
Abstract
Background
Italian consensus for the classification and reporting of thyroid cytology was published in 2014 and it has been used in almost all Italian institutions. To date, there are not solid data on the reliability of Italian consensus for the classification and reporting of thyroid cytology in classifying low and high risk indeterminate nodules (Tir 3A and Tir 3B, respectively). Here, we reviewed and meta-analyzed the results of published articles to obtain evidence-based information on this topic.
Research design and methods
A comprehensive literature exploration of online databases was conducted by searching all published papers citing Italian consensus for the classification and reporting of thyroid cytology. The search was updated until June 2017, and references of the retrieved articles were also screened. Only original articles reporting histologic follow-up of nodules cytologically classified as Tir 3A and Tir 3B were eligible for inclusion.
Results
The literature search revealed 62 articles and six of these were eligible for the study. All papers were retrospective and published very recently. Overall, 423 indeterminate lesions, of which 180 Tir 3A and 243 Tir 3B, were found. Of these, 29 cancers were recorded in Tir 3A and 127 in Tir 3B. The pooled rate of malignancy was 17% (95% CI = 12 to 22%) in Tir 3A and 52% (95% CI = 46 to 58%) in Tir 3B. No significant publication bias was evident.
Conclusions
Italian consensus for the classification and reporting of thyroid cytology 2014 shows high reliability in discriminating indeterminate lesions at low risk of malignancy from those at high risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cytology from fine-needle aspiration (FNA) is recognized as a main tool for the evaluation of thyroid nodules [1, 2]. The main limit of thyroid FNA is represented by indeterminate reports which occur with a non-negligible rate (i.e., up to 20–25% in different institutions). In presence of an indeterminate FNA report, the histologic examination after surgery is still the more frequently adopted way to achieve a diagnosis. Unfortunately, only one in four of all indeterminate nodules is cancer at final histology. Thus, to preoperatively diagnose thyroid nodules cytologically classified as indeterminate has represented one major challenge in clinical thyroidology [3]. Many imaging or molecular parameters have been investigated in this context [4,5,6,7,8,9,10,11]. However, to date there is no international consensus to use these tools for the management of patients in clinical practice.
In the last decades several international societies have published their guidelines for reporting thyroid cytology. A major challenge of these cytologic systems was to discriminate, between all indeterminate lesions, those at high risk of malignancy requiring surgery from that at low risk in which we could plan a clinical/ultrasonographic follow-up [12]. Specifically, the British Thyroid Association proposed the subclassification Thy 3a (low risk) and Thy 3f (high risk) [13] and Bethesda system the subcategories Category III (low risk) and IV (high risk) [14]. After these, the Italian consensus for the classification and reporting of thyroid cytology (ICCRTC) reported a five-classes system with a subclassification of Tir 3 in Tir 3A (low risk) and Tir 3B (high risk) [15]. Specifically, Tir 3A is defined as increased cellularity with numerous microfollicular structures in a background of scant colloid, where the proportion of microfollicles is not sufficient for the diagnosis of follicular neoplasm; this category also includes partially compromised samples (i.e., preparation artifacts or blood contamination of specimens), with cytologic or architectural alterations that cannot be confidently classified as benign nor otherwise categorized. Conversely, Tir 3B is characterized by high cellularity in a monotonous microfollicular/trabecular arrangement, with scant or absent colloid, that is suggestive for follicular neoplasm; in addition, of very high interest, the Italian classification includes in the subcategory Tir 3B those cases with “mild/focal nuclear atypia”. The latter represents the most significant difference between Italian system and British and Bethesda ones which include the atypia in their categories of indeterminate at low risk, i.e., Thy 3a [13] and Category III [14], respectively. The decision of ICCRTC was mainly based on the high rate of malignancy (25 %) reported in the Category III of Bethesda system until that moment [16, 17]. Currently, no published data are available on the reliability of ICCRTC and in particular on cancer rate of Tir 3A and Tir 3B. Instead, no significantly difference was found in a meta-analysis of papers reporting the performance of Category III and Category IV of Bethesda [18].
Here, we aimed to systematically review all published papers reporting the rate of malignancy at final postoperative histology of thyroid nodules with presurgical FNA diagnosis of Tir 3A or Tir 3B according to the ICCRTC. Furthermore, to obtain more robust evidence from these data, a meta-analysis of the published articles was also attempted.
Material and methods
Search strategy
A comprehensive literature search in online databases of Google Scholar and Scopus was conducted by searching all papers citing the Italian consensus for the classification and reporting of thyroid cytology (i.e., we searched by using the original title of the ICCRTC “Italian consensus for the classification and reporting of thyroid cytology” and then retrieved all papers with this article cited in the references list). This allowed us to retrieve studies reporting a series of nodules undergone FNA and classified according to ICCRTC. A beginning date limit was not used, the search was updated until June 20, 2017 and no language restriction was used. To try to expand our search, references of the retrieved articles were also screened to identify additional studies.
Study selection
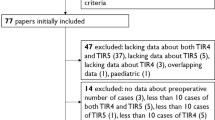
Only original articles that reported complete data of nodules with indeterminate FNA according to ICCRTC were eligible for inclusion: the main exclusion criteria were articles that did not provide histologic follow-up of the indeterminate nodules and studies with overlapping patient data. Cases reports were also excluded. Two researchers (PT, LG) independently reviewed titles and abstracts of the retrieved articles, applying the above criteria; then, the same researchers independently reviewed the full-text version of the remaining articles to determine their final inclusion.
Data extraction
For each included study, information was abstracted concerning study data (authors, year of publication and country of origin); number of patients evaluated; number of thyroid cancers and thyroid benignancy detected.
Statistical analysis
The prevalence of cancers among the categories Tir 3A and Tir 3B was obtained from individual studies using the formula: number of cancers/number of thyroid nodules × 100. For statistical pooling of the data, DerSimonian and Laird method (random-effects model) [19] was used. In this model, pooled data represent weighted averages related to the sample size of the individual studies. Pooled data were presented with 95% confidence intervals (95%CI) and displayed using a forest plot. I-square index was used to quantify the heterogeneity among the studies, and a significant heterogeneity was defined as an I-square value > 50%. Egger’s test was carried out to evaluate the possible presence of a significant publication bias. Statistical analyzes were performed using the StatsDirect statistical software version (StatsDirect Ltd; Altrincham, UK).
Results
Eligible articles
The comprehensive computer literature search revealed 62 articles. Review of titles and abstracts excluded 56 articles according to the above criteria, and six articles [20,21,22,23,24,25] were finally included.
Qualitative analysis (systematic review)
All the included studies were retrospective and were published by Italian authors. Data on the final histologic follow-up were clearly identified in all these manuscripts and the true percentage of malignancy could be calculated. Table 1 details the characteristics and findings of the six included studies. Out of the six papers, one aimed to evaluate the reliability of core needle biopsy in indeterminate nodules [20], two investigated the reliability of ultrasound parameters to predict malignancy [22, 24], and the remaining three [21, 23, 25] reported institutional experiences in indeterminate thyroid nodules with specific focus on the new ICCRTC. Total cases of indeterminate nodules with postoperative histologic follow-up was 423 and 156 (36.9%) of these were malignant. Table 2 describes the results of the 6 studies in the subcategories Tir 3A and Tir 3B.
Quantitative analysis (meta-analysis)
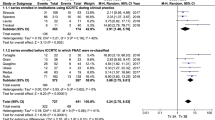
The rate of malignancy among the pooled series of indeterminate thyroid nodules at low risk according to ICCRTC (Tir 3A) was 17% (95% CI = 12 to 22%), ranging from 6.7 to 26.1% (Fig. 1). The rate of malignancy among the pooled series of indeterminate thyroid nodules at high risk (Tir 3B) was 52% (95% CI = 46 to 58%), ranging from 42.4 and 57.8% (Fig. 2). The included studies were statistically non heterogeneous for sample and prevalence of cancers among nodules classified as Tir 3A (I-square 3.7%) and Tir 3B (I-square 0%). No significant publication bias was evident in these series: Egger’s test for Tir 3A = 2.95 (95% CI = −0.63 to 6.53, P = 0.084); Egger’s test for Tir 3B = 1.95 (95% CI = −4.81 to 0.92, P = 0.132).

Pooled prevalence of cancers in nodules cytologically classified as Tir 3A

Pooled prevalence of cancers in nodules cytologically classified as Tir 3B
Discussion
Here, we aimed to systematically review all published data on the prevalence of cancers in thyroid nodules with preoperative cytologic diagnosis of Tir 3A or Tir 3B according to ICCRTC [15]. Also, we attempted to meta-analyze the results of the included papers. Remarkably, the sample size and the prevalence of cancer in both categories were non-heterogeneous and no significant bias was identified. These data allow us to consider the recent results as strong. The systematic review retrieved six original papers with complete data of thyroid nodules operated upon after indeterminate FNA. The meta-analysis demonstrated that the subcategory Tir 3A had a lower cancer rate (17%) than Tir 3B (52%). This finding is encouraging for all users of Italian system for classification of thyroid cytologic samples in their clinical practice. In fact, this meta-analysis supports the actions suggested from the panel of ICCRTC, i.e., repeat FNA or clinical follow-up in presence of a Tir 3A cytologic report, and surgery in case of Tir 3B. We would like to underline that the present findings are quite different from that recorded in a meta-analysis on the reliability of Bethesda system in distinguishing low risk indeterminate lesions from high risk ones; there, the overall rate of malignancy was 27% for the Category III and 31% for the Category IV [18]. Then, no true difference was found between these two subcategories. Specifically, a preoperative Category III had a higher risk of malignancy than that one would expect. The herein demonstrated good performance of ICCRTC is probably due to the different interpretation of atypia which are features of its high risk subcategory (Tir 3B), while are included in the low risk of British (Thy 3a) and Bethesda (Category IV) systems. We advise for further prospective studies on this topic.
Some potential limitations of the present study have to be discussed. Generally, studies reporting positive findings are more likely to be published than those describing negative results. Also, small sample-size studies are likely to report positive relationship. Our study demonstrated lack of both significant publication bias and heterogeneity between the included studies. However, we retain that a selection bias might be present in this meta-analysis because these papers reported only selected series of patients undergone surgery (to obtain a histologic diagnosis of the indeterminate lesions) and it is not possible to evaluate outcome of all patients non-operated upon. Finally, the herein recorded malignancy rate of both Tir 3A and Tir 3B is higher than that expected [15]; conversely, in the document of ICCRTC the experts report clearly an estimation of risk based on their previous clinical experience.
In conclusion, Italian classification of thyroid cytologic samples can discriminate the indeterminate lesions at low risk of malignancy from that at high risk. This is mainly due to the fact that the Italian system, at variance with British and Bethesda ones, includes in the subcategory at high risk those cases with mild/focal nuclear atypia.
References
H. Gharib, E. Papini, R. Paschke, D.S. Duick, R. Valcavi, L. Hegedüs, P. Vitti, AACE/AME/ETA Task force on thyroid nodules. american association of clinical endocrinologists, associazione medici endocrinologi, and europeanthyroid association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr. Pract. 16, 1–43 (2010)
B.R. Haugen, E.K. Alexander, K.C. Bible, G.M. Doherty, S.J. Mandel, Y.E. Nikiforov, F. Pacini, G.W. Randolph, A.M. Sawka, M. Schlumberger, K.G. Schuff, S.I. Sherman, J.A. Sosa, D.L. Steward, R.M. Tuttle, L. Wartofsky, 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 26, 1–133(2016)
Z.W. Baloch, S. Fleisher, V.A. LiVolsi, P.K. Gupta, Diagnosis of “follicular neoplasm”: a gray zone in thyroid fine-needle aspiration cytology. Diagn. Cytopathol. 26, 41–44 (2002)
P. Trimboli, G. Treglia, L. Guidobaldi, E. Saggiorato, G. Nigri, A. Crescenzi, F. Romanelli, F. Orlandi, S. Valabrega, R. Sadeghi, L. Giovanella, Clinical characteristics as predictors of malignancy in patients with indeterminate thyroid cytology: a meta-analysis. Endocrine 46, 52–59 (2014)
P. Trimboli, E. Condorelli, A. Catania, S. Sorrenti, Clinical and ultrasound parameters in the approach to thyroid nodules cytologically classified as indeterminate neoplasm. Diagn. Cytopathol. 37, 783–785 (2009)
A. Heinzel, D. Müller, F.F. Behrendt, L. Giovanella, F.M. Mottaghy, F.A. Verburg, Thyroid nodules with indeterminate cytology: molecular imaging with 99mTc-methoxyisobutylisonitrile (MIBI) is more cost-effective than the Afirma gene expression classifier. Eur. J. Nucl. Med Mol. Imaging 41, 1497–1500 (2014)
L. Giovanella, L. Ceriani, G. Treglia, Role of isotope scan, including positron emission tomography/computed tomography, in nodular goitre. Best. Pract. Res Clin. Endocrinol. Metab. 28, 507–518 (2014)
A. Bartolazzi, F. Orlandi, E. Saggiorato, M. Volante, F. Arecco, R. Rossetto, N. Palestini, E. Ghigo, M. Papotti, G. Bussolati, M.P. Martegani, F. Pantellini, A. Carpi, M.R. Giovagnoli, S. Monti, V. Toscano, S. Sciacchitano, G.M. Pennelli, C. Mian, M.R. Pelizzo, M. Rugge, G. Troncone, L. Palombini, G. Chiappetta, G. Botti, A. Vecchione, R. Bellocco; Italian Thyroid Cancer Study Group (ITCSG), Galectin-3-expression analysis in the surgical selection of follicular thyroid nodules with indeterminate fine-needle aspiration cytology: a prospective multicentre study. Lancet Oncol. 9, 543–549 (2008)
P. Trimboli, G. Treglia, E. Condorelli, F. Romanelli, A. Crescenzi, M. Bongiovanni, L. Giovanella, BRAF mutated carcinomas among thyroid nodules with prior indeterminate FNA report: a systematic review and meta-analysis. Clin. Endocinol 84, 315–320 (2016)
P. Trimboli, G. Treglia, R. Sadeghi, F. Romanelli, L. Giovanella, Reliability of real-time elastography to diagnose thyroid nodules previously read at FNAC as indeterminate: a meta-analysis. Endocrine 50, 335–343 (2015)
P. Trimboli, A. Crescenzi, Thyroid core needle biopsy: taking stoke of the situation. Endocrine 48, 779–785 (2015)
E.K. Alexander, G.C. Kennedy, Z.W. Baloch, E.S. Cibas, D. Chudova, J. Diggans, L. Friedman, R.T. Kloos, V.A. LiVolsi, S.J. Mandel, S.S. Raab, J. Rosai, D.L. Steward, P.S. Walsh, J.I. Wilde, M.A. Zeiger, R.B. Lanman, B.R. Haugen, Preoperative diagnosis of benign thyroid nodules with indeterminate cytology. N. Engl. J. Med 367, 705–715 (2012)
P. Perros, K. Boelaert, S. Colley, C. Evans, R.M. Evans, G. Gerrard Ba, J. Gilbert, B. Harrison, S.J. Johnson, T.E. Giles, L. Moss, V. Lewington, K. Newbold, J. Taylor, R.V.Thakker, J. Watkinson, G.R.Williams British Thyroid Association Guidelines for the management of thyroid cancer. Clin. Endocrinol. 81, 1–122 (2014)
E.S. Cibas, S.Z. Ali, The bethesda system for reporting thyroid cytopathology. Thyroid 19, 1159–1165 (2009)
F. Nardi, F. Basolo, A. Crescenzi, G. Fadda, A. Frasoldati, F. Orlandi, L. Palombini, E. Papini, M. Zini, A. Pontecorvi, P. Vitti, Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Invest 37, 593–599 (2014)
A.A. Renshaw, Should “atypical follicular cells” in thyroid fine-needle aspirates be subclassified? Cancer Cytopathol. 118, 186–189 (2010)
P.A. Vanderlaan, E. Marqusee, J.F. Krane, Usefulness of diagnostic qualifiers for thyroid, fine-needle aspirations with atypia of undetermined significance. Am. J. Clin. Pathol. 136, 572–577 (2011)
P. Straccia, E.D. Rossi, T. Bizzarro, C. Brunelli, F. Cianfrini, D. Damiani, G. Fadda, A meta-analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated? Cancer Cytopathol. 123, 713–722 (2015)
R. DerSimonian, N. Laird, Meta-analysis in clinical trials. Control Clin. Trials 7, 177–188 (1986)
P. Trimboli, L. Guidobaldi, S. Amendola, N. Nasrollah, F. Romanelli, D. Attanasio, G. Ramacciato, E. Saggiorato, S. Valabrega, A. Crescenzi, Galectin-3 and HBME-1 improve the accuracy of core biopsy in indeterminate thyroid nodules. Endocrine 52, 39–45 (2016)
F. Tartaglia, A. Giuliani, L. Tromba, S. Carbotta, M. Karpathiotakis, G. Tortorelli, F. Pelle, R. Merola, C. Donello, G. Carbotta, L. De Anna, G. Conzo, S. Sorrenti, S. Ulisse, Fine needle aspiration cytology of 650 thyroid nodules operated for multinodular goiter: a cyto-histological correlation based on the new Italian cytological classification (siapec 2014). J. Biol. Regul. Homeost. Agents 30, 1187–1193 (2016)
G. Grani, L. Lamartina, V. Ascoli, D. Bosco, F. Nardi, F. D’Ambrosio, A. Rubini, L. Giacomelli, M. Biffoni, S. Filetti, C. Durante, V. Cantisani, Ultrasonography scoring systems can rule out malignancy in cytologically indeterminate thyroid nodules. Endocrine 57, 256–261 (2017)
F. Quaglino, V. Marchese, E. Mazza, C. Gottero, R. Lemini, S. Taraglio, When is thyroidectomy the right choice? comparison between fine-needle aspiration and final histology in a single institution experience. Eur. Thyroid J. 6, 94–100 (2017)
S. Ulisse, D. Bosco, F. Nardi, A. Nesca, E. D’Armiento, V. Guglielmino, C. De Vito, S. Sorrenti, D. Pironi, F. Tartaglia, S. Arcieri, A. Catania, M. Monti, A. Filippini, V. Ascoli, Thyroid imaging reporting and data system score combined with the new italian classification for thyroid cytology improves the clinical management of indeterminate nodules. Int J. Endocrinol. 2017, 9692304 (2017)
F. Medas, E. Erdas, L. Gordini, G. Conzo, C. Gambardella, G.L. Canu, G. Pisano, A. Nicolosi, P.G. Calò, Risk of malignancy in thyroid nodules classified as TIR-3A: What therapy? Int J. Surg. 41, S60–S64 (2017)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Trimboli, P., Crescenzi, A. & Giovanella, L. Performance of Italian Consensus for the Classification and Reporting of Thyroid Cytology (ICCRTC) in discriminating indeterminate lesions at low and high risk of malignancy. A systematic review and meta-analysis. Endocrine 60, 31–35 (2018). https://doi.org/10.1007/s12020-017-1382-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-017-1382-6