
Abstract
Metastatic differentiated thyroid carcinoma (DTC) with positive 131I scintigraphy, but negative stimulated Tg (sTg) is relatively rare in clinical practice. The clinical characteristics of these patients were analyzed in the current study. A total of 3367 consecutive histologically proven DTC patients were analyzed retrospectively from January 2007 to June 2013. Tg negativity was defined as a sTg level of <2 ng/mL without positive anti-Tg antibody (TgAb level of <100 IU/mL) under thyroid-stimulating hormone stimulation (TSH level of ≥30 mIU/L). Analyses were performed using the Statistical Package for the Social Sciences, version 20.0 (SPSS, Chicago, IL, USA). Seventy-one patients (median age 45 years, range 17–68 years) were post-therapeutic 131I-SPECT/CT positive and sTg negative (PTP-TN) constituting 2.1 % of all patients. Of these 71 patients, 2 (2.8 %) had bone metastasis, 11 (15.5 %) had lung metastasis, and 59 (83.1 %) had lymph node metastasis. Fifty-six patients had cervical lymph node metastasis (cLNM), and US was positive in 15 patients (26.8 %), while negative in 41 patients (73.2 %). When compared to patients with concordant positive results for sTg and 131I scintigraphy, US showed a relatively lower positive rate in the detection of cLNM in PTP-TN patients (28.8 vs. 53.8 %; χ 2 = 6.70; P = 0.01). In conclusion, even with sTg <2 ng/mL, there is a low risk of metastatic DTC. US had limitations in PTP-TN patients, while post-therapy 131I-SPECT/CT demonstrated an advantage in the detection of functioning metastasis despite low sTg levels in patients with metastatic DTC.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The conventional and effective treatment of differentiated thyroid carcinoma (DTC) in most patients consists of adequate surgical management followed by radioiodine (RAI) ablation and thyroid hormone suppression. Following 131I remnant ablation, the measurement of serum thyroglobulin (Tg) levels forms the basis of post-ablation follow-up, together with cervical ultrasound (US) [1, 2]. Stimulated serum Tg (sTg) level has a good prognostic value for persistent/recurrent disease after total thyroidectomy. A low sTg level has a high negative predictive value, whereas a high sTg level is frequently associated with persistent disease [3]. In addition, 131I-post-therapeutic whole-body planar scintigraphy (RxWBS), which is performed 3–7 days after the administration of high activity RAI in patients with DTC, is a standard procedure for RAI therapy and a useful tool for DTC patient staging [4].
As the mainstay in the follow-up of patients with DTC, reports of patients with a negative RxWBS and positive sTg are common. Reports of patients with positive 131I scintigraphy and negative sTg levels are relatively rare and all describe the results of 131I whole-body planar scintigraphy (131I-WBS) [5–7]. However, the lack of anatomical details visible on planar imaging and the superimposition of areas of increased RAI uptake present challenges with regard to accurate diagnosis and the localization of RAI-avid metastatic disease [8]. To date, the value of post-therapeutic 131I-SPECT/CT in these patients has not been reported.
Neck US, another main tool for the follow-up of DTC patients, is considered to be the most sensitive method for detecting cervical lymph node metastasis in DTC patients [9]. However, the positive rate of US in metastatic DTC patients with positive 131I scintigraphy and negative sTg levels has not been studied.
In the present study, 71 metastatic DTC patients were found to be false negative by serum sTg level but positive by post-therapeutic 131I-SPECT/CT. The clinical characteristics of these patients were investigated. And the positive rate of neck US in these patients with cervical lymph node metastasis was further studied.
Materials and methods
Patients
All patients withdrew thyroid hormone medication and began a low iodine diet 2–4 weeks before 131I therapy (thyroid-stimulating hormone [TSH] ≥ 30 mIU/L). The patients received oral 131I after obtaining conventional measurements, including free triiodothyronine (FT3), free thyroxine (FT4), TSH, Tg, anti-Tg antibody (TgAb), neck ultrasonography, and chest CT scan. An empirical treatment dose of 131I was administered (30-100 mCi for residual thyroid ablation, 150–200 mCi for metastatic disease).
Inclusion criteria
The inclusion criteria were (1) histologically proven DTC, (2) (near-) total thyroidectomy before 131I treatment, (3) sTg level <2 ng/mL and TgAb level <100 IU/mL, (4) TSH level ≥30 mIU/L after 2–4 weeks of levothyroxine withdrawal, and (5) post-therapeutic 131I-SPECT/CT diagnosed functioning metastatic disease.
Exclusion criteria
The exclusion criteria were (1) TgAb level ≥100 IU/mL or sTg level ≥2 ng/mL, (2) TSH level <30 mIU/L, (3) other types of thyroid carcinoma, and (4) no abnormal findings observed on131I scintigraphy.
Post-therapeutic 131I-WBS and SPECT/CT
131I-WBS and 131I-SPECT/CT fusion imaging were performed 3d after oral 131I. 131I whole-body planar images were obtained in both anterior and posterior projections using dual-head γ-cameras equipped with high-energy general-purpose collimators, at a table speed of 12 cm/min. SPECT/CT images were recorded using a Philips Precedence 16 (Philips, Medical Systems, The Netherlands), which consisted of a dual-detector γ-camera and an integrated 16-slice helical CT scanner. No contrast medium was administered during the procedure. CT data were used for attenuation correction and anatomic information. SPECT data were obtained on a dual-head camera in step-and-shoot mode, using a noncircular orbit, a 128 × 128 × 16 matrix, and 32 angles over a total of 180° (per detector); the acquisition time varied between 30 and 60 s per stop, depending on the counting rate. Reconstruction was performed on a Philips JETStream system using the Philips Astonish algorithm, providing transaxial, sagittal, and coronal slices of SPECT, CT, and fused SPECT/CT data.
Tg and anti-Tg antibody measurements
All patients had a serum TSH concentration of 30 mIU/L or more at the time of Tg and TgAb measurements following withdrawal of thyroid hormone replacement for 2–4 weeks. Tg and anti-Tg antibody measurements were obtained 1 day before the administration of 131I. TgAb was measured in all samples at the time of Tg determination. Serum Tg levels were determined in duplicate using electrochemiluminescence immunoassay kits (Roche Diagnostics GmbH, Mannheim, Germany), with a measurement range of 0.1000–1000 ng/mL. Serum TgAb levels were determined in duplicate using electrochemiluminescence immunoassay kits (Roche Diagnostics GmbH, Mannheim, Germany), with a measurement range of 10–4000 IU/mL.
Imaging interpretation
On RxWBS, abnormal findings were defined as any focal uptake above the surrounding background that was incompatible with obvious physiological activity or residual thyroid tissue. Uptake foci in the salivary glands and esophageal tract were considered physiological. Two nuclear medicine physicians jointly diagnosed the planar data and recorded the findings as normal or abnormal. SPECT/CT was then performed in patients with abnormal findings, for further evaluation. The SPECT/CT imaging features were classified as follows: 1, remnant tissue if the median/paramedian foci were localized either in the lower thyroid bed (usually posterolaterally to the trachea), in the upper thyroid bed or in the thyroglossal duct remnants; 2, lymph node metastasis (LNM) when a focus was localized in front of a round lesion congruent with a lymph node; 3, distant metastasis when focal iodine uptake was localized to bones or soft tissue organs in accordance with characteristic CT findings such as small lung nodules or lytic bone lesions. Ultrasonography examination of the entire neck was performed in all patients before 131I therapy with at least 2-4 weeks of levothyroxine withdrawal. The results of US examination of the neck were retrospectively evaluated. Tumor US findings were classified according to the nature, shape, echogenicity, margin, calcification, and vascularity [9, 10]. The presence of LNM was assessed using a four-point scale of the reviews’ confidence: 1, definitely absent; 2, probably absent; 3, probably present; 4, definitely present. For the purposes of positive and negative correlation, findings graded as 3 or 4 were considered positive; findings graded as 1 or 2 were considered negative for LNM.
Statistical analysis
Comparisons of continuous variables between two groups were performed using the Student’s t test. The Chi-square test was used for categorical variables. The Chi-square test was used to compare the US positive rate for detection of cervical lymph node metastasis between groups. All tests were two sided. A P value of <0.05 was considered statistically significant. All analyses were performed using the Statistical Package for the Social Sciences, version 20.0 (SPSS, Chicago, IL,USA).
Results
Clinical characteristics
Seventy-one of 3367 consecutive patients with histologically proven DTC (constituting 2.1 % of all patients) were post-therapeutic 131I-SPECT/CT positive and stimulated serum thyroglobulin negative (PTP-TN). The total number of all patients with negative stimulated serum Tg (with TgAb level of <100 IU/mL) was 604 and the percentage of patients who had negative stimulated serum Tg levels and positive post-therapy 131I-SPECT/CT scans of the total of all patients with negative stimulated serum Tg regardless of the outcome of the post-therapy scan is 11.7 %. Clinical data for these 71 patients were collected. The median age of the 71 patients was 45 years (range 17–68 years), with 36 subjects ≥45 years of age and 35 < 45 years. The female to male ratio was 2.55:1 with 51 women and 20 men. Sixty-six patients (93.0 %) had histologically proven PTC (2 had follicular variant PTC and one had columnar cell variant PTC) and 5 (7.0 %) had FTC. All 71 patients underwent (near-) total thyroidectomy before 131I treatment, and 59 (83.1 %) of these patients achieved (near-) total thyroidectomy after the first operation. The remaining 12 patients required two thyroid operations. They initially underwent thyroid lobectomies for primary DTC, but recurrence and/or metastatic lesions were detected during follow-up and complete thyroidectomies were performed before 131I treatment. The median time between the last thyroidectomy and the first positive 131I post-ablation scans was 3 months (range 0.5–23 months). Sixty-one (85.9 %) patients underwent neck dissection (central, central, and lateral neck dissection) including therapeutic or prophylactic procedures, while the remaining 10 patients (14.1 %) did not undergo neck dissection. Forty patients received 131I for residual thyroid ablation and the remaining 31 patients for the treatment of metastatic disease. Eighteen patients (25.4 %) had an undetectable sTg level (less than 0.1 ng/ml). Pathological T status was T1 in 25, T2 in 34, T3 in 8, and T4 in 4 patients. The clinical characteristics of these patients who were post-therapeutic 131I-SPECT/CT positive and stimulated serum thyroglobulin negative are shown in Table 1.
In order to determine the clinical characteristics of the PTP-TN patients, 71 patients with concordant positive results for sTg and 131I scintigraphy (PTP-TP, post-therapeutic 131I scintigraphy positive, and stimulated serum thyroglobulin positive) were randomly selected (groups-1, PTP-TP vs. PTP-TN). When compared to PTP-TP patients, PTP-TN patients were older (39 vs. 45 years, P = 0.04). In addition, the metastatic profile was significantly different (Fig. 1a, more patients with lymph node metastasis and fewer patients with lung and bone metastases in the PTP-TN group). All the patients with nodal involvement had only one focal uptake except two patients who had both mediastinal and cervical lymph node metastases with two focal uptakes. When compared the number of focal uptake revealed in patients with nodal involvement (focal uptake of the residual thyroid was excluded) between the two groups (Fig. 1c), the result demonstrated that all patients predominantly had one focal uptake and the small number of more than one focal uptake made the statistical differences that it cannot be calculated. No statistically significant differences in clinical characteristics were observed including gender (P = 0.112), the number of thyroid operations (P = 0.108), pathology of DTC (P = 0.546), pathological T status and N status (Table 2).

a Three site-associated categories were classified containing 2 (2.8 %) with bone metastasis (BM), 11 (15.5 %) with lung metastasis (LM), 59 (83.1 %) with lymph node metastasis (LNM). *P < 0.05; b the positive rate of cervical US between post-therapeutic 131I-SPECT/CT positive, while stimulated serum thyroglobulin-negative (PTP-TN) patients and post-therapeutic 131I-SPECT/CT positive and stimulated serum thyroglobulin positive (PTP-TP) patients. *P < 0.05; c number of focal uptake in PTP-TP and PTP-TN patients with node involvement (focal uptake of the residual thyroid was excluded)
Metastasis categories
All patients showed metastasis on 131I-SPECT/CT and three site-associated categories were determined, i.e., bone, lung, and lymph node. Of these 71 patients, 2 (2.8 %) had bone metastasis, 11 (15.5 %) had lung metastasis, and 59 (83.1 %) had lymph node metastasis.
Cervical LNM (cLNM) group
Among the 59 patients with lymph node metastasis, one had lung and cervical lymph node metastasis, two had both mediastinal and cervical lymph node metastases, three had only mediastinal lymph node metastasis, and 53 had only cervical lymph node metastasis. Of the 56 patients with cervical lymph node metastasis, US was positive in 15 patients (26.8 %) and negative in 41 patients (73.2 %). When 3 patients with parapharyngeal lymph node metastasis and 1 patient with paratracheal lymph node metastasis were excluded, US was positive in 15 patients (28.8 %) and negative in 37 patients (71.2 %).
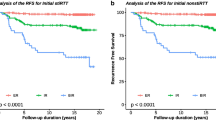
In order to investigate differences in the positive rate of US between PTP-TN patients and PTP-TP patients, 52 age- and sex-matched PTP-TP patients cervical lymph node metastases (parapharyngeal or paratracheal metastasis excluded) were identified (groups-2, PTP-TP vs. PTP-TN) (Table 3). Neck US was positive in 28 patients (53.8 %) and negative in 24 patients (46.2 %). These data demonstrated that compared to the PTP-TP group, US showed a relatively lower positive rate in the detection of cervical lymph node metastases in PTP-TN DTC patients (28.8 % vs. 53.8 %; χ 2 = 6.70; P = 0.01, Fig. 1b). Post-therapy 131I-SPECT/CT findings in two patients with cervical lymph node metastasis from the two subgroups are illustrated in Fig. 2.

Post-therapy 131I-SPECT/CT findings in patients with cervical lymph node metastasis. a (PTP-TN) A 45-year-old female papillary thyroid carcinoma patient received 100 mCi radioiodine after total thyroidectomy. Serum Tg, <0.1 ng/mL; TgAb, <10 IU/mL; TSH, >100 mIU/L). b (PTP-TP) A 43-year-old female papillary thyroid carcinoma patient received 100 mCi radioiodine after total thyroidectomy. Serum Tg, 106.4 ng/mL; TgAb, <10 IU/mL; TSH, >100 mIU/L)
Follow-up 131I therapy
No further 131I treatment was undertaken in 15 (21.1 %) of the 71 patients. These 15 patients did not accept further 131I therapy despite our recommendation. The remaining 56 patients (78.9 %) were followed up for a mean of 37 months (12–84 months) with regular 131I treatments (usually every 6 months; at least 100 mCi each time). During this period, metastatic uptake disappeared in 29 (51.8 %), was ameliorated in 16 (28.6 %), and persisted in 10 (17.9 %). One patient with bone metastases experienced progression. Diagnostic doses during 131I-WBS are not routinely recommended in our institution and none of these patients received diagnostic doses during 131I-WBS in the follow-up setting.
Discussion
Concordant results (undetectable or low level of sTg associated with negative 131I-WBS or elevated levels of sTg associated with positive 131I-WBS) are usually indicative of the absence or presence of disease. However, discordant results (elevated level of sTg with negative 131I-WBS or low levels of sTg with positive 131I-WBS) can also occur [11]. A low level of sTg with positive 131I scintigraphy is a relatively rare entity in clinical practice and it has been reported that 8.5 % of DTC patients show recurrences and metastases on RxWBS with a low sTg value [7]. The incidence rate in the current study is lower than that previously reported. Possible reasons for this could be as follows: (1) although all the patients recruited had histologically confirmed DTC and had undergone thyroidectomy before RAI therapy, bias in patient selection for RAI therapy in different countries could influence the incidence of this condition; (2) differences in the imaging modality (in this study SPECT/CT was used, while in previous research planar 131I whole body scan was used) could contribute to the different results observed; (3) also the short whole body scanning time could reduce the quality of your whole body scanning and detection of small and/or lower uptake foci which could be another potential bias.
131I-SPECT/CT is increasingly used to evaluate patients with DTC. Post-therapy scans with 131I-SPECT/CT improve detection and localization of 131I accumulation in lymph node metastases and distant metastases compared with planar WBS and reduce the number of equivocal diagnoses and the need for additional cross-sectional imaging [12]. It has been reported that integrated 131I-SPECT/CT imaging had an incremental diagnostic value compared with 131I-WBS in 47.6–88 % of cases and it was useful for distinguishing between benign and malignant lesions with a low confidence level in 131I-WBS [13].
Metastatic pattern in PTP-TN DTC patients was studied and three site-associated categories were determined, i.e., bone, lung and lymph node. Of 71 patients in the present study, 2 (2.8 %) had bone metastasis, 11 (15.5 %) had lung metastasis, and 59 (83.1 %) had lymph node metastasis. This metastatic profile is coincident with a previous study (the percentage of lymph node metastasis was 86.5 %) [7]. In patients with lymph node metastasis, all predominantly had one focal uptake. The number of focal uptake revealed in patients with nodal involvement was different between PTP-TN and PTP-TP patients but the the statistical differences cannot be calculated because of the small number of more than one focal uptake patients.
Recurrent and/or metastatic disease in DTC patients detected by 131I-SPECT/CT with no rise in sTg levels can occur due to different reasons. Several technical and methodological factors can cause false negative Tg determinations [14]. Reasons including small size of the tumor, unable to release detectable amounts of Tg, or loss of Tg secretion with preserved capability of 131I trapping have been reported [15–17]. Another explanation for low Tg levels in patients with persistent disease identified by scintigraphy is structural changes in Tg which can occur as an integral part of malignant transformation [17, 18]. Alterations of Tg structure may be based on reduced iodine content, and different amounts of several amino acids and monosaccharides as demonstrated by Kohno et al. who found that Tg in papillary adenocarcinomas differs from normal Tg [19].
With regard to the cut-off level of sTg and TgAb, we chose the stimulated serum Tg level of <2 ng/mLand a Tg Ab level of <100 IU/mL. According to the revised guidelines of the American Thyroid Association (ATA), the cut-off for sTg (2 ng/mL) chosen after thyroid hormone withdrawal is an appropriate tradeoff between sensitivity and specificity for the detection of recurrent disease. The positive cut-off of TgAb (100 IU/mL in the current study) chosen for evaluation of DTC patients is controversial. Previous studies have reported that the cut-off level for TgAb ranges from 30 to 100 IU/mL [7, 11]. Chung et al. reported that using a cut-off level of 100 IU/mL, the recurrence rate in TgAb-positive patients (Tg-undetectable) was significantly higher than that in TgAb-negative patients (49 vs. 3.4 %, P < 0.0001) [20]. However, some authors [21] consider that Tg measurements are not reliable in patients with detectable TgAbs, regardless of the level. In the current study, 12 patients (16.9 %) had undetectable serum TgAb.
Another interesting finding is the relatively low positive rate of US for the detection of cervical lymph node metastasis in PTP-TN DTC patients. As one of the main tools for the follow-up of DTC patients, neck US is the most sensitive method for detecting cLNM [1, 9] and the sonographic criteria for identifying cervical lymph node metastases are well established [22]. However, it is still difficult to differentiate recurrent tumors from non-recurrent lesions, such as postoperative granulation, suture granuloma and a benign lymph node, on ultrasound alone and the lower paratracheal, parapharyngeal, and retropharyngeal nodal chains are inadequately imaged with ultrasound [23]. According to our data, in DTC patients with low sTg levels and metastasis detected by 131I-SPECT/CT, neck US could not accurately differentiate between benign and malignant nodes. The reason for this could be that these metastatic nodes were too small to reach the metastatic criteria on ultrasonography. In these cases 131I-SPECT/CT was important in the diagnosis of recurrent and/or metastatic disease from DTC. Qiu et al. [24] also demonstrated that 131I-SPECT/CT could identify parapharyngeal metastasis from DTC at an early stage which could not be adequately imaged by other detectors.
Several limitations have to be mentioned in the current study. Only 11 of the 71 patients were confirmed to have metastases by pathology. The use of fine-needle aspiration biopsy of cervical and mediastinal lymph nodes may confirm the presence of metastasis. Without the results of fine-needle aspiration biopsy, it could be argued that a negative sTg level, as determined in the present study, is in fact a false-positive 131I-SPECT/CT finding. However, due to the nature of the imaging modality used in this study, 131I-SPECT/CT effectively excluded residual noncancerous thyroid tissue located outside the thyroid bed (substernal goiter or ectopic foci along the thyroglossal duct), physiologic uptake in non-thyroidal tissues, and contamination which might mimic uptake on WBS. In addition, 56 patients (78.9 %) were confirmed by repeated 131I positive uptake (although the 131I uptake gradually reduced, persistent positive uptake of 131I was re-identified by 131I-SPECT/CT after approximately 2–11 courses of 131I therapy during approximately 12–84 months follow-up). However, SPECT/CT imaging was only performed for specific areas such as suspicious foci detected on the planar image. This clinical application of SPECT/CT could result in missed opportunities for detecting additional occult lesions in patients with non-suspicious planar image findings. However, an undetectable or low level of sTg associated with a normal 131I-WBS is usually indicative of the absence of disease. The retrospective nature of the data in the present study may be another limitation.
In conclusion, 71 DTC patients (2.1 %) were found to have positive post-therapeutic 131I-SPECT/CT and negative sTg. When compared to PTP-TP patients, PTP-TN patients were older (39 vs. 45 years, P = 0.04).The metastatic sites in these patients were predominantly located in the cervical lymph nodes (78.9 %). The positive rate of US in the detection of cLNM in these patients was relatively low when compared to PTP-PT patients (28.8 vs. 53.8 %; χ 2 = 6.70; P = 0.01). Based on these findings, even with sTg <2 ng/mL, there is a low risk of metastatic thyroid carcinoma. US had limitations in PTP-TN patients, while post-therapy 131I-SPECT/CT had an advantage in the detection of functioning metastasis despite a low sTg level in patients with metastatic DTC.
References
D.S. Cooper, G.M. Doherty, B.R. Haugen, R.T. Kloos, S.L. Lee, S.J. Mandel, E.L. Mazzaferri, B. McIver, F. Pacini, M. Schlumberger, S.I. Sherman, D.L. Steward, R.M. Tuttle, Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19(11), 1167–1214 (2009). doi:10.1089/thy.2009.0110
C. Durante, G. Costante, S. Filetti, Differentiated thyroid carcinoma: defining new paradigms for postoperative management. Endocr. Relat. Cancer 20(4), R141–R154 (2013). doi:10.1530/erc-13-0066
J.I. Lee, Y.J. Chung, B.Y. Cho, S. Chong, J.W. Seok, S.J. Park, Postoperative-stimulated serum thyroglobulin measured at the time of 131I ablation is useful for the prediction of disease status in patients with differentiated thyroid carcinoma. Surgery 153(6), 828–835 (2013). doi:10.1016/j.surg.2012.12.008
F. Pacini, M. Schlumberger, H. Dralle, R. Elisei, J.W. Smit, W. Wiersinga, European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur. J. Endocrinol./Eur. Fed. Endocr. Soc. 154(6), 787–803 (2006). doi:10.1530/eje.1.02158
C. Nascimento, I. Borget, A. Al Ghuzlan, D. Deandreis, L. Chami, J.P. Travagli, D. Hartl, J. Lumbroso, C. Chougnet, L. Lacroix, E. Baudin, M. Schlumberger, S. Leboulleux, Persistent disease and recurrence in differentiated thyroid cancer patients with undetectable postoperative stimulated thyroglobulin level. Endocr. Relat. Cancer 18(2), R29–40 (2011). doi:10.1677/erc-10-0292
H.T. Phan, P.L. Jager, J.E. van der Wal, W.J. Sluiter, J.T. Plukker, R.A. Dierckx, B.H. Wolffenbuttel, T.P. Links, The follow-up of patients with differentiated thyroid cancer and undetectable thyroglobulin (Tg) and Tg antibodies during ablation. Eur. J. Endocrinol./Eur. Fed. Endocr. Soc. 158(1), 77–83 (2008). doi:10.1530/eje-07-0399
E.K. Park, J.K. Chung, I.H. Lim, J. Park do, D.S. Lee, M.C. Lee, B.Y. Cho, Recurrent/metastatic thyroid carcinomas false negative for serum thyroglobulin but positive by posttherapy I-131 whole body scans. Eur. J. Nucl. Med. Mol. Imaging 36(2), 172–179 (2009). doi:10.1007/s00259-008-0912-0
T. Leitha, A. Staudenherz, Frequency of diagnostic dilemmas in 131I whole body scanning. Nuklearmedizin 42(2), 55–62 (2003). doi:10.1267/nukl03020055
S.K. Kuna, I. Bracic, V. Tesic, K. Kuna, G.H. Herceg, D. Dodig, Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer. J. Ultrasound Med. 25(12), 1531–1537 (2006). quiz 1538–1540
A. Tschammler, G. Ott, T. Schang, B. Seelbach-Goebel, K. Schwager, D. Hahn, Lymphadenopathy: differentiation of benign from malignant disease–color Doppler US assessment of intranodal angioarchitecture. Radiology 208(1), 117–123 (1998). doi:10.1148/radiology.208.1.9646801
L. Montella, M. Caraglia, A. Abbruzzese, A. Soricelli, S.D. Prete, G. Squame, M. Salvatore, Molecular technology and the recombinant TSH have changed diagnostics of thyroid carcinoma with positive I-131 whole body scan but low serum thyroglobulin. Exp. Mol. Med. 36(3), 268–273 (2004). doi:10.1038/emm.2004.36
Y. Maruoka, K. Abe, S. Baba, T. Isoda, H. Sawamoto, Y. Tanabe, M. Sasaki, H. Honda, Incremental diagnostic value of SPECT/CT with 131I scintigraphy after radioiodine therapy in patients with well-differentiated thyroid carcinoma. Radiology 265(3), 902–909 (2012). doi:10.1148/radiol.12112108
Y.L. Xue, Z.L. Qiu, H.J. Song, Q.Y. Luo, Value of (1)(3)(1)I SPECT/CT for the evaluation of differentiated thyroid cancer: a systematic review of the literature. Eur. J. Nucl. Med. Mol. Imaging 40(5), 768–778 (2013). doi:10.1007/s00259-012-2310-x
C. Ma, A. Kuang, J. Xie, T. Ma, Possible explanations for patients with discordant findings of serum thyroglobulin and 131I whole-body scanning. J. Nucl. Med. 46(9), 1473–1480 (2005)
H.W. Muller-Gartner, C. Schneider, Clinical evaluation of tumor characteristics predisposing serum thyroglobulin to be undetectable in patients with differentiated thyroid cancer. Cancer 61(5), 976–981 (1988)
M. Franceschi, Z. Kusic, D. Franceschi, L. Lukinac, S. Roncevic, Thyroglobulin determination, neck ultrasonography and iodine-131 whole-body scintigraphy in differentiated thyroid carcinoma. J. Nucl. Med. 37(3), 446–451 (1996)
M.W. Ashcraft, A.J. Van Herle, The comparative value of serum thyroglobulin measurements and iodine 131 total body scans in the follow-up study of patients with treated differentiated thyroid cancer. Am. J. Med. 71(5), 806–814 (1981)
E.G. Black, A. Cassoni, T.M. Gimlette, C.L. Harmer, M.N. Maisey, G.D. Oates, R. Hoffenberg, Serum thyroglobulin in thyroid cancer. Lancet 2(8244), 443–445 (1981)
Y. Kohno, O. Tarutani, S. Sakata, H. Nakajima, Monoclonal antibodies to thyroglobulin elucidate differences in protein structure of thyroglobulin in healthy individuals and those with papillary adenocarcinoma. J. Clin. Endocrinol. Metab. 61(2), 343–350 (1985). doi:10.1210/jcem-61-2-343
J.K. Chung, Y.J. Park, T.Y. Kim, Y. So, S.K. Kim, D.J. Park, D.S. Lee, M.C. Lee, B.Y. Cho, Clinical significance of elevated level of serum antithyroglobulin antibody in patients with differentiated thyroid cancer after thyroid ablation. Clin. Endocrinol. 57(2), 215–221 (2002)
C.A. Spencer, Challenges of serum thyroglobulin (Tg) measurement in the presence of Tg autoantibodies. J. Clin. Endocrinol. Metab. 89(8), 3702–3704 (2004). doi:10.1210/jc.2004-0986
S. Leboulleux, E. Girard, M. Rose, J.P. Travagli, N. Sabbah, B. Caillou, D.M. Hartl, N. Lassau, E. Baudin, M. Schlumberger, Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 92(9), 3590–3594 (2007). doi:10.1210/jc.2007-0444
Y.L. Seo, D.Y. Yoon, S. Baek, Y.J. Ku, Y.S. Rho, E.J. Chung, S.H. Koh, Detection of neck recurrence in patients with differentiated thyroid cancer: comparison of ultrasound, contrast-enhanced CT and (18)F-FDG PET/CT using surgical pathology as a reference standard: (ultrasound vs. CT vs. (18)F-FDG PET/CT in recurrent thyroid cancer). Eur. Radiol. 22(10), 2246–2254 (2012). doi:10.1007/s00330-012-2470-x
Z.L. Qiu, Y.H. Xu, H.J. Song, Q.Y. Luo, Localization and identification of parapharyngeal metastases from differentiated thyroid carcinoma by 131I-SPECT/CT. Head Neck 33(2), 171–177 (2011). doi:10.1002/hed.21416
Conflict of interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
This study was sponsored by the National Natural Science Foundation of China (Nos. 81271611 & 81201115).
Author information
Authors and Affiliations
Corresponding author
Additional information
Chen-Tian Shen and Wei-Jun Wei have contributed equally to this work.
Rights and permissions
About this article

Cite this article
Shen, CT., Wei, WJ., Qiu, ZL. et al. Value of post-therapeutic 131I scintigraphy in stimulated serum thyroglobulin-negative patients with metastatic differentiated thyroid carcinoma. Endocrine 51, 283–290 (2016). https://doi.org/10.1007/s12020-015-0660-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-015-0660-4