. Studies of thyroid neoplasms composed predominantly (>75 %) of OF/HC have shown that the larger the lesion, the more likely it is to show invasive characteristics. Hence, an OF/HC tumor that is 4 cm or greater has an 80 % chance of showing histological evidence of malignancy [14–21]. However, small OF/HC carcinomas (less than 2 cm) can occur and can be associated with aggressive clinical course.
It has been reported that OF/HC carcinomas with widespread metastatic spread have a worse prognosis that do nononcocytic follicular carcinomas matched for stage and patient parameters; this might be attributable to the reduced capacity for radioactive iodine uptake that these lesions may exhibit [22–24]. The loss of effectiveness of this targeted treatment results in increased morbidity and mortality.
As with follicular carcinomas, malignancy is based on the identification of capsular and/or vascular invasion. We believe that vascular invasion warrants identification with specific classification as angioinvasive carcinoma. The criteria are similar to those applied to diagnose follicular carcinoma.
The term “poorly differentiated carcinoma of the thyroid gland” (PDTC) was first described in 1963, but no diagnostic criteria were provided at that time [25]. Since then, numerous studies have shown that patients with these tumors have an adverse outcome compared to conventional well-differentiated carcinomas of the thyroid [26–31]. It is now generally accepted that PDTC is an entity biologically located midway in the spectrum between classic well-differentiated follicular epithelium-derived carcinomas and anaplastic thyroid carcinomas [8]. An attempt to establish diagnostic criteria for PDTC occurred in 2006 when these tumors were defined based on both growth pattern and high-grade features [7]. Consequently, oncocytic PDTC can be regarded as a variant of conventional PDTC [8]. However, this variant was explicitly excluded from the Turin criteria, although it has long been known that oncocytic thyroid tumors can have an adverse outcome [5, 7–9, 32].
The present study can answer whether the Turin criteria can be applied to oncocytic variant follicular carcinoma in the affirmative. In our 17 OV-PDTC cases, all had vascular invasion and more importantly, PDTC’s features, solid/trabecular growth pattern, necrosis, and high mitotic rates [3, 9]. The finding of “small cell” component characterized by cells with hyperchromatic nuclei and scant eosinophilic cytoplasm was an interesting finding in our cases; this has not been reported previously. These foci were limited in quantity, i.e., 10–20 % of the entire tumor mass and were devoid of necrosis.
These areas of “small cells” were distinctly noticeable within the tumor at low magnification as they stand out against a background of oncocytic cells with abundant cytoplasm. In two of our cases, these small cell foci appeared in metastatic sites (lung); small biopsies (transbronchial specimens) were difficult to interpret as metastases from the thyroid tumors since they showed immunoreactivity for TTF-1 but not for thyroglobulin. Hence, a separate primary lung carcinoma was considered. On review of the original thyroid tumors in these cases, the small cell areas shared similar immunostaining results while the oncocytic areas demonstrated staining for thyroglobulin (often focal) as well as TTF-1.
Compared to minimally invasive and angioinvasive cases, patients with OV-PDTC are older (average age 71 years old) and the behavior of the tumors is more aggressive with more numerous foci of vascular invasion and a higher tumor-related mortality. Statistical significance was noted among these three groups. The OV-PDTC occurred equally in both genders; however, advanced disease was more frequent in male patients. Comparing the sizes, the OV-PDTC presented as a large tumors with local and distant metastases at the time of diagnosis. The clinical follow-up of our cohort demonstrated significant differences between the minimally invasive and OV-PDTC; however, the differences were negligible between angioinvasive OF/HC carcinoma and OV-PDTC. Papotti et al. identified a group of OF/HC carcinomas of the thyroid with solid or trabecular growth pattern (they called it poorly differentiated oxyphilic (Hürthle cell) carcinoma) in 1996 and found that these patients had a worse prognosis comparing with Hürthle cell carcinoma with a predominant follicular pattern [33]. Most recently, Dettmer et al. demonstrated that there is a significant difference in the overall and tumor-specific survival for poorly differentiated oncocytic thyroid carcinoma (OV-PDTC) compared to conventional PDTC [9]. However, they did not address the difference between the OV-PDTC and other types of oncocytic thyroid carcinoma, as in this study.
Based on our data, we concluded the Turin criteria can be applied to “poorly differentiated oncocytic variant/Hürthle cell follicular thyroid carcinoma” and OV-PDTC are associated with a more aggressive clinical behavior and more serious prognosis than minimally invasive and angioinvasive oncocytic thyroid follicular carcinoma.
References
Carcangiu ML, Zampi G, Rosai J. Poorly differentiated ("insular") thyroid carcinoma. A reinterpretation of Langhans' "wuchernde Struma". Am J Surg Pathol1984; 8:655–668
Sakamoto A, Kasai N, Sugano H. Poorly differentiated carcinoma of the thyroid. Cancer1983; 52:1849–1855
Hiltzik D, Carlson DL, Tuttle RM, Chuai S, Ishill N, Shaha A, Shah JP, Singh B, Ghossein RA. Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: a clinicopathologic study of 58 patients. Cancer2006; 106:1286–1295
Volante M, Landolfi S, Chiusa L, Palestini N, Motta M, Codegone A, Torchio B, Papotti MG. Poorly differentiated carcinomas of the thyroid with trabecular, insular, and solid patterns: a clinicopathologic study of 183 patients. Cancer2004; 100:950–957
Akslen LA, LiVolsi VA. Poorly differentiated thyroid carcinoma—it is important. American Journal of Surgical Pathology2000; 24:310–313
Akslen LA, LiVolsi VA. Prognostic significance of histologic grading compared with subclassification of papillary thyroid carcinoma. [see comments]. Cancer2000; 88:1902–1908
Volante M, Collini P, Nikiforov YE, Sakamoto A, Kakudo K, Katoh R, Lloyd RV, LiVolsi VA, Papotti M, Sobrinho-Simoes M, Bussolati G, Rosai J. Poorly differentiated thyroid carcinoma: the Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol2007; 31:1256–1264
DeLellis RA, Lloyd RD, Heitz PU, Eng C, eds. WHO: Pathology and Genetics. Tumours of Endocrine Organs. Lyon, France: IARC Press; 2004. Kleihues P, Sobin LE, eds. WHO Classification of Tumours
Dettmer M, Schmitt A, Steinert H, Moch H, Komminoth P, Perren A. Poorly differentiated oncocytic thyroid carcinoma—diagnostic implications and outcome. Histopathology2012; 60:1045–1051
Samulski TD, Bai S, LiVolsi VA, Montone K, Baloch Z. Malignant potential of small oncocytic follicular carcinoma/Hurthle cell carcinoma: an institutional experience. Histopathology2013; 63:568–573
Friedman N. Celluar involution in thyroid gland; significance of Hürthle cells in myxedema, exhaustion atrophy, Hashimoto's disease and reaction to irradiation, thiouracil therapy and subtotal resection. J Clin Endocrinol Metab1949; 9:874–882
Sobrinho-Simoes MA, Nesland JM, Holm R, Sambade MC, Johannessen JV. Hurthle cell and mitochondrion-rich papillary carcinomas of the thyroid gland: an ultrastructural and immunocytochemical study. Ultrastruct Pathol1985; 8:131–142
Asa SL. My approach to oncocytic tumours of the thyroid. J Clin Pathol2004; 57:225–232
Bronner M, LiVolsi V. Oxyphilic (Askanazy/Hurthle cell) tumors of the thyroid: Microscopic features predict biologic behavior. Surg Pathol1988; 1:137–150
Thompson N, Dun E, Batsakis J, Nishiyama R. Hürthle cell lesions of the thyroid gland. Surg Gynecol Obstet1974; 139:555–560
Johnson TL, Lloyd RV, Burney RE, Thompson NW. Hurthle cell thyroid tumors. An immunohistochemical study. Cancer1987; 59:107–112
Arganini M, Behar R, Wu TC, Straus F, 2nd, McCormick M, DeGroot LJ, Kaplan EL. Hurthle cell tumors: a twenty-five-year experience. Surgery1986; 100:1108–1115
Gosain AK, Clark OH. Hurthle cell neoplasms. Malignant potential. Archives of Surgery1984; 119:515–519
Har-El G, Hadar T, Segal K, Levy R, Sidi J. Hurthle cell carcinoma of the thyroid gland. A tumor of moderate malignancy. Cancer1986; 57:1613–1617
Flint A, Lloyd RV. Hurthle-cell neoplasms of the thyroid gland. Pathol Annu1990; 25 Pt 1:37–52
Carcangiu ML, Bianchi S, Savino D, Voynick IM, Rosai J. Follicular Hurthle cell tumors of the thyroid gland. Cancer1991; 68:1944–1953.
Rosai J, Carcangui ML, DeLellis RA. Tumors of The Thyroid Gland. Vol 3rd Series, Fascicle 5. Washington, DC: Armed Forces Institute of Pathology.
Gundry S, Burney R, Thompson N, Lloyd R. Total thyroidectomy for Hürthle cell neoplasm of the thyroid gland. Arch Surg1983; 118:529–553
Watson R, Brennan M, Goellner J, van Heerden J, McConahey W, Taylor W. Invasive Hürthle cell carcinoma of the thyroid: natural history and management. Mayo Clin Proc1984; 59:851–855
Granner DK, Buckwalter JA. Poorly differentiated carcinoma of the thyroid gland. Surg Gynecol Obstet1963; 116:650–656
Papotti M, Botto Micca F, Favero A, et al. Poorly differentiated thyroid carcinomas with primordial cell component: A group of aggressive lesions sharing insular, trabecular and solid patterns. Am J Surg Pathol1993; 17:291
Pilotti S, Collini P, Manzari A, Marubini E, Rilke F. Poorly differentiated forms of papillary thyroid carcinoma: distinctive entities or morphological patterns? Semin Diagn Pathol1995; 12:249–255
Pilotti S, Collini P, Mariani L, Placucci M, Bongarzone I, Vigneri P, Cipriani S, Falcetta F, Miceli R, Pierotti MA, Rilke F. Insular carcinoma: a distinct de novo entity among follicular carcinomas of the thyroid gland. Am J Surg Pathol1997; 21:1466–1473
Decaussin M, Bernard MH, Adeleine P, Treilleux I, Peix JL, Pugeat M, Tourniaire J, Berger N. Thyroid carcinomas with distant metastases: a review of 111 cases with emphasis on the prognostic significance of an insular component. Am J Surg Pathol2002; 26:1007–1015
Sobrinho-Simoes M, Sambade C, Fonseca E, Soares P. Poorly differentiated carcinomas of the thyroid gland: a review of the clinicopathologic features of a series of 28 cases of a heterogeneous, clinically aggressive group of thyroid tumors. Int J Surg Pathol2002; 10:123–131
Asioli S, Erickson LA, Righi A, Jin L, Volante M, Jenkins S, Papotti M, Bussolati G, Lloyd RV. Poorly differentiated carcinoma of the thyroid: validation of the Turin proposal and analysis of IMP3 expression. Mod Pathol2010; 23:1269–1278
Lazzi S, Spina D, Als C, Tosi P, Mazzucchelli L, Kraft R, Laissue JA, Cottier H. Oncocytic (Hurthle cell) tumors of the thyroid: distinct growth patterns comparedwith clinicopathological features. Thyroid1999; 9:97–103
Papotti M, Torchio B, Grassi L, et al. Poorly differentiated oxyphilic (Hurthle cell) carcinomas of the thyroid. Am J Surg Pathol1996; 20:686–694
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bai, S., Baloch, Z.W., Samulski, T.D. et al. Poorly Differentiated Oncocytic (Hürthle Cell) Follicular Carcinoma: an Institutional Experience. Endocr Pathol 26, 164–169 (2015). https://doi.org/10.1007/s12022-015-9367-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12022-015-9367-6