
Abstract
Amyloid plaques are composed primarily of amyloid-beta (Aβ) peptides derived from proteolytic cleavage of amyloid precursor protein (APP) and are considered to play a pivotal role in Alzheimer’s disease (AD) pathogenesis. Presently, AD is diagnosed after the onset of clinical manifestations. With the arrival of novel therapeutic agents for treatment of AD, there is an urgent need for biomarkers to detect early stages of AD. Measurement of plasma Aβ has been suggested as an inexpensive and non-invasive tool to diagnose AD and to monitor Aβ modifying therapies. However, the majority of cross-sectional studies on plasma Aβ levels in humans have not shown differences between individuals with AD compared to controls. Similarly, cross-sectional studies of mouse plasma Aβ have yielded inconsistent trends in different mouse models. However, longitudinal studies appear to be more promising in humans. Recently, efforts to modify plasma Aβ levels using modulators have shown some promise. In this review, we will summarize the present data on plasma Aβ in humans and mouse models of AD. We will discuss the potential of modulators of Aβ levels in plasma, including antibodies and insulin, and the challenges associated with measuring plasma Aβ. Modulators of plasma Aβ may provide an important tool to optimize plasma Aβ levels and may improve the diagnostic potential of this approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The pathological hallmarks of Alzheimer’s disease (AD) are amyloid plaques, neurofibrillary tangles, synaptic degeneration, and neuronal loss (Price and Sisodia 1998). Amyloid plaques are composed of amyloid-beta (Aβ) 42 and 40 peptides derived from the proteolytic cleavage of amyloid precursor protein (APP) by β-site APP cleavage enzyme 1 (BACE1) (Sinha et al. 1999; Vassar et al. 1999) and the γ-secretase (De Strooper 2003). The endosome and the endocytic pathway have been proposed as possible sites for the β and γ cleavage of APP (Small and Gandy 2006), and the resulting Aβ peptides are secreted by both neuronal and non-neuronal cells (Selkoe 1997, 2002). Recently, soluble forms of Aβ have been implicated in neurotoxicity (Lambert et al. 1998; Walsh et al. 2002; Lesne et al. 2006), and may correlate better with cognition than amyloid plaque burden (Lue et al. 1999; McLean et al. 1999).
The clinical manifestations of AD, i.e. cognitive decline and neuro-behavioral changes, are preceded by a long preclinical stage characterized by the silent development of neuropathological lesions (Crystal et al. 1988; Katzman et al. 1988; Troncoso et al. 1996; Price and Morris 1999; Schmitt et al. 2000; Morris and Price 2001). These preclinical and early stages of AD represent the ideal time to treat the disease (Neugroschl and Davis 2002) with newly emerging approaches such as gamma-secretase inhibitors (Siemers et al. 2006, 2007) or immunotherapy (Hock et al. 2003).
As Aβ is considered to play an early and pivotal role in AD pathogenesis (Hardy and Selkoe 2002), it may be a useful tool in diagnosing AD in the preclinical/early stages, as well as for monitoring potential Aβ modifying therapies (Galasko 2005). While human CSF Aβ levels have mostly shown reduction with disease progression (Jensen et al. 1999), much of the data on plasma Aβ levels have been equivocal (Irizarry 2004). However, since plasma Aβ would be less invasive and more accessible than CSF Aβ as a biomarker, many strategies are under investigation to optimize plasma Aβ as a predictor of AD as well as to monitor the efficacy of Aβ modifying agents.
In this article, we will review studies involving plasma Aβ levels in humans as well as in transgenic (tg) mouse models of AD. Further, we will discuss the challenges that arise in measuring plasma Aβ levels as well as ways to optimize the detection of Aβ in plasma.
Plasma Aβ Levels
Human
While the data on human cerebrospinal fluid (CSF) mostly show decreased Aβ levels correlating with diagnosis and disease progression of AD (Jensen et al. 1999; Sunderland et al. 2003), much of the data on human plasma Aβ remain unclear. Studies have shown that subjects who exhibit overproduction of Aβ such as individuals with familial forms of AD and Down’s syndrome have higher plasma Aβ levels compared to controls (Scheuner et al. 1996; Tokuda et al. 1997; Iwatsubo 1998). However, only 5–10% of the AD cases are familial (Goate et al. 1991; Levy-Lahad et al. 1995; Sherrington et al. 1995) and the remaining cases are mostly sporadic (sAD) and late-onset AD (LOAD). While Aβ production is thought to be increased in FAD (Selkoe 2001), sAD is thought to be caused by the imbalance between Aβ production and clearance (Selkoe 2001; Hardy and Selkoe 2002). Many of the cross-sectional studies examining sAD subjects have not shown significant difference in the plasma Aβ levels compared to cognitively normal controls or controls with other neurological diseases (Table 1).
There may be several reasons why the data on plasma Aβ levels in sAD subjects are less consistent compared to CSF Aβ levels. Direct communication between the brain interstitial fluid (ISF) and CSF (Silverberg et al. 2003) may allow the Aβ level in the brain ISF to be closely reflected in the CSF. It is thought that decreasing CSF Aβ levels with progression of AD is a reflection of increasing Aβ deposition into insoluble plaques in the brain, as well as decreasing numbers of neurons that are able to produce Aβ in the brain (Jensen et al. 1999). In plasma, interpretation of the Aβ level is more complex. In addition to variability found with age and disease severity (Giedraitis et al. 2007), there are other factors that come into play. One of the factors is the origin of Aβ in the plasma. There is evidence to suggest that most of the Aβ production occurs in the brain (Laird et al. 2005), however, the possibility of Aβ derived from other sources must be considered. Proteolytic processing of APP by BACE1 leads to the formation of Aβ. BACE1 activity can be found at very high levels in the AD brain (Holsinger et al. 2002; Yang et al. 2003), but is also present at lower levels in peripheral organs such as skeletal muscle, liver, kidney, and lung (Sinha et al. 1999; Vassar et al. 1999) Aβ peptides have also been detected in skin, subcutaneous tissue, and intestine (Joachim et al. 1989) as well as in muscle (Kuo et al. 2000b). Although the formation of Aβ species may be higher in the brain compared to other organs, it is possible that production of Aβ in large peripheral organs such as skeletal muscles which comprises approximately 25% of the body weight in humans may result in a significant contribution to the plasma Aβ pool (Kuo et al. 2000b). Platelets are another source of Aβ, albeit mostly Aβ40 (Bush et al. 1990; Chen et al. 1995; Evin et al. 2003). Detection of lower Aβ levels (1:2) in the ventricular CSF samples compared to the spinal CSF samples also suggest contribution of Aβ from periphery (de Leon et al. 2004).
Another factor that may confound the detection of Aβ is the transporter-dependent movement of Aβ into and from the brain. Animal data suggest that approximately 10% of Aβ from the brain interstitial fluid (ISF) moves into blood stream via ISF bulk flow (Shibata et al. 2000). However, most of the movement of Aβ is thought to be dependent on transporters such as low-density lipoprotein receptor-related protein-1 (LRP-1) (Deane et al. 2004; Shibata et al. 2000) and receptor for advanced glycation end products (RAGE) (Deane et al. 2003) due to the presence of tight endothelial cell junctions at the blood–brain barrier (BBB) (Begley and Brightman 2003). Taken together, these reasons may explain the difficulty in establishing a direct correlation between plasma Aβ and CSF Aβ levels (Vanderstichele et al. 2000; Mehta et al. 2001; Giedraitis et al. 2007; Matsumoto et al. 2007). Further, these factors may explain why plasma Aβ levels do not correlate well with brain Aβ levels at autopsy (Freeman et al. 2007) or in vivo imaging by PIB compound (Fagan et al. 2006) in AD cases.
One interesting finding observed in several of these studies is the effect of aging on plasma Aβ levels in humans (Matsubara et al. 1999; Mayeux et al. 1999, 2003; Fukumoto et al. 2003; Ertekin-Taner et al. 2008; Sundelof et al. 2008). Specifically, increase in age alone correlated with increase in plasma Aβ levels in some studies. This was demonstrated in cognitively normal adults (Matsubara et al. 1999) as well as in sAD/MCI and other neurological controls (Fukumoto et al. 2003). This increase may be due to aging related changes. Tamaki et al. demonstrated decreased levels of hepatic LRP-1 with concomitant decrease in hepatic Aβ40 uptake in aged versus young rats (Tamaki et al. 2006). If the same holds true for humans, decreased peripheral uptake and clearance of Aβ in the liver may be contributing to the increase in plasma Aβ levels in older adults.
The effects of aging also complicate the interpretation of plasma Aβ levels. It is possible that the gradual decrease in plasma Aβ levels in the AD group may eventually fall to the same range as the normal controls whose plasma Aβ levels increase in an age-dependent manner (Golde et al. 2000). This may explain why much of the plasma Aβ data in cross-sectional studies do not show significant differences between sAD and controls. The longitudinal studies seem more promising, with some studies showing initially elevated Aβ42 levels in those that eventually develop AD (Mayeux et al. 1999, 2003). Most show that subjects who manifest sAD within the time frame of the study start with higher plasma Aβ42 levels, and the Aβ42/Aβ40 ratios also appear to be significantly different from those who remain asymptomatic, albeit different patterns that have been observed in different studies (Table 1) (Mayeux et al. 1999; Graff-Radford et al. 2007). It may also be important to understand the genetics of sAD in order to correctly interpret plasma Aβ levels, as plasma Aβ42 was shown to be elevated in the extended family members of some of the subjects with sAD or LOAD (Ertekin-Taner et al. 2001, 2008).
Recently, different studies have investigated the time-dependent variability of Aβ levels in CSF. One study has shown that CSF Aβ levels are thought to have significant variability (1.5- to 4-fold) over 12–36 h, and that they may be dependent on the time of day or activity (Bateman et al. 2007), while other studies have shown that they are stable up to an average of 10–18 months of follow up (Kanai et al. 1998; Andreasen et al. 1999). Plasma Aβ surprisingly has less variability, with remarkable reproducibility over a 3-day period in 19 subjects. There was a small but significant difference in the levels measured in the morning versus afternoon. There was also a good reproducibility in 32 subjects from a different cohort over a 12-week period (Ertekin-Taner et al. 2008).
Taken together, the interpretation of the cross-sectional studies may be complicated by the complex nature of plasma Aβ, whereas longitudinal studies of plasma Aβ may be a better indicator of disease progression. Further investigations are necessary to understand Aβ production and clearance, and may lead to a better understanding of the diagnostic potential of plasma Aβ.
Mouse
In addition to endogenous mouse APP expression, transgenic mice overexpress human APP under the regulation of a specific promoter element. Endogenous mouse APP is found primarily in the brain and lung with lower levels of expression in the spleen, stomach, large intestine, and skin (Kawarabayashi et al. 2001). The promoter that drives the transgene dictates the expression of human APP in mouse models of AD, hence, this expression is highly model specific. For example, in Tg2576 mice human APP is expressed at high levels in brain, spleen and lung, with lower levels of transgene expression in skin, bone, muscle, heart, pancreas, stomach, and large intestine (Kawarabayashi et al. 2001). BACE1 expression, which is necessary for the formation of Aβ42, is limited to the brain of wild-type mice by Western blot analysis (Laird et al. 2005). By sensitive ELISA measurements, Aβ has been detected at low levels in peripheral organs (10–24 pmol/g), whereas the levels in the brain were 20- to 40-fold higher in Tg2576 mice (Kawarabayashi et al. 2001). Therefore, the expression patterns of human APP and mouse BACE1 are likely to affect the availability of Aβ in plasma, and should be considered when interpreting the plasma Aβ data from mouse models of AD.
Similar to the data in humans, plasma Aβ levels in AD mouse models are conflicting. Using the Tg2576 mouse model, Kawarabayashi et al. have shown that the plasma levels of Aβ are inversely related to Aβ plaque burden (Kawarabayashi et al. 2001). As mentioned above, Aβ formation in this model is high in the brain, but also present in peripheral organs (Kawarabayashi et al. 2001). As total brain levels of Aβ increased, indicating increasing plaque formation, CSF and plasma levels of Aβ concurrently decreased. This was not the case in wild-type mice, and therefore could not be attributed to normal aging (Kawarabayashi et al. 2001).
Aβ levels in plasma and CSF in the PDAPP mouse model of AD do not correspond with the findings in Tg2576 mice. In these mice, human APP expression is found only in the brain by Western blotting (DeMattos et al. 2001). DeMattos et al. have reported a statistically significant positive correlation between CSF and plasma Aβ levels in young mice prior to the onset of amyloid deposition. However, a robust correlation between CSF and plasma Aβ was absent in older mice that were just beginning to accumulate amyloid plaques. If the older mouse cohort was divided into subsets by presence of amyloid plaques, the ratio of CSF to plasma Aβ was found to be twice as high in mice with amyloid plaques compared to mice without amyloid plaques. Unlike the observations by Kawarabayashi et al., this increase was attributed to higher CSF Aβ levels in the mice with amyloid plaques. Furthermore, the plasma Aβ levels did not correlate with the amyloid burden in the brain (DeMattos et al. 2002b). Hence, neither the levels of plasma Aβ alone or the ratio of CSF:plasma Aβ provided a clear cut prediction of amyloid formation in these mice.
Hence, the cross-sectional studies using mouse models of AD indicate that different models yield varying results, and corroborate the human data outlined in the previous section suggesting that such studies may not yield a reliable biomarker of early AD.
Challenges in Measuring Plasma Aβ
A factor that may contribute to the inconsistent data on plasma Aβ levels in both humans and transgenic mouse models of AD could be the difficulty in measuring Aβ by traditional ELISA assays. APP and other soluble APP fragments in biological samples may compete with Aβ peptides for capture and detection antibody in an ELISA assay (Golde et al. 2000). It has been shown that 6E10, a common antibody used in Aβ-specific ELISA assays, binds full-length APP, which could potentially interfere with the ability of 6E10 to sensitively detect Aβ species in plasma (Englund et al. 2007). Englund et al. have also demonstrated that an elevated level of Aβ protofibrils formed during the Aβ aggregation process leads to a reduced signal by traditional sandwich ELISA (Englund et al. 2007). Since oligomeric Aβ species are poorly detected by Aβ ELISA assays, only a subset of Aβ species present in the biological samples are accurately measured, leading to a potential underestimation of total Aβ levels (Stenh et al. 2005). Furthermore, presence of N-terminally truncated Aβ species in AD brains may create some problems for ELISA assays with N-terminal capture antibodies (Naslund et al. 1994; Ida et al. 1996).
Aβ binding proteins in the plasma also pose problems in measuring Aβ levels. Proteins such as albumin (Biere et al. 1996), α2 macroglobulin (Kuo et al. 1999), various lipoproteins (Koudinov et al. 1994; Biere et al. 1996), and others (Kuo et al. 1999) are known to bind Aβ. Some studies have shown that large quantities of Aβ may remain “sequestered” by binding proteins, and interfere with ELISA quantification (Kuo et al. 2000a; Slemmon et al. 2007). This “masking” effect by the plasma binding proteins (Kuo et al. 1999) may also strengthen the case for longitudinal studies rather than cross-sectional studies. There is probably less variability in binding protein compositions within a subject than between subjects, as long as there has not been a major change in health that may affect binding proteins levels such as albumin.
Different steps in blood sample processing can also lead to underestimation of Aβ levels in plasma. Processing of the whole blood to plasma would spin down the platelets which are known to contribute to the blood Aβ pool (Bush et al. 1990; Chen et al. 1995; Evin et al. 2003). However, one study has demonstrated that over 90% of the Aβ appears to remain within the plasma component when compared to the Aβ levels in the whole blood prior to processing (Slemmon et al. 2007). Other steps in the sample processing that influence plasma Aβ detection has been reviewed previously (Vanderstichele et al. 2000).
Antibody-Modulated Plasma Aβ Levels
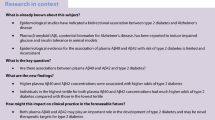
Although the utility of plasma Aβ as a biomarker for AD is difficult to interpret, the data collected from CSF samples appear to be more consistent. The inherent challenges in measuring plasma Aβ may further limit the potential of this strategy. However, it has been proposed that the equilibrium of Aβ can be disturbed by the administration of an Aβ-binding agent, such as an Aβ-specific antibody, in the blood. By binding Aβ in the blood, the antibody can potentially sequester plasma Aβ, shifting the equilibrium of soluble Aβ species, and causing a net efflux of Aβ from the brain to the plasma (Fig. 1) (DeMattos et al. 2001, 2002a). This hypothesis is designated the “peripheral sink mechanism” (DeMattos et al. 2001). Such an approach could maximize the levels of Aβ available for detection in the plasma. In the following paragraphs, we will outline the data in support for using Aβ-specific antibodies to detect plasma Aβ.

Amyloid-beta (Aβ) 1-40 and 1-42 are synthesized in the brain (Laird et al. 2005) (1), as well as in the periphery (Irizarry et al. 1997; Joachim et al. 1989; Vassar et al. 1999) (2). Circulating Aβ peptides enter the blood stream (3) and are partly cleared by the LRP-1 receptors in the liver (Tamaki et al. 2006) (4). Soluble extracellular brain Aβ (5) may accumulate in the brain parenchyma as amyloid plaques. Receptor mediated movement of the soluble Aβ through the blood–brain barrier (BBB) (6) is mediated by transporters such as low-density lipoprotein receptor-related protein-1 (LRP-1) (Deane et al. 2004; Shibata et al. 2000) for efflux, and receptor for advanced glycation end products (RAGE) (Deane et al. 2003) for influx. Once in the blood, Aβ peptides are bound by numerous binding proteins such as ApoE (Tanzi et al. 2004), albumin (Biere et al. 1996), and others (7). Aβ-specific IgG is also able to bind Aβ peptide in the blood, and may induce efflux of Aβ from the brain to the blood via the “peripheral sink” mechanism (DeMattos et al. 2001)
Human
Following antibody-mediated amelioration of Aβ deposition and behavioral deficits after Aβ vaccinations in tg mouse models of AD (Janus et al. 2000; Morgan et al. 2000), Dodel et al. examined whether naturally occurring human antibodies which recognizes Aβ can be used for treatment of AD. The first study involving 7 subjects with neurological disorders receiving intravenous immunoglobulin (IVIG) demonstrated that there was a significant reduction in the CSF Aβ levels accompanied by a significant increase in serum Aβ (Dodel et al. 2002). In another study involving 5 AD patients, infusion of IVIG again resulted in decrease in CSF Aβ with increase in serum Aβ (Dodel et al. 2004). This was similar to the observations in the tg mouse models of AD (see below), but more studies will need to be conducted to determine whether the Aβ levels after IVIG can be used as a biomarker. In active immunization trials, generation of antibodies against Aβ was not associated with changes in CSF or plasma Aβ levels (Hock et al. 2003).
Mouse
In 2001, DeMattos et al. demonstrated that administration of an antibody against the mid-region of Aβ (m266) was able to induce a rapid increase of Aβ total:IgG complex from 150 pg/ml basal level to at least 15,000 pg/ml 6 h after i.v. antibody administration in young PDAPP mice prior to plaque onset (DeMattos et al. 2001). This group has previously shown that the unmodified plasma Aβ40 levels in PDAPP mice do not correlate with brain amyloid plaque burden (DeMattos et al. 2002b), in concordance with the human studies outlined above. However, administration of the m266 antibody in this mouse model induced an efflux of Aβ40 from the central nervous system (CNS) into the plasma that correlated with the brain amyloid plaque load (DeMattos et al. 2002a). The m266 antibody has also been utilized to demonstrate a dose-dependent increase in plasma Aβ40 levels in PDAPP transgenic mice following i.p. injections, which was accompanied by cognitive improvement, suggesting that antibody injection may also have therapeutic benefits (Dodart et al. 2002).
Levites et al. have further characterized the effect of Aβ antibody injection in young Tg2576 mice prior to the onset of amyloid plaque deposition. This group demonstrates a 25-fold increase in plasma levels of Aβ42 within 1 day following intraperitoneal (i.p.) administration of 500 μg Ab9 (a mouse monoclonal antibody with epitope within Aβ1-16). Furthermore, an Ab9:Aβ40 complex with a half-life of approximately 7 days is detected in the plasma. Preclearing the plasma with a protein A/G, which removes mouse IgG, abolished greater than 90% of the plasma Aβ ELISA signal. This data suggests that the majority of Aβ that is detected in plasma is bound to the injected antibody, and that the Aβ:antibody complex is not a classic immune complex subject to rapid clearance (Levites et al. 2006). This supports the idea that the administration of Aβ antibody in mouse models of AD may be a feasible approach to maximize the measurable levels of Aβ in the plasma.
In support of using a peripheral sink mechanism to enhance the detection of Aβ in blood, a number of studies have demonstrated enhanced levels of Aβ total, Aβ40 and/or Aβ42 after Aβ antibody administration (Table 2) (Lemere et al. 2003; Asami-Odaka et al. 2005; Hartman et al. 2005; DaSilva et al. 2006; Gray et al. 2007; Takata et al. 2007). However, the increases in Aβ after Aβ antibody administration vary from 2-fold to approximately 1,000-fold (Table 2), and in some cases there is no significant difference between antibody-induced Aβ levels and controls (Seabrook et al. 2006; Zamora et al. 2006). There is also considerable divergence in the plasma Aβ levels reported in two separate studies that employed the same antibody (m266) and the same mouse model (Table 2) (DeMattos et al. 2001; Dodart et al. 2002). Patients at risk for AD may exhibit very mild elevations in soluble Aβ levels as compared to healthy controls, therefore it is possible that very large inductions in plasma Aβ are necessary to identify the at-risk population. This potential caveat needs to be further examined in order to ascertain the feasibility of antibody-induced Aβ levels as a diagnostic biomarker.
Furthermore, the increases in plasma Aβ levels are compared to different types of controls in the above-mentioned studies, including pre-injection Aβ levels (DeMattos et al. 2001; Gray et al. 2007; Takata et al. 2007), Aβ levels in transgenic mice given vehicle (Dodart et al. 2002; Asami-Odaka et al. 2005; DaSilva et al. 2006; Seabrook et al. 2006; Zamora et al. 2006), and Aβ immunized wild-type mice (Lemere et al. 2003). All humans produce Aβ, but it is possible that people at risk for AD have a higher production of Aβ compared to normal controls. Similarly, non-transgenic mice produce endogenous mouse Aβ at lower levels than the human Aβ that is produced in transgenic AD mouse models. Therefore, non-transgenic mice, or mice producing human Aβ at a lower level, could serve as an appropriate control for studies testing the efficacy of agents that induce Aβ efflux from the brain to the blood, yet these types of controls are not always included.
Instead, the increases in Aβ are commonly compared to “baseline” Aβ readings, which does not provide much information regarding if the Aβ elevations in patients at risk for AD would be distinguishable from those of a healthy individual. In addition, the range of controls used in these animal studies may account for some of the variability in plasma Aβ increases. The variations in fold-Aβ elevations may also be attributable to the Aβ antibodies, tg mouse models, injection routes, and detection systems used.
Moreover, plasma Aβ levels may change with age due to changes in clearance of the Aβ peptide (Tamaki et al. 2006). Hence, it will be important to determine the ability of Aβ antibodies to induce elevations in young transgenic mice that have not yet developed amyloid plaques, as it is crucial that AD can be detected prior to the onset of symptoms. This has been tested in one mouse model where Aβ levels were elevated by approximately 500% in pre-plaque mice and 250% in mice that had developed amyloid plaques (Takata et al. 2007). However, the dose of antibody administered in this study differed for the two age groups, making it difficult to directly compare the effectiveness of Aβ antibody to induce Aβ efflux from the brain at different ages (Table 2) (Takata et al. 2007).
In order to optimize antibody-induced increases in Aβ levels for a diagnostic test, the most suitable antibody (isotype, affinity, and epitope), injection route, kinetics and detection system must be determined. As will be discussed in the following paragraph, the detection of antibody-induced Aβ levels has its own set of inherent challenges.
Challenges in Measuring Antibody-Induced Plasma Aβ
Measurements of antibody-induced plasma Aβ levels may be confounded by the presence of a third antibody in the traditional sandwich ELISA design. In addition to the capture antibody (coating the ELISA plate) and the detection antibody (which detects the antigen bound to the capture antibody), the plasma Aβ that is measured in this assay may be complexed with the injected antibody used to sequester Aβ in the periphery. Aβ42 is a small peptide and many of the Aβ antibody epitopes overlap, potentially leading to steric hindrance in detection assays such as ELISAs. Gray et al. have shown that ELISA measurements of Aβ in plasma using 1A10 as the capture antibody are abrogated if the plasma sample is spiked with antibody 1A10. However, ELISA readings can be restored to near 100% if the plasma is treated with 2% SDS before dilution and addition to the ELISA plate (Gray et al. 2007). Further, as mentioned previously, oligomeric species of Aβ are poorly detected by ELISA assays (Englund et al. 2007), a complication that is likely to persist when antibody-induced Aβ levels are measured.
Other Modifiers of Plasma Aβ/Aβ binding Agents
Human
Similar to AD, insulin resistance syndrome is also prevalent in the US, and is associated with aging (Harris et al. 1998). Insulin receptors are present throughout peripheral tissues as well as in the brain (Schulingkamp et al. 2000). There are in vitro data suggesting that insulin increases extracellular Aβ by reducing insulin degrading enzyme (IDE)-mediated Aβ degradation (Qiu et al. 1998). In addition to competing with Aβ for IDE, insulin facilitates trans-Golgi network (TGN) transport of Aβ, and increases Aβ secretion (Gasparini et al. 2001). Hence, systemic insulin levels may affect the levels of plasma Aβ.
In humans, age-dependent increases in CSF Aβ42 levels were observed in cognitively normal subjects who received continuous insulin infusions compared to those who received saline infusions (Watson et al. 2003). Plasma Aβ42 levels were also increased in the insulin infusion group compared to the saline infusion group, and this increase in Aβ42 levels correlated with higher BMI values (Fishel et al. 2005). In another study, insulin infusion was able to induce greater percentage increases in plasma Aβ levels in AD patients, with no overall change in cognitively normal controls (Kulstad et al. 2006). AD patients of different ApoE genotypes may have different dose–response pattern to insulin infusion as assessed by cognitive tests as well as plasma APP levels (Craft et al. 2003). In addition to the possible mechanisms of plasma Aβ increases mentioned above, there may be other explanations for these observations (Kulstad et al. 2006). Insulin may act by activating insulin receptors present in the platelets and release Aβ via insulin signaling molecule phosphatidylinositol 3-kinase (PI3K) (Nystrom and Quon 1999; Skovronsky et al. 2001). Insulin may also mediate plasma Aβ levels via LRP-1 mediated clearance of Aβ40 as seen in rats (Tamaki et al. 2007), as well as by reducing the plasma level of APP in humans (Boyt et al. 2000). Finally, the observed increase in plasma Aβ may be secondary to enhanced efflux of Aβ from the brain, as can be inferred from insulin-induced increases in Aβ levels in the CSF (Watson et al. 2003). Therefore, insulin infusion appears as a potential tool in modulating plasma Aβ levels.
Mouse
Due to the concerns about the inflammatory effects of antibody injection (Robinson et al. 2003), other compounds that have Aβ binding capacity without immunomodulative effects have been explored in mice. Both gelsolin (Chauhan et al. 1999) and ganglioside GM1 (Choo-Smith et al. 1997) bind Aβ with high affinity, and gelsolin also co-immunoprecipitates with Aβ in human plasma (Chauhan et al. 1999). Additionally, only 1% of gelsolin can cross the blood–brain barrier (Saulino and Schengrund 1994) and GM1 is a large compound (86 kDa) unlikely to readily enter the CNS, indicating that these compounds may be well suited for maximizing plasma levels of Aβ. When these agents were administered to PS/APP tg mice by intraperitoneal injection by Matsouka and colleagues, GM1 induced an approximate twofold increase of plasma Aβ40 that was statistically significant. Three weeks after the initial GM1 administration, plasma Aβ42 levels were also nearly twofold higher than those of vehicle treated animals. However, intraperitoneal injection of gelsolin did not alter plasma Aβ levels. Both compounds reduced brain Aβ burden, and because of their low availability to the CNS, this suggests that these compounds are acting via peripheral sink mechanisms (Matsuoka et al. 2003).
Another agent known to bind amyloid is the histological dye Congo red. While Congo red readily the stains β-pleated sheet conformations of amyloid plaques, it has been reported to be a poor stain of diffuse amyloid deposits (Braak et al. 1989; Klunk et al. 1989). However, recent evidence of Congo red analogs with affinity for soluble oligomeric Aβ species has emerged (Maezawa et al. 2008). Intravenous administration of the Congo red derivative Chrysamine G results in a rapid and statistically significant increase in plasma Aβ40 levels, but this increase is minimal (125% of pretreatment) (Matsuoka et al. 2005). Other Congo red derivates tested in the study did not induce an increase in plasma Aβ levels (Matsuoka et al. 2005).
As mentioned previously, LRP-1 is a receptor which mediates transport of Aβ across the BBB, as well as clearance of systemic Aβ by the liver (Quinn et al. 1997; Shibata et al. 2000; Deane et al. 2004). LRP-1 binds Aβ with high affinity, and this binding is mediated by two domains known as cluster II and cluster IV (Deane et al. 2004). LRP-1 also has a higher affinity for Aβ than other LRP-1 ligands such as ApoE4 (Sagare et al. 2007), and soluble LRP is found in human plasma (Quinn et al. 1997), making it an ideal candidate for sequestration of Aβ in the plasma. Sagare et al. have utilized a soluble recombinant LRP fragment that encompasses cluster IV (LRP-IV) to induce peripheral sink activity in mice (Sagare et al. 2007). Intravenous administration of LRP-IV in wild-type C57BL/6 mice for 5 days resulted in a statistically significant twofold approximate increase in endogenous mouse Aβ40, and 1.5-fold increase in endogenous mouse Aβ42, as compared to vehicle injected mice. Similarly, statistically significant twofold increases in plasma Aβ40 and Aβ42 were observed in Tg2576 transgenic mice after daily i.p. injection of LRP-IV for 3 months, compared to vehicle. The plasma Aβ was primarily associated with LRP-IV, but LRP-IV was not found in the CSF and was not taken up by the brain (Sagare et al. 2007). This data suggests that LRP-IV may induce sequestration of plasma Aβ by a peripheral sink mechanism.
Finally, the Nogo-66 receptor (NgR) limits axonal growth in the human brain and also interacts with the central domain of Aβ (Park et al. 2006a, b). When NgR was administered subcutaneously over a period of 3 months in the APP/PS1 mouse model of AD, there was no significant difference in the absolute Aβ plasma levels of NgR treated animals compared to controls. However, treatment was accompanied by reductions in brain Aβ levels, improvement in cognitive performance, and a significant twofold increase in the ratio of plasma/brain Aβ42 (Park et al. 2006b). This data provides some evidence that plasma Aβ binding agents administered in circulation could create an efflux of Aβ from brain to blood.
While peripheral sequestration of Aβ by injection of agents with high affinity for Aβ appears to be a feasible approach to increase plasma Aβ levels, the agents tested to date have not yielded substantial increases in plasma Aβ as compared to vehicle. As mentioned above, considerable elevations in plasma Aβ may be necessary to differentiate individuals in the early stages of AD from healthy controls. Furthermore, in the studies mentioned above, the plasma Aβ levels after administration of the Aβ-binding agent have been compared either to pre-treatment plasma Aβ levels or to Aβ levels from vehicle treated transgenic animals. As demonstrated by Sagare et al., at least one of these Aβ binding agents, LRP-IV, is able to provoke increases in endogenous mouse Aβ in wild-type mice, as well as increases in human Aβ derived from transgene expression in Tg2576 mice (Sagare et al. 2007). All humans, whether they are at risk for AD or not, produce Aβ. Similarly, both transgenic mice and non-transgenic mice produce some form of Aβ, although the levels of Aβ are considerably higher in transgenic mice. None of the studies above have compared the increases in plasma Aβ levels induced by the Aβ binding agent in transgenic mice versus non-transgenic mice. Although this scenario would not be an ideal representation of a diagnostic test in humans, it would be important to examine how these agents might allow differentiation of plasma samples from AD patients compared to healthy controls.
Also, a careful kinetics study to determine when the Aβ levels peak after administration of the Aβ-binding agents will be necessary since the clearance of these agents will likely vary. Finally, as is the case with antibody-induced plasma Aβ levels, it is important that mice of different ages are tested with the Aβ-binding agents. Studies using mice with pathology ranging pre-onset to significant amyloid plaque burden are necessary in order to determine if these agents could be useful as a preclinical diagnostic test.
Conclusion
On the basis of the data in humans and tg mouse models of AD, unmodified levels of plasma Aβ alone do not appear to be reliable as a biomarker of AD at least in cross-sectional studies, while longitudinal studies seem more promising. Many modulators of plasma Aβ that are under investigation in humans as well as in animal models at this time, including Aβ antibodies, Aβ binding agents and insulin. These may be important in optimizing the plasma Aβ levels, and may improve the diagnostic potential of plasma Aβ. Standardization in the processing of the plasma would be also important (Golde et al. 2000; Galasko 2005) for the reasons discussed in this review article. Currently there are efforts to standardize the laboratory processing of plasma biomarkers, such as in the biomarker core of the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (Mueller et al. 2005). In addition, understanding of other factors such as location of Aβ synthesis and clearance would also play an important part in interpretation of Aβ as a biomarker.
Another possible approach to the utilization of Aβ as a biomarker of AD is the combination of this measurement with other biomarkers in the plasma, CSF, or imaging studies. A combination of multiple biomarkers would be very informative in predicting the subjects who would go on to develop AD (Ray et al. 2007). Furthermore, as many therapeutic agents that specifically target Aβ are under investigation at this time (Cummings et al. 2007), there is need for a biomarker that can provide information on whether these agents have affected the levels of brain Aβ (Galasko 2005). The importance of plasma Aβ remains as a non-invasive biomarker for monitoring the efficacy of these agents.
References
Andreasen, N., Hesse, C., Davidsson, P., Minthon, L., Wallin, A., Winblad, B., et al. (1999). Cerebrospinal fluid beta-amyloid(1-42) in Alzheimer disease: Differences between early- and late-onset alzheimer disease and stability during the course of disease. Archives of Neurology, 56, 673–680.
Asami-Odaka, A., Obayashi-Adachi, Y., Matsumoto, Y., Takahashi, H., Fukumoto, H., Horiguchi, T., et al. (2005). Passive immunization of the Abeta42(43) C-terminal-specific antibody BC05 in a mouse model of Alzheimer’s disease. Neurodegeneration Diseases, 2, 36–43.
Assini, A., Cammarata, S., Vitali, A., Colucci, M., Giliberto, L., Borghi, R., et al. (2004). Plasma levels of amyloid beta-protein 42 are increased in women with mild cognitive impairment. Neurology, 63, 828–831.
Bateman, R. J., Wen, G., Morris, J. C., & Holtzman, D. M. (2007). Fluctuations of CSF amyloid-beta levels: Implications for a diagnostic and therapeutic biomarker. Neurology, 68, 666–669.
Begley, D. J., & Brightman, M. W. (2003). Structural and functional aspects of the blood–brain barrier. Progress in Drug Research, 61, 39–78.
Biere, A. L., Ostaszewski, B., Stimson, E. R., Hyman, B. T., Maggio, J. E., & Selkoe, D. J. (1996). Amyloid beta-peptide is transported on lipoproteins and albumin in human plasma. Journal of Biological Chemistry, 271, 32916–32922.
Boyt, A. A., Taddei, T. K., Hallmayer, J., Helmerhorst, E., Gandy, S. E., Craft, S., et al. (2000). The effect of insulin and glucose on the plasma concentration of Alzheimer’s amyloid precursor protein. Neuroscience, 95, 727–734.
Braak, H., Braak, E., Ohm, T., & Bohl, J. (1989). Alzheimer’s disease: Mismatch between amyloid plaques and neuritic plaques. Neuroscience Letters, 103, 24–28.
Bush, A. I., Martins, R. N., Rumble, B., Moir, R., Fuller, S., Milward, E., et al. (1990). The amyloid precursor protein of Alzheimer’s disease is released by human platelets. Journal of Biological Chemistry, 265, 15977–15983.
Chauhan, V. P., Ray, I., Chauhan, A., & Wisniewski, H. M. (1999). Binding of gelsolin, a secretory protein, to amyloid beta-protein. Biochemical and Biophysical Research Communications, 258, 241–246.
Chen, M., Inestrosa, N. C., Ross, G. S., & Fernandez, H. L. (1995). Platelets are the primary source of amyloid beta-peptide in human blood. Biochemical and Biophysical Research Communications, 213, 96–103.
Choo-Smith, L. P., Garzon-Rodriguez, W., Glabe, C. G., & Surewicz, W. K. (1997). Acceleration of amyloid fibril formation by specific binding of Abeta-(1-40) peptide to ganglioside-containing membrane vesicles. Journal of Biological Chemistry, 272, 22987–22990.
Craft, S., Asthana, S., Cook, D. G., Baker, L. D., Cherrier, M., Purganan, K., et al. (2003). Insulin dose–response effects on memory and plasma amyloid precursor protein in Alzheimer’s disease: Interactions with apolipoprotein E genotype. Psychoneuroendocrinology, 28, 809–822.
Crystal, H., Dickson, D., Fuld, P., Masur, D., Scott, R., Mehler, M., et al. (1988). Clinico-pathologic studies in dementia: Nondemented subjects with pathologically confirmed Alzheimer’s disease. Neurology, 38, 1682–1687.
Cummings, J. L., Doody, R., & Clark, C. (2007). Disease-modifying therapies for Alzheimer disease: Challenges to early intervention. Neurology, 69, 1622–1634.
DaSilva, K., Brown, M. E., Westaway, D., & McLaurin, J. (2006). Immunization with amyloid-beta using GM-CSF and IL-4 reduces amyloid burden and alters plaque morphology. Neurobiology of Disease, 23, 433–444.
de Leon, M. J., DeSanti, S., Zinkowski, R., Mehta, P. D., Pratico, D., Segal, S., et al. (2004). MRI and CSF studies in the early diagnosis of Alzheimer’s disease. Journal of Internal Medicine, 256, 205–223.
De Strooper, B. (2003). Aph-1, Pen-2, and Nicastrin with Presenilin generate an active gamma-Secretase complex. Neuron, 38, 9–12.
Deane, R., Du Yan, S., Submamaryan, R. K., LaRue, B., Jovanovic, S., Hogg, E., et al. (2003). RAGE mediates amyloid-beta peptide transport across the blood–brain barrier and accumulation in brain. Nature Medicine, 9, 907–913.
Deane, R., Wu, Z., Sagare, A., Davis, J., Du Yan, S., Hamm, K., et al. (2004). LRP/amyloid beta-peptide interaction mediates differential brain efflux of Abeta isoforms. Neuron, 43, 333–344.
DeMattos, R. B., Bales, K. R., Cummins, D. J., Dodart, J. C., Paul, S. M., & Holtzman, D. M. (2001). Peripheral anti-A beta antibody alters CNS and plasma A beta clearance and decreases brain A beta burden in a mouse model of Alzheimer’s disease. Proceedings of the National Academy of Sciences of the United States of America, 98, 8850–8855.
DeMattos, R. B., Bales, K. R., Cummins, D. J., Paul, S. M., & Holtzman, D. M. (2002a). Brain to plasma amyloid-beta efflux: A measure of brain amyloid burden in a mouse model of Alzheimer’s disease. Science, 295, 2264–2267.
DeMattos, R. B., Bales, K. R., Parsadanian, M., O’Dell, M. A., Foss, E. M., Paul, S. M., et al. (2002b). Plaque-associated disruption of CSF and plasma amyloid-beta (Abeta) equilibrium in a mouse model of Alzheimer’s disease. Journal of Neurochemistry, 81, 229–236.
Dodart, J. C., Bales, K. R., Gannon, K. S., Greene, S. J., DeMattos, R. B., Mathis, C., et al. (2002). Immunization reverses memory deficits without reducing brain Abeta burden in Alzheimer’s disease model. Nature Neuroscience, 5, 452–457.
Dodel, R. C., Du, Y., Depboylu, C., Hampel, H., Frolich, L., Haag, A., et al. (2004). Intravenous immunoglobulins containing antibodies against beta-amyloid for the treatment of Alzheimer’s disease. Journal of Neurology, Neurosurgery and Psychiatry, 75, 1472–1474.
Dodel, R., Hampel, H., Depboylu, C., Lin, S., Gao, F., Schock, S., et al. (2002). Human antibodies against amyloid beta peptide: A potential treatment for Alzheimer’s disease. Annals of Neurology, 52, 253–256.
Englund, H., Sehlin, D., Johansson, A. S., Nilsson, L. N., Gellerfors, P., Paulie, S., et al. (2007). Sensitive ELISA detection of amyloid-beta protofibrils in biological samples. Journal of Neurochemistry, 103, 334–345.
Ertekin-Taner, N., Graff-Radford, N., Younkin, L. H., Eckman, C., Adamson, J., Schaid, D. J., et al. (2001). Heritability of plasma amyloid beta in typical late-onset alzheimer’s disease pedigrees. Genetic Epidemiology, 21, 19–30.
Ertekin-Taner, N., Younkin, L. H., Yager, D. M., Parfitt, F., Baker, M. C., Asthana, S., et al. (2008). Plasma amyloid beta protein is elevated in late-onset alzheimer disease families. Neurology, 70, 596–606.
Evin, G., Zhu, A., Holsinger, R. M., Masters, C. L., & Li, Q. X. (2003). Proteolytic processing of the Alzheimer’s disease amyloid precursor protein in brain and platelets. Journal of Neuroscience Research, 74, 386–392.
Fagan, A. M., Mintun, M. A., Mach, R. H., Lee, S. Y., Dence, C. S., Shah, A. R., et al. (2006). Inverse relation between in vivo amyloid imaging load and cerebrospinal fluid Abeta42 in humans. Annals of Neurology, 59, 512–519.
Fishel, M. A., Watson, G. S., Montine, T. J., Wang, Q., Green, P. S., Kulstad, J. J., et al. (2005). Hyperinsulinemia provokes synchronous increases in central inflammation and beta-amyloid in normal adults. Archives of Neurology, 62, 1539–1544.
Freeman, S. H., Raju, S., Hyman, B. T., Frosch, M. P., & Irizarry, M. C. (2007). Plasma Abeta levels do not reflect brain Abeta levels. Journal of Neuropathology and Experimental Neurology, 66, 264–271.
Fukumoto, H., Tennis, M., Locascio, J. J., Hyman, B. T., Growdon, J. H., & Irizarry, M. C. (2003). Age but not diagnosis is the main predictor of plasma amyloid beta-protein levels. Archives of Neurology, 60, 958–964.
Galasko, D. (2005). Biomarkers for Alzheimer’s disease—clinical needs and application. Journal of Alzheimers Disease, 8, 339–346.
Gasparini, L., Gouras, G. K., Wang, R., Gross, R. S., Beal, M. F., Greengard, P., et al. (2001). Stimulation of beta-amyloid precursor protein trafficking by insulin reduces intraneuronal beta-amyloid and requires mitogen-activated protein kinase signaling. Journal of Neuroscience, 21, 2561–2570.
Giedraitis, V., Sundelof, J., Irizarry, M. C., Garevik, N., Hyman, B. T., Wahlund, L. O., et al. (2007). The normal equilibrium between CSF and plasma amyloid beta levels is disrupted in Alzheimer’s disease. Neuroscience Letters, 427, 127–131.
Goate, A., Chartier-Harlin, M. C., Mullan, M., Brown, J., Crawford, F., Fidani, L., et al. (1991). Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer’s disease. Nature, 349, 704–706.
Golde, T. E., Eckman, C. B., & Younkin, S. G. (2000). Biochemical detection of Abeta isoforms: Implications for pathogenesis, diagnosis, and treatment of Alzheimer’s disease. Biochimica et Biophysica Acta, 1502, 172–187.
Graff-Radford, N. R., Crook, J. E., Lucas, J., Boeve, B. F., Knopman, D. S., Ivnik, R. J., et al. (2007). Association of low plasma Abeta42/Abeta40 ratios with increased imminent risk for mild cognitive impairment and Alzheimer disease. Archives of Neurology, 64, 354–362.
Gray, A. J., Sakaguchi, G., Shiratori, C., Becker, A. G., LaFrancois, J., Aisen, P. S., et al. (2007). Antibody against C-terminal Abeta selectively elevates plasma Abeta. NeuroReport, 18, 293–296.
Hardy, J., & Selkoe, D. J. (2002). The amyloid hypothesis of Alzheimer’s disease: Progress and problems on the road to therapeutics. Science, 297, 353–356.
Harris, M. I., Flegal, K. M., Cowie, C. C., Eberhardt, M. S., Goldstein, D. E., Little, R. R., et al. (1998). Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988–1994. Diabetes Care, 21, 518–524.
Hartman, R. E., Izumi, Y., Bales, K. R., Paul, S. M., Wozniak, D. F., & Holtzman, D. M. (2005). Treatment with an amyloid-beta antibody ameliorates plaque load, learning deficits, and hippocampal long-term potentiation in a mouse model of Alzheimer’s disease. Journal of Neuroscience, 25, 6213–6220.
Hock, C., Konietzko, U., Streffer, J. R., Tracy, J., Signorell, A., Muller-Tillmanns, B., et al. (2003). Antibodies against beta-amyloid slow cognitive decline in Alzheimer’s disease. Neuron, 38, 547–554.
Holsinger, R. M., McLean, C. A., Beyreuther, K., Masters, C. L., & Evin, G. (2002). Increased expression of the amyloid precursor beta-secretase in Alzheimer’s disease. Annals of Neurology, 51, 783–786.
Ida, N., Hartmann, T., Pantel, J., Schroder, J., Zerfass, R., Forstl, H., et al. (1996). Analysis of heterogeneous A4 peptides in human cerebrospinal fluid and blood by a newly developed sensitive Western blot assay. Journal of Biological Chemistry, 271, 22908–22914.
Irizarry, M. C. (2004). Biomarkers of Alzheimer disease in plasma. NeuroRx, 1, 226–234.
Irizarry, M. C., McNamara, M., Fedorchak, K., Hsiao, K., & Hyman, B. T. (1997). APPSw transgenic mice develop age-related A beta deposits and neuropil abnormalities, but no neuronal loss in CA1. Journal of Neuropathology and Experimental Neurology, 56, 965–973.
Iwatsubo, T. (1998). Amyloid beta protein in plasma as a diagnostic marker for Alzheimer’s disease. Neurobiology of Aging, 19, 161–163.
Janus, C., Pearson, J., McLaurin, J., Mathews, P. M., Jiang, Y., Schmidt, S. D., et al. (2000). A beta peptide immunization reduces behavioural impairment and plaques in a model of Alzheimer’s disease. Nature, 408, 979–982.
Jensen, M., Schroder, J., Blomberg, M., Engvall, B., Pantel, J., Ida, N., et al. (1999). Cerebrospinal fluid A beta42 is increased early in sporadic Alzheimer’s disease and declines with disease progression. Annals of Neurology, 45, 504–511.
Joachim, C. L., Mori, H., & Selkoe, D. J. (1989). Amyloid beta-protein deposition in tissues other than brain in Alzheimer’s disease. Nature, 341, 226–230.
Kanai, M., Matsubara, E., Isoe, K., Urakami, K., Nakashima, K., Arai, H., et al. (1998). Longitudinal study of cerebrospinal fluid levels of tau, A beta1-40, and A beta1-42(43) in Alzheimer’s disease: A study in Japan. Annals of Neurology, 44, 17–26.
Katzman, R., Terry, R., DeTeresa, R., Brown, T., Davies, P., Fuld, P., et al. (1988). Clinical, pathological, and neurochemical changes in dementia: A subgroup with preserved mental status and numerous neocortical plaques. Annals of Neurology, 23, 138–144.
Kawarabayashi, T., Younkin, L. H., Saido, T. C., Shoji, M., Ashe, K. H., & Younkin, S. G. (2001). Age-dependent changes in brain, CSF, and plasma amyloid (beta) protein in the Tg2576 transgenic mouse model of Alzheimer’s disease. Journal of Neuroscience, 21, 372–381.
Klunk, W. E., Pettegrew, J. W., & Abraham, D. J. (1989). Quantitative evaluation of congo red binding to amyloid-like proteins with a beta-pleated sheet conformation. Journal of Histochemistry and Cytochemistry, 37, 1273–1281.
Kosaka, T., Imagawa, M., Seki, K., Arai, H., Sasaki, H., Tsuji, S., et al. (1997). The beta APP717 Alzheimer mutation increases the percentage of plasma amyloid-beta protein ending at A beta42(43). Neurology, 48, 741–745.
Koudinov, A., Matsubara, E., Frangione, B., & Ghiso, J. (1994). The soluble form of Alzheimer’s amyloid beta protein is complexed to high density lipoprotein 3 and very high density lipoprotein in normal human plasma. Biochemical and Biophysical Research Communications, 205, 1164–1171.
Kulstad, J. J., Green, P. S., Cook, D. G., Watson, G. S., Reger, M. A., Baker, L. D., et al. (2006). Differential modulation of plasma beta-amyloid by insulin in patients with Alzheimer disease. Neurology, 66, 1506–1510.
Kuo, Y. M., Emmerling, M. R., Lampert, H. C., Hempelman, S. R., Kokjohn, T. A., Woods, A. S., et al. (1999). High levels of circulating Abeta42 are sequestered by plasma proteins in Alzheimer’s disease. Biochemical and Biophysical Research Communications, 257, 787–791.
Kuo, Y. M., Kokjohn, T. A., Kalback, W., Luehrs, D., Galasko, D. R., Chevallier, N., et al. (2000a). Amyloid-beta peptides interact with plasma proteins and erythrocytes: Implications for their quantitation in plasma. Biochemical and Biophysical Research Communications, 268, 750–756.
Kuo, Y. M., Kokjohn, T. A., Watson, M. D., Woods, A. S., Cotter, R. J., Sue, L. I., et al. (2000b). Elevated abeta42 in skeletal muscle of Alzheimer disease patients suggests peripheral alterations of AbetaPP metabolism. American Journal of Pathology, 156, 797–805.
Laird, F. M., Cai, H., Savonenko, A. V., Farah, M. H., He, K., Melnikova, T., et al. (2005). BACE1, a major determinant of selective vulnerability of the brain to amyloid-beta amyloidogenesis, is essential for cognitive, emotional, and synaptic functions. Journal of Neuroscience, 25, 11693–11709.
Lambert, M. P., Barlow, A. K., Chromy, B. A., Edwards, C., Freed, R., Liosatos, M., et al. (1998). Diffusible, nonfibrillar ligands derived from Abeta1-42 are potent central nervous system neurotoxins. Proceedings of the National Academy of Sciences of the United States of America, 95, 6448–6453.
Lemere, C. A., Spooner, E. T., LaFrancois, J., Malester, B., Mori, C., Leverone, J. F., et al. (2003). Evidence for peripheral clearance of cerebral Abeta protein following chronic, active Abeta immunization in PSAPP mice. Neurobiology of Disease, 14, 10–18.
Lesne, S., Koh, M. T., Kotilinek, L., Kayed, R., Glabe, C. G., Yang, A., et al. (2006). A specific amyloid-beta protein assembly in the brain impairs memory. Nature, 440, 352–357.
Levites, Y., Das, P., Price, R. W., Rochette, M. J., Kostura, L. A., McGowan, E. M., et al. (2006). Anti-Abeta42- and anti-Abeta40-specific mAbs attenuate amyloid deposition in an Alzheimer disease mouse model. Journal of Clinical Investigation, 116, 193–201.
Levy-Lahad, E., Wasco, W., Poorkaj, P., Romano, D. M., Oshima, J., Pettingell, W. H., et al. (1995). Candidate gene for the chromosome 1 familial Alzheimer’s disease locus. Science, 269, 973–977.
Lue, L. F., Kuo, Y. M., Roher, A. E., Brachova, L., Shen, Y., Sue, L., et al. (1999). Soluble amyloid beta peptide concentration as a predictor of synaptic change in Alzheimer’s disease. American Journal of Pathology, 155, 853–862.
Maezawa, I., Hong, H. S., Liu, R., Wu, C. Y., Cheng, R. H., Kung, M. P., et al. (2008). Congo red and thioflavin-T analogs detect Abeta oligomers. Journal of Neurochemistry, 107, 457–468.
Matsubara, E., Ghiso, J., Frangione, B., Amari, M., Tomidokoro, Y., Ikeda, Y., et al. (1999). Lipoprotein-free amyloidogenic peptides in plasma are elevated in patients with sporadic Alzheimer’s disease and Down’s syndrome. Annals of Neurology, 45, 537–541.
Matsumoto, Y., Yanase, D., Noguchi-Shinohara, M., Ono, K., Yoshita, M., & Yamada, M. (2007). Blood–brain barrier permeability correlates with medial temporal lobe atrophy but not with amyloid-beta protein transport across the blood–brain barrier in Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders, 23, 241–245.
Matsuoka, Y., Saito, M., LaFrancois, J., Saito, M., Gaynor, K., Olm, V., et al. (2003). Novel therapeutic approach for the treatment of Alzheimer’s disease by peripheral administration of agents with an affinity to beta-amyloid. Journal of Neuroscience, 23, 29–33.
Matsuoka, Y., Shao, L., Debnath, M., Lafrancois, J., Becker, A., Gray, A., et al. (2005). An Abeta sequestration approach using non-antibody Abeta binding agents. Current Alzheimer Research, 2, 265–268.
Mayeux, R., Honig, L. S., Tang, M. X., Manly, J., Stern, Y., Schupf, N., et al. (2003). Plasma A[beta]40 and A[beta]42 and Alzheimer’s disease: Relation to age, mortality, and risk. Neurology, 61, 1185–1190.
Mayeux, R., Tang, M. X., Jacobs, D. M., Manly, J., Bell, K., Merchant, C., et al. (1999). Plasma amyloid beta-peptide 1-42 and incipient Alzheimer’s disease. Annals of Neurology, 46, 412–416.
McLean, C. A., Cherny, R. A., Fraser, F. W., Fuller, S. J., Smith, M. J., Beyreuther, K., et al. (1999). Soluble pool of Abeta amyloid as a determinant of severity of neurodegeneration in Alzheimer’s disease. Annals of Neurology, 46, 860–866.
Mehta, P. D., Pirttila, T., Mehta, S. P., Sersen, E. A., Aisen, P. S., & Wisniewski, H. M. (2000). Plasma and cerebrospinal fluid levels of amyloid beta proteins 1-40 and 1-42 in Alzheimer disease. Archives of Neurology, 57, 100–105.
Mehta, P. D., Pirttila, T., Patrick, B. A., Barshatzky, M., & Mehta, S. P. (2001). Amyloid beta protein 1-40 and 1-42 levels in matched cerebrospinal fluid and plasma from patients with Alzheimer disease. Neuroscience Letters, 304, 102–106.
Morgan, D., Diamond, D. M., Gottschall, P. E., Ugen, K. E., Dickey, C., Hardy, J., et al. (2000). A beta peptide vaccination prevents memory loss in an animal model of Alzheimer’s disease. Nature, 408, 982–985.
Morris, J. C., & Price, A. L. (2001). Pathologic correlates of nondemented aging, mild cognitive impairment, and early-stage Alzheimer’s disease. Journal of Molecular Neuroscience, 17, 101–118.
Mueller, S. G., Weiner, M. W., Thal, L. J., Petersen, R. C., Jack, C. R., Jagust, W., et al. (2005). Ways toward an early diagnosis in Alzheimer’s disease: The Alzheimer’s Disease Neuroimaging Initiative (ADNI). Alzheimers and Dementia, 1, 55–66.
Naslund, J., Schierhorn, A., Hellman, U., Lannfelt, L., Roses, A. D., Tjernberg, L. O., et al. (1994). Relative abundance of Alzheimer A beta amyloid peptide variants in Alzheimer disease and normal aging. Proceedings of the National Academy of Sciences of the United States of America, 91, 8378–8382.
Neugroschl, J., & Davis, K. L. (2002). Biological markers in Alzheimer disease. American Journal of Geriatric Psychiatry, 10, 660–677.
Nystrom, F. H., & Quon, M. J. (1999). Insulin signalling: Metabolic pathways and mechanisms for specificity. Cellular Signalling, 11, 563–574.
Park, J. H., Gimbel, D. A., GrandPre, T., Lee, J. K., Kim, J. E., Li, W., et al. (2006a). Alzheimer precursor protein interaction with the Nogo–66 receptor reduces amyloid-beta plaque deposition. Journal of Neuroscience, 26, 1386–1395.
Park, J. H., Widi, G. A., Gimbel, D. A., Harel, N. Y., Lee, D. H., & Strittmatter, S. M. (2006b). Subcutaneous Nogo receptor removes brain amyloid-beta and improves spatial memory in Alzheimer’s transgenic mice. Journal of Neuroscience, 26, 13279–13286.
Pesaresi, M., Lovati, C., Bertora, P., Mailland, E., Galimberti, D., Scarpini, E., et al. (2006). Plasma levels of beta-amyloid (1-42) in Alzheimer’s disease and mild cognitive impairment. Neurobiology of Aging, 27, 904–905.
Price, D. L., & Sisodia, S. S. (1998). Mutant genes in familial Alzheimer’s disease and transgenic models. Annual Review of Neuroscience, 21, 479–505.
Price, J. L., & Morris, J. C. (1999). Tangles and plaques in nondemented aging and “preclinical” Alzheimer’s disease. Annals of Neurology, 45, 358–368.
Qiu, W. Q., Walsh, D. M., Ye, Z., Vekrellis, K., Zhang, J., Podlisny, M. B., et al. (1998). Insulin-degrading enzyme regulates extracellular levels of amyloid beta-protein by degradation. Journal of Biological Chemistry, 273, 32730–32738.
Quinn, K. A., Grimsley, P. G., Dai, Y. P., Tapner, M., Chesterman, C. N., & Owensby, D. A. (1997). Soluble low density lipoprotein receptor-related protein (LRP) circulates in human plasma. Journal of Biological Chemistry, 272, 23946–23951.
Ray, S., Britschgi, M., Herbert, C., Takeda-Uchimura, Y., Boxer, A., Blennow, K., et al. (2007). Classification and prediction of clinical Alzheimer’s diagnosis based on plasma signaling proteins. Nature Medicine, 13, 1359–1362.
Robinson, S. R., Bishop, G. M., & Munch, G. (2003). Alzheimer vaccine: Amyloid-beta on trial. Bioessays, 25, 283–288.
Sagare, A., Deane, R., Bell, R. D., Johnson, B., Hamm, K., Pendu, R., et al. (2007). Clearance of amyloid-beta by circulating lipoprotein receptors. Nature Medicine, 13, 1029–1031.
Saulino, M. F., & Schengrund, C. L. (1994). Differential accumulation of gangliosides by the brains of MPTP-lesioned mice. Journal of Neuroscience Research, 37, 384–391.
Scheuner, D., Eckman, C., Jensen, M., Song, X., Citron, M., Suzuki, N., et al. (1996). Secreted amyloid beta-protein similar to that in the senile plaques of Alzheimer’s disease is increased in vivo by the presenilin 1 and 2 and APP mutations linked to familial Alzheimer’s disease. Nature Medicine, 2, 864–870.
Schmitt, F. A., Davis, D. G., Wekstein, D. R., Smith, C. D., Ashford, J. W., & Markesbery, W. R. (2000). “Preclinical” AD revisited: Neuropathology of cognitively normal older adults. Neurology, 55, 370–376.
Schulingkamp, R. J., Pagano, T. C., Hung, D., & Raffa, R. B. (2000). Insulin receptors and insulin action in the brain: Review and clinical implications. Neuroscience and Biobehavioral Reviews, 24, 855–872.
Seabrook, T. J., Jiang, L., Thomas, K., & Lemere, C. A. (2006). Boosting with intranasal dendrimeric Abeta1-15 but not Abeta1-15 peptide leads to an effective immune response following a single injection of Abeta1-40/42 in APP-tg mice. J Neuroinflammation, 3, 14.
Selkoe, D. J. (1997). Alzheimer’s disease: Genotypes, phenotypes, and treatments. Science, 275, 630–631.
Selkoe, D. J. (2001). Clearing the Brain’s Amyloid Cobwebs. Neuron, 32, 177–180.
Selkoe, D. J. (2002). Deciphering the genesis and fate of amyloid beta-protein yields novel therapies for Alzheimer disease. Journal of Clinical Investigation, 110, 1375–1381.
Sherrington, R., Rogaev, E. I., Liang, Y., Rogaeva, E. A., Levesque, G., Ikeda, M., et al. (1995). Cloning of a gene bearing missense mutations in early-onset familial Alzheimer’s disease. Nature, 375, 754–760.
Shibata, M., Yamada, S., Kumar, S. R., Calero, M., Bading, J., Frangione, B., et al. (2000). Clearance of Alzheimer’s amyloid-ss(1-40) peptide from brain by LDL receptor-related protein-1 at the blood–brain barrier. Journal of Clinical Investigation, 106, 1489–1499.
Siemers, E. R., Dean, R. A., Friedrich, S., Ferguson-Sells, L., Gonzales, C., Farlow, M. R., et al. (2007). Safety, tolerability, and effects on plasma and cerebrospinal fluid amyloid-beta after inhibition of gamma-secretase. Clinical Neuropharmacology, 30, 317–325.
Siemers, E. R., Quinn, J. F., Kaye, J., Farlow, M. R., Porsteinsson, A., Tariot, P., et al. (2006). Effects of a gamma-secretase inhibitor in a randomized study of patients with Alzheimer disease. Neurology, 66, 602–604.
Silverberg, G. D., Mayo, M., Saul, T., Rubenstein, E., & McGuire, D. (2003). Alzheimer’s disease, normal-pressure hydrocephalus, and senescent changes in CSF circulatory physiology: A hypothesis. Lancet Neurology, 2, 506–511.
Sinha, S., Anderson, J. P., Barbour, R., Basi, G. S., Caccavello, R., Davis, D., et al. (1999). Purification and cloning of amyloid precursor protein beta-secretase from human brain. Nature, 402, 537–540.
Skovronsky, D. M., Lee, V. M., & Pratico, D. (2001). Amyloid precursor protein and amyloid beta peptide in human platelets. Role of cyclooxygenase and protein kinase C. Journal of Biological Chemistry, 276, 17036–17043.
Slemmon, J. R., Painter, C. L., Nadanaciva, S., Catana, F., Cook, A., Motter, R., et al. (2007). Distribution of Abeta peptide in whole blood. Journal of Chromatography. B, Analytical Technologies in the Biomedical and Life Sciences, 846, 24–31.
Small, S. A., & Gandy, S. (2006). Sorting through the cell biology of Alzheimer’s disease: Intracellular pathways to pathogenesis. Neuron, 52, 15–31.
Stenh, C., Englund, H., Lord, A., Johansson, A. S., Almeida, C. G., Gellerfors, P., et al. (2005). Amyloid-beta oligomers are inefficiently measured by enzyme-linked immunosorbent assay. Annals of Neurology, 58, 147–150.
Sundelof, J., Giedraitis, V., Irizarry, M. C., Sundstrom, J., Ingelsson, E., Ronnemaa, E., et al. (2008). Plasma beta Amyloid and the Risk of Alzheimer Disease and Dementia in Elderly Men: A Prospective, Population-Based Cohort Study. Archives of Neurology, 65, 256–263.
Sunderland, T., Linker, G., Mirza, N., Putnam, K. T., Friedman, D. L., Kimmel, L. H., et al. (2003). Decreased beta-amyloid1-42 and increased tau levels in cerebrospinal fluid of patients with Alzheimer disease. JAMA, 289, 2094–2103.
Takata, K., Hirata-Fukae, C., Becker, A. G., Chishiro, S., Gray, A. J., Nishitomi, K., et al. (2007). Deglycosylated anti-amyloid beta antibodies reduce microglial phagocytosis and cytokine production while retaining the capacity to induce amyloid beta sequestration. European Journal of Neuroscience, 26, 2458–2468.
Tamaki, C., Ohtsuki, S., Iwatsubo, T., Hashimoto, T., Yamada, K., Yabuki, C., et al. (2006). Major involvement of low-density lipoprotein receptor-related protein 1 in the clearance of plasma free amyloid beta-peptide by the liver. Pharmaceutical Research, 23, 1407–1416.
Tamaki, C., Ohtsuki, S., & Terasaki, T. (2007). Insulin facilitates the hepatic clearance of plasma amyloid beta-peptide (1-40) by intracellular translocation of low-density lipoprotein receptor-related protein 1 (LRP-1) to the plasma membrane in hepatocytes. Molecular Pharmacology, 72, 850–855.
Tamaoka, A., Fukushima, T., Sawamura, N., Ishikawa, K., Oguni, E., Komatsuzaki, Y., et al. (1996). Amyloid beta protein in plasma from patients with sporadic Alzheimer’s disease. Journal of the Neurological Sciences, 141, 65–68.
Tanzi, R. E., Moir, R. D., & Wagner, S. L. (2004). Clearance of Alzheimer’s Abeta peptide: The many roads to perdition. Neuron, 43, 605–608.
Tokuda, T., Fukushima, T., Ikeda, S., Sekijima, Y., Shoji, S., Yanagisawa, N., et al. (1997). Plasma levels of amyloid beta proteins Abeta1-40 and Abeta1-42(43) are elevated in Down’s syndrome. Annals of Neurology, 41, 271–273.
Troncoso, J. C., Martin, L. J., Dal Forno, G., & Kawas, C. H. (1996). Neuropathology in controls and demented subjects from the Baltimore Longitudinal Study of Aging. Neurobiology of Aging, 17, 365–371.
van Oijen, M., Hofman, A., Soares, H. D., Koudstaal, P. J., & Breteler, M. M. (2006). Plasma Abeta(1-40) and Abeta(1-42) and the risk of dementia: A prospective case-cohort study. Lancet Neurology, 5, 655–660.
Vanderstichele, H., Van Kerschaver, E., Hesse, C., Davidsson, P., Buyse, M. A., Andreasen, N., et al. (2000). Standardization of measurement of beta-amyloid(1-42) in cerebrospinal fluid and plasma. Amyloid, 7, 245–258.
Vassar, R., Bennett, B. D., Babu-Khan, S., Kahn, S., Mendiaz, E. A., Denis, P., et al. (1999). Beta-secretase cleavage of Alzheimer’s amyloid precursor protein by the transmembrane aspartic protease BACE. Science, 286, 735–741.
Walsh, D. M., Klyubin, I., Fadeeva, J. V., Cullen, W. K., Anwyl, R., Wolfe, M. S., et al. (2002). Naturally secreted oligomers of amyloid beta protein potently inhibit hippocampal long-term potentiation in vivo. Nature, 416, 535–539.
Watson, G. S., Peskind, E. R., Asthana, S., Purganan, K., Wait, C., Chapman, D., et al. (2003). Insulin increases CSF Abeta42 levels in normal older adults. Neurology, 60, 1899–1903.
Yang, L. B., Lindholm, K., Yan, R., Citron, M., Xia, W., Yang, X. L., et al. (2003). Elevated beta-secretase expression and enzymatic activity detected in sporadic Alzheimer disease. Nature Medicine, 9, 3–4.
Zamora, E., Handisurya, A., Shafti-Keramat, S., Borchelt, D., Rudow, G., Conant, K., et al. (2006). Papillomavirus-like particles are an effective platform for amyloid-beta immunization in rabbits and transgenic mice. Journal of Immunology, 177, 2662–2670.
Acknowledgments
This work was supported by the Johns Hopkins Alzheimer’s Disease Research Center (National Institutes of Health Grant PO1 AGO05146), John A. Hartford Foundation grant #2007-0005, Center of Excellence Renewal, at the Johns Hopkins School of Medicine, and an Anonymous Foundation. We would like to thank Dr. Abhay Moghekar and Dr. Philip Wong for their insightful comments on this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oh, E.S., Troncoso, J.C. & Fangmark Tucker, S.M. Maximizing the Potential of Plasma Amyloid-Beta as a Diagnostic Biomarker for Alzheimer’s Disease. Neuromol Med 10, 195–207 (2008). https://doi.org/10.1007/s12017-008-8035-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12017-008-8035-0