
Abstract
The amyloid β-peptide theory of Alzheimer’s Disease has helped to advance our understanding of the disease tremendously. A new area of research focuses on the changes in neuronal network activity that take place and may contribute to the clinical and pathological picture of Alzheimer’s Disease. An apparent symptom of altered neuronal network activity in Alzheimer’s Disease is an increased frequency in epileptic seizures that is observed both in human patients and in mouse models of Alzheimer’s Disease. A root cause for altered network activity may be amyloid β itself by its ability to alter synaptic (glutamatergic) transmission and to impair the induction of long-term potentiation. It is on this aspect of Alzheimer’s Disease research that the current issue of NeuroMolecular Medicine will focus. Reviews will discuss the basic research and clinical aspects of the issue such as the effects of amyloid β on synaptic transmission and neuronal networks, as well as the changes in functional MRI activation patterns observed in early stages of Alzheimer’s Disease and the frequency and relevance of epileptic seizures in Alzheimer’s Disease patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
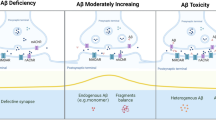
The amyloid β-peptide (Aβ) theory of Alzheimer’s Disease (AD) has proven invaluable for advancing our understanding of AD, and for the development of many therapeutic strategies including vaccination against Aβ, inhibition of amyloid precursor protein (APP) cleaving enzymes, glutaminyl cyclase inhibitors, and drugs targeting cholesterol synthesis or apoplipoprotein function. The Aβ theory of AD originated from the discovery that Aβ is the main constituent of amyloid plaques in the brains of AD patients, and was subsequently supported by genetic findings that linked gene mutations in the APP and Presenilin (PS) genes to increased Aβ production. In the last decade, the Aβ theory of AD subtly shifted its emphasis away from amyloid plaques which, although most likely detrimental to brain tissue (Meyer-Luehmann et al. 2008), are not necessarily regarded as the root cause of cognitive decline. Rather the emphasis has turned to soluble Aβ oligomers or fibrils, which have been shown to have an inhibitory influence on synaptic transmission and can reduce the number of synapses in experimental models (Kamenetz et al. 2003). The debate about which specific form of Aβ transmits these effects is still ongoing. For example, Aβ dimers isolated from brain extracts from AD patients were found to have these inhibitory properties (Shankar et al. 2008), whereas with synthetic peptides Aβ oligomers of at least 100 molecules were needed to exert similar effects (Laurén et al. 2009). While the final word is still out on this matter, the change in focus from amyloid plaques to Aβ oligomers has advanced our knowledge in several ways. First, there is evidence for a possible physiological function for soluble Aβ, serving as a negative feedback mechanism in synaptic transmission that protects neurons from overexcitation. Accordingly, Aβ generation has been shown to increase in depolarized neurons. Second, soluble Aβ provides a direct link to synaptic transmission, the basis of all information processing in the brain. Therefore, the soluble Aβ theory of AD also provides a rationale for how in early stages of AD neuronal information processing may be affected without neuron loss or significant structural brain damage.
The pathogenesis of AD, however, may be much more complex than a simple increase in levels of Aβ and, indeed, many elderly individuals exhibit extensive Aβ plaque pathology with no major impairment of cognitive function (Forman et al. 2007). While neurofibrillary tangles are better correlated with cognitive impairment, some individuals may also have relatively high numbers of neurofibrillary tangles and yet maintain normal cognitive function. Moreover, recent studies of animal models of AD and tauopathies have shown that cognitive performance can be improved without lessening of Aβ or tau pathology (Halagappa et al. 2007). Aging is the major risk factor for the most common late-onset cases of AD, and so it is not surprising that links have been discerned between the molecular mechanisms of normal aging and AD. Three age-related changes that are relevant to perturbed network activity are: (1) increased oxidative damage to cellular proteins, membranes, and nucleic acids (Mattson 2004a, b; Markesbery and Lovell 2007); (2) reduced neurotrophic factor signaling (Zuccato and Cattaneo 2009); and (3) dysregulation of neuronal calcium homeostasis (Bezprozvanny and Mattson 2008). Oxidative stress can affect neuronal excitability by inhibiting ion-motive ATPases, modifying ligand- and voltage-gated ion channels and altering neurotransmitter signaling pathways. Neurotrophic factors, particularly BDNF, have been shown to affect network excitability and play pivotal roles in cognitive processes. Aβ, oxidative stress, and altered neurotrophic factor signaling can perturb calcium homeostasis and, on the other hand, aberrant calcium signaling can alter APP processing, can promote oxidative stress, and can impair neurotrophic signaling. Intuitively, it seems likely that some of the earliest abnormalities that occur in AD are subtle alterations in neurotransmitter and neurotrophic factor signaling associated with increased oxidative stress and perturbed cellular calcium homeostasis.
A next logical step is to move from the level of individual synapses and neuron to a higher level of organization and study how neuronal network function is altered in AD. It is on this aspect that the current issue of NeuroMolecular Medicine will focus, discussing some of the more recent exciting findings. As has been pointed out previously (Palop et al. 2006; Mesulam 2000), a sustained alteration of synaptic transmission is likely to elicit compensatory responses in the brain. Some of these compensatory responses may be beneficial and others may be detrimental to cognitive function or neuronal survival and, moreover, the responses may occur in both short- and long-term time periods. Short-term adaptive responses of neuronal network activity are possible explanation for the remarkable day to day fluctuations typically seen in AD patients (Palop et al. 2006, Palop and Mucke 2009), which cannot be explained through structural changes in the brain. In any case, the compensatory responses, which can be considered indirect effects of Aβ, are likely to become part of the overall clinical picture in more advanced stages of the disease. A clear understanding of these compensatory responses should help us understand endogenous processes that help the brain cope with increased levels of Aβ and oxidative stress to keep synaptic transmission working despite impaired synaptic drive. Having a closer look at neuronal adaptive responses to aging and increased Aβ levels also will likely help us understand some of the apparent discrepancies that have emerged. For example, despite the inhibitory effect of Aβ on synaptic transmission in slice culture experiments, several mouse models of AD exhibit epileptic seizures, in part before the onset of plaque deposition and memory deficits (LaFerla et al. 1995; Moechars et al. 1999; Kumar-Singh et al. 2000; Lalonde et al. 2005). This increased excitability may contribute to cognitive dysfunction because hippocampal epileptiform discharges can also occur without any observable seizure activity in mice (Palop et al. 2007).
Another open question is: how might alterations in neuronal network activity contribute to increased production and/or reduced clearance of Aβ in AD? Aβ production can be increased by neuronal depolarization and intriguingly Aβ deposition is increased in areas of the “default network”, i.e., brain regions that are active in restive state and are silenced during learning and memory tasks (Sperling et al. 2009). Importantly, in patients with minimal cognitive impairment and MCI patients, the default network remains active during learning and memory tasks (Sperling et al. 2009).
Exposure of neurons to Aβ peptide in culture and in vivo causes an increased intracellular calcium concentration (Mattson et al. 1992; Kuchibhotla et al. 2008). One possible explanation would be that the primary action of Aβ is inhibition of synaptic transmission and that an adaptive response in neurons then causes an increase in cytosolic calcium, which will then render the neurons more susceptible to epileptic discharges and excitotoxicity. A variation of this hypothesis would be that Aβ primarily inhibits N-methyl d-aspartate (NMDA) receptor mediated currents and that a compensatory increase in AMPA/kainate receptor currents then leads to increased vulnerability to seizures (Moechars et al. 1999). Of course, the reverse may be the case as well, i.e., that the primary action of Aβ is to increase excitability and compensatory responses then inhibit the strength of synaptic transmission. These points underscore that much more work remains to be done to establish the sequence of events underlying neuronal network dysfunction in AD, and the role of Aβ in those events.
In this issue of NeuroMolecular Medicine, Lennart Mucke and Jorge Palop discuss the latest developments and insights in the area of neuronal network activity in AD, the molecular mechanism that may underlie altered network activity and how mouse models of AD can be used to unravel the effects that Aβ has at the molecular, synaptic, and network level. Andrew Larner considers the clinical side of the issue reviewing the current knowledge about epileptic seizures in AD patients. It has been known for a long time that epileptic seizure frequency is increased in AD patients, but it has until recently been considered to be a late stage epiphenomenon. And while it is unlikely that seizures precede the clinical onset of AD in patients as clearly as in some mice models, more recent studies have shown that seizures in fact can occur fairly early in the course of the disease. A greater knowledge about seizure type and origin may help us understand if and how subclinical seizures can have an impact on cognitive function in AD patients.
Michael Rowan provides an oversight about how Aβ alters glutamatergic synaptic transmission and how neuronal activity and cholinergic transmission interact with the effects of Aβ.
While Aβ production seems to be a fairly straightforward process involving two proteases (β- and γ-secretases), APP processing in fact is a quite intricate and complex procedure that can be considered a miniature network that is likely to have multiple sites of feedback regulation. More functions have evolved for most of APP’s cleavage products in addition to Aβ including secreted forms of APP (sAPPα and sAPPβ) and intracellular C-terminal domains including AICD (Furukawa et al. 1996; Mattson 2004a, b). In addition, more substrates have been discovered for APP processing enzymes. Reducing Aβ formation through inhibition of APP processing enzymes therefore is likely to affect non-APP substrate cleaving and possibly also inhibit the functions of non-Aβ fragments of APP, making the search for suitable yet potent β- and γ-secretase inhibitors a formidable task. Vivian Chow and Philip Wong together with the authors of this article review this aspect of AD.
Stress can be considered a modulator of brain network activity and Sarah Rothman and Mark Mattson review the evidence that suggests a link between stress and AD.
Mouse models of AD replicate only specific aspects of the disease, which in most cases is increased Aβ production and deposition in plaques. They lack neurofibrillary tangles unless a mutation in the microtubule associated protein tau is introduced in addition to APP and PS1 mutations, as in the so-called triple transgenic AD mice (Oddo et al. 2003b). While these triple transgenic mice have proven very useful in addressing some of the basic questions regarding Aβ and tau pathologies (Oddo et al. 2003a, 2006, 2007, 2008a, b) one must keep in mind that in sporadic AD no mutations are observed in the tau gene and tau mutations alone will cause neurofibrillary tangles without plaques. So it remains to be seen whether the same interactions between Aβ and tau that are observed in the triple transgenic mice actually take place in sporadic AD patients. Similarly, it has to be taken into account that the PS1 mutations used for most mouse models of AD increase neuronal cytosolic calcium via release from the endoplasmic reticulum (Guo et al. 1997; Chan et al. 2000; Tu et al. 2006; Nelson et al. 2007; Cheung et al. 2008), causing severe calcium dysregulation (Lopez et al. 2008) that is possibly independent of the γ-secretase activity of PS1. This is another aspect of AD mouse models that is unlikely to appear in this form in sporadic AD. Also aging is the single most powerful risk factor for developing AD. However, aging induced changes in the human brain are somewhat different (and arguably more severe) from those observed in mice (Loerch et al. 2008). Accordingly, studying AD mouse models can only provide an addition but no substitute for studying AD patients. In addition to neuropathological studies with brain tissue, the emergence of functional MRI and advanced software analysis now allows us to study neuronal network interactions in human brains. Reisa Sperling introduces us to this technique and reviews some of the findings from AD patients. These studies are likely to provide us with clues about the effect of AD on neuronal network activity and how network activity in AD patients may shape the disease. Ultimately the challenge will be to reconcile and integrate the findings from basic research at single synapse level with functional MRI and clinical data. We hope that this issue of NeuroMolecular Medicine provides some food for thought for our readers toward this goal.
References
Bezprozvanny, I., & Mattson, M. P. (2008). Neuronal calcium mishandling and the pathogenesis of Alzheimer’s disease. Trends in Neurosciences, 31, 454–463.
Chan, S. L., Mayne, M., Holden, C. P., Geiger, J. D., & Mattson, M. P. (2000). Presenilin-1 mutations increase levels of ryanodine receptors and calcium release in PC12 cells and cortical neurons. Journal of Biological Chemistry, 275, 18195–18200.
Cheung, K. H., Shineman, D., Müller, M., Cárdenas, C., Mei, L., Yang, J., et al. (2008). Mechanism of Ca2+ disruption in Alzheimer’s disease by presenilin regulation of InsP3 receptor channel gating. Neuron, 58, 871–883.
Forman, M. S., Mufson, E. J., Leurgans, S., Pratico, D., Joyce, S., Leight, S., et al. (2007). Cortical biochemistry in MCI and Alzheimer disease: Lack of correlation with clinical diagnosis. Neurology, 68, 757–763.
Furukawa, K., Barger, S. W., Blalock, E. M., & Mattson, M. P. (1996). Activation of K+ channels and suppression of neuronal activity by secreted beta-amyloid-precursor protein. Nature, 379, 74–78.
Guo, Q., Sopher, B. L., Furukawa, K., Pham, D. G., Robinson, N., Martin, G. M., et al. (1997). Alzheimer’s presenilin mutation sensitizes neural cells to apoptosis induced by trophic factor withdrawal and amyloid beta-peptide: involvement of calcium and oxyradicals. Journal of Neuroscience, 17, 4212–4222.
Halagappa, V. K., Guo, Z., Pearson, M., Matsuoka, Y., Cutler, R. G., Laferla, F. M., et al. (2007). Intermittent fasting and caloric restriction ameliorate age-related behavioral deficits in the triple-transgenic mouse model of Alzheimer’s disease. Neurobiology of Diseases, 26, 212–220.
Kamenetz, F., Tomita, T., Hsieh, H., Seabrook, G., Borchelt, D., Iwatsubo, T., et al. (2003). APP processing and synaptic function. Neuron, 37, 925–937.
Kuchibhotla, K. V., Goldman, S. T., Lattarulo, C. R., Wu, H. Y., Hyman, B. T., & Bacskai, B. J. (2008). Abeta plaques lead to aberrant regulation of calcium homeostasis in vivo resulting in structural and functional disruption of neuronal networks. Neuron, 59, 214–225.
Kumar-Singh, S., Dewachter, I., Moechars, D., Lübke, U., De Jonghe, C., Ceuterick, C., et al. (2000). Behavioral disturbances without amyloid deposits in mice overexpressing human amyloid precursor protein with Flemish (A692G) or Dutch (E693Q) mutation. Neurobiology of Diseases, 7, 9–22.
LaFerla, F. M., Tinkle, B. T., Bieberich, C. J., Haudenschild, C. C., & Jay, G. (1995). The Alzheimer’s A beta peptide induces neurodegeneration and apoptotic cell death in transgenic mice. Nature Genetics, 9, 21–30.
Lalonde, R., Dumont, M., Staufenbiel, M., & Strazielle, C. (2005). Neurobehavioral characterization of APP23 transgenic mice with the SHIRPA primary screen. Behavioural Brain Research, 157, 91–98.
Laurén, J., Gimbel, D. A., Nygaard, H. B., Gilbert, J. W., & Strittmatter, S. M. (2009). Cellular prion protein mediates impairment of synaptic plasticity by amyloid-beta oligomers. Nature, 457, 1128–1132.
Loerch, P. M., Lu, T., Dakin, K. A., Vann, J. M., Isaacs, A., Geula, C., et al. (2008). Evolution of the aging brain transcriptome and synaptic regulation. PLoS One, 3, e3329.
Lopez, J. R., Lyckman, A., Oddo, S., Laferla, F. M., Querfurth, H. W., & Shtifman, A. (2008). Increased intraneuronal resting [Ca2+] in adult Alzheimer’s disease mice. Journal of Neurochemistry, 105, 262–271.
Markesbery, W. R., & Lovell, M. A. (2007). Damage to lipids, proteins, DNA, and RNA in mild cognitive impairment. Archives of Neurology, 64, 954–956.
Mattson, M. P. (2004a). Pathways towards and away from Alzheimer’s disease. Nature, 430, 631–639.
Mattson, M. P. (2004b). Metal-catalyzed disruption of membrane protein and lipid signaling in the pathogenesis of neurodegenerative disorders. Annals of the New York Academy of Sciences, 1012, 37–50.
Mattson, M. P., Cheng, B., Davis, D., Bryant, K., Lieberburg, I., & Rydel, R. E. (1992). beta-Amyloid peptides destabilize calcium homeostasis and render human cortical neurons vulnerable to excitotoxicity. Journal of Neuroscience, 12, 376–389.
Mesulam, M. M. (2000). A plasticity-based theory of the pathogenesis of Alzheimer’s disease. Annals of the New York Academy of Sciences, 924, 42–52.
Meyer-Luehmann, M., Spires-Jones, T. L., Prada, C., Garcia-Alloza, M., de Calignon, A., Rozkalne, A., et al. (2008). Rapid appearance and local toxicity of amyloid-beta plaques in a mouse model of Alzheimer’s disease. Nature, 451, 720–724.
Moechars, D., Lorent, K., & Van Leuven, F. (1999). Premature death in transgenic mice that overexpress a mutant amyloid precursor protein is preceded by severe neurodegeneration and apoptosis. Neuroscience, 91, 819–830.
Nelson, O., Tu, H., Lei, T., Bentahir, M., de Strooper, B., & Bezprozvanny, I. (2007). Familial Alzheimer disease-linked mutations specifically disrupt Ca2+ leak function of presenilin 1. Journal of Clinical Investigation, 117, 1230–1239.
Oddo, S., Caccamo, A., Cheng, D., Jouleh, B., Torp, R., & LaFerla, F. M. (2007). Genetically augmenting tau levels does not modulate the onset or progression of Abeta pathology in transgenic mice. Journal of Neurochemistry, 102, 1053–1063.
Oddo, S., Caccamo, A., Cheng, D., & Laferla, F. M. (2008a). Genetically altering Abeta distribution from the brain to the vasculature ameliorates tau pathology. Brain Pathology, 19, 421–430.
Oddo, S., Caccamo, A., Kitazawa, M., Tseng, B. P., & LaFerla, F. M. (2003a). Amyloid deposition precedes tangle formation in a triple transgenic model of Alzheimer’s disease. Neurobiology of Aging, 24, 1063–1070.
Oddo, S., Caccamo, A., Shepherd, J. D., Murphy, M. P., Golde, T. E., Kayed, R., et al. (2003b). Triple-transgenic model of Alzheimer’s disease with plaques and tangles: Intracellular Abeta and synaptic dysfunction. Neuron, 39, 409–421.
Oddo, S., Caccamo, A., Tran, L., Lambert, M. P., Glabe, C. G., Klein, W. L., et al. (2006). Temporal profile of amyloid-beta (Abeta) oligomerization in an in vivo model of Alzheimer disease. A link between Abeta and tau pathology. Journal of Biological Chemistry, 281, 1599–1604.
Oddo, S., Caccamo, A., Tseng, B., Cheng, D., Vasilevko, V., Cribbs, D. H., et al. (2008b). Blocking Abeta42 accumulation delays the onset and progression of tau pathology via the C terminus of heat shock protein70-interacting protein: a mechanistic link between Abeta and tau pathology. Journal of Neuroscience, 28, 12163–12175.
Palop, J. J., Chin, J., & Mucke, L. (2006). A network dysfunction perspective on neurodegenerative diseases. Nature, 443, 768–773.
Palop, J. J., Chin, J., Roberson, E. D., Wang, J., Thwin, M. T., Bien-Ly, N., et al. (2007). Aberrant excitatory neuronal activity and compensatory remodeling of inhibitory hippocampal circuits in mouse models of Alzheimer’s disease. Neuron, 55, 697–711.
Palop, J. J., & Mucke, L. (2009). Epilepsy and cognitive impairments in Alzheimer disease. Archives of Neurology, 66, 435–440.
Shankar, G. M., Li, S., Mehta, T. H., Garcia-Munoz, A., Shepardson, N. E., Smith, I., et al. (2008). Amyloid-beta protein dimers isolated directly from Alzheimer’s brains impair synaptic plasticity and memory. Nature Medicine, 14, 837–842.
Sperling, R. A., Laviolette, P. S., O’Keefe, K., O’Brien, J., Rentz, D. M., Pihlajamaki, M., et al. (2009). Amyloid deposition is associated with impaired default network function in older persons without dementia. Neuron, 63, 178–188.
Tu, H., Nelson, O., Bezprozvanny, A., Wang, Z., Lee, S. F., Hao, Y. H., et al. (2006). Presenilins form ER Ca2+ leak channels, a function disrupted by familial Alzheimer’s disease-linked mutations. Cell, 126, 981–993.
Zuccato, C., & Cattaneo, E. (2009). Brain-derived neurotrophic factor in neurodegenerative diseases. Nature Reviews: Neurology, 5, 311–322.
Acknowledgments
This work was supported by the Intramural Research Program of the NIH, National Institute on Aging.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gleichmann, M., Mattson, M.P. Alzheimer’s Disease and Neuronal Network Activity. Neuromol Med 12, 44–47 (2010). https://doi.org/10.1007/s12017-009-8100-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12017-009-8100-3