
Abstract
IgG4-associated cholangitis (IAC) is a major manifestation of immunoglobulin G4-related disease (IgG4-RD), an inflammatory multiorgan disorder of unknown cause. IAC and autoimmune pancreatitis (AIP) may mimic sclerosing cholangitis, cholangiocarcinoma, or pancreatic carcinoma. Typically, elderly male patients present with abdominal discomfort, weight loss, jaundice, and itch. At present, no accurate diagnostic test for IAC and IgG4-RD is at hand, often causing significant diagnostic delay. Serum IgG4 is only diagnostic when markedly raised (>4× ULN). Imaging in IAC discloses mass-forming lesions and/or strictures in the biliary tract. Histology may show tissue infiltration of IgG4-expressing plasma cells. Diagnostic criteria for histologic and imaging findings, serum tests, organ manifestation pattern, and response to immunosuppressive therapy (HISORt) criteria are used for the diagnosis of IgG4-RD. Still, considering the difficulty in diagnosing IAC and AIP, unnecessary hepatic or pancreatic resections for presumed malignancies occur. The good response to corticosteroid therapy in IAC and other manifestations of IgG4-RD suggests an immune-mediated inflammatory disease. Maintenance immunosuppression after induction of remission is needed in the majority of patients to avoid relapse. The pathogenesis of IAC and IgG4-RD remains poorly understood. Unresolved questions include: (i) Does IgG4 have a pro- or anti-inflammatory role in IAC? (ii) Is IAC a B cell- and/or T cell-mediated disease? (iii) Which are the molecular targets attacked by the immune system in IgG4-RD? Here, we review the diagnostic and therapeutic management of the disease and discuss recent pathophysiological findings, which might help to better understand the molecular mechanisms contributing to IAC and other manifestations of IgG4-RD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
IgG4-associated cholangitis (IAC) [1–3], also known as IgG4-related (sclerosing) cholangitis (IgG4-RSC) [4], is thought to be an immune-mediated inflammatory disease characterized by inflammatory lesions in the pancreaticobiliary tract with massive infiltration of lymphocytes—especially IgG4-positive B cells—in the bile duct wall, elevated IgG4 serum levels, and good response to corticosteroid treatment. IAC belongs to the spectrum of immunoglobulin G4-related disease (IgG4-RD), which encompasses a large number of medical conditions that share similar histopathological features [5]. Many organs can be affected both simultaneously as well as consecutively (Table 1). The pancreaticobiliary tract is one of the major localizations of IgG4-RD [2]. IAC is often accompanied by autoimmune pancreatitis (AIP), the most widely studied organ manifestation of IgG4-RD. Pathophysiological mechanisms that lead to IAC and other organ manifestations of IgG4-RD remain largely unknown.
First, we provide an overview of historical and epidemiological aspects of IAC and discuss the clinical dilemmas physicians face in the diagnosis and treatment of patients with IAC. In the second part, we address key questions regarding the pathophysiology of IAC and other IgG4-RD that researchers in the field are currently seeking to answer.
Clinical Aspects of IAC
How Was IAC Discovered?
Long before the concept of an IgG4-related systemic disease was established, first cases of this inflammatory disease of the hepatobiliary tract were reported. In 1963, Bartholomew et al. described two patients with sclerosing cholangitis associated with Riedel’s struma and fibrous retroperitonitis, respectively, bringing forward the idea of a systemic inflammatory disease with at least three organ manifestations [6]. During the next 25 years, several cases of sclerosing cholangitis in association with inflammatory changes of other organs were reported, including the pancreas, salivary and lacrimal glands, orbit, mediastinum, and lymph nodes [7–12]. In 1999, Erkelens et al. reported four cases of sclerosing pancreatocholangitis responsive to corticosteroid treatment [13]. In 2001, Hamano et al. described elevated serum levels of the immunoglobulin G4 subtype in patients with sclerosing pancreatitis [14]. In 2003, Kamisawa et al. disclosed stereotypical histopathological features of infiltrating IgG4-bearing plasma cells and a specific pattern of storiform fibrosis in various affected organs, suggestive of a systemic “autoimmune” disease with multiple organ manifestations [15], today known as IgG4-RD. In 2007, the term IAC was introduced [16] as a distinct organ manifestation of IgG4-RD [4].
What Are the Patient Characteristics?
Patients with IAC and AIP are generally over 60 years old and are predominantly male (male/female ratio up to 8:1) [1, 17–19]. A recent study suggested that the majority of patients with IAC and AIP in two independent cohorts had a career in “blue-collar” occupations with long-term exposure to solvents, industrial gases, and other environmental agents [20], indicating a possible role for environmental factors in the development of IAC and AIP. More than half of the patients with AIP also have hepatobiliary manifestations [21], and most patients with IAC show involvement of the pancreas [1], which underscores the close relationship between the two manifestations. Very limited data exists on incidence and prevalence. In a nationwide survey of AIP in Japan, the overall prevalence rate was estimated on 2.2 per 100,000 inhabitants, with an annual incidence rate of 0.9 per 100,000 inhabitants [21]. Whether prevalence rates in Western countries are similar remains to be clarified. IAC and AIP are underdiagnosed due to limited awareness among physicians and lack of accurate diagnostic markers.
How to Diagnose IAC?
Establishing the diagnosis, IAC can be challenging. Clinically, patients present with obstructive jaundice, mild to moderate abdominal pain, and weight loss. Pancreatic involvement may cause new onset diabetes mellitus or steatorrhea. On radiological imaging, mass forming or sclerosing lesions may be seen. In this phase, it may be difficult to distinguish IAC from the more common diagnoses of pancreaticobiliary malignancies [22] and sclerosing cholangiopathies, such as primary sclerosing cholangitis (PSC) [23]. Historically, the diagnosis of IAC has frequently been missed, resulting in needless surgery, radiation therapy, or medication for presumed malignancy. Indeed, in up to a third of patients in current IAC cohorts, extensive surgery has taken place erroneously prior to diagnosis [1, 24].
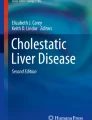
Thus, what are the diagnostic features of IAC? Cholangiography may reveal narrowing of the bile ducts on different levels, each manifestation carrying its own differential diagnosis [25]: hilar stenoses show radiographic similarities with Klatskin tumors (Fig. 1), whereas distal stenosis of the common bile duct mimics chronic pancreatitis, pancreatic cancer, or cholangiocarcinoma [3, 26, 27]. Strictures more diffusely distributed throughout the intra- and extrahepatic bile ducts resemble PSC (Fig. 2). However, unlike PSC, IAC generally presents in elderly men (>60 years old), has no clear association with inflammatory bowel disease, and is frequently accompanied by pancreatic inflammation.

A 69-year-old painter presented with icterus and weight loss. CT scan showed dilatation of intrahepatic bile ducts. ERCP disclosed hilar stenosis compatible with Klatskin tumor Bismuth type IIIa. Serum IgG4 levels were 1,440 mg/dL. The stenosis completely disappeared after prednisolone treatment
Hematological examinations may show, in addition to an increase in cholestatic parameters such as ALP, γ-GT and serum bilirubin, and tumor marker CA 19-9, elevation of IgG4 serum levels. However, IgG4 levels are not diagnostic when only moderately elevated (<4× ULN), as both pancreaticobiliary cancers and PSC can exhibit a rise in IgG4 levels [28–30]. In addition, in ~20–25 % of IAC and AIP patients, normal IgG4 levels are observed (<140 mg/dL) [1, 31]. Other serum markers such as rheumatoid factor and anti-nuclear antibodies may be positive in a number of patients but lack specificity and sensitivity [32]. Thus far, no disease-specific serum (auto)antibodies have been identified yet. However, one immunohistochemical study claimed that sera of AIP patients but not of healthy controls showed reactivity with epithelial cells in pancreatic and bile ducts. This would suggests the presence of disease-specific autoantibodies [33], but adequate disease controls such as PSC were lacking in this study. Serum CA 19-9, a tumor marker for cancer in the pancreaticobiliary system, however is not useful in the differentiation between malignancy and IAC or AIP, as this marker is often elevated in IAC and AIP patients [29, 30].
Histopathologically, bile duct and liver biopsies are characterized by (1) infiltration by IgG4+ B cells and terminally differentiated plasma cells, as well as CD4+ T cells, (2) obliterative phleblitis, and (3) fibrosis in later stages of chronic inflammation, arranged in a storiform pattern [5]. The diagnostic value of the number of infiltrating IgG4+ plasma cells depends on the cutoff level used. A commonly used threshold is >10 IgG4+-positive plasma cells per high-power field (HPF) [5]. In a comparative study of 29 IAC with (only) 6 PSC and 27 pancreaticobiliary carcinoma patients undergoing endoscopic biopsy of both the ampulla of Vater and bile duct, immunostaining showed more than 10 IgG4+ plasma cells per HPF in 72 % of the IAC patients in at least one of the biopsies [34]. However, false-positive rates were found in 12 % of the controls (1/6 PSC patients; 3/27 pancreaticobiliary carcinoma patients). Biopsy of the ampulla of Vater had a sensitivity of 52 % and specificity of 89 % comparable to biopsy of the bile ducts with a sensitivity and specificity of 52 and 96 %, respectively. A cutoff level of more than 20 IgG4+ plasma cells per HPF was highly specific but even less sensitive.
Many other organ systems can be involved in the disease, both simultaneously and consecutively, showing similar signs of swelling, loss of function, and characteristic infiltration of lymphocytes and (fibro)inflammatory histopathological features. Recognized localizations include the pituitary gland, salivary and lacrimal gland, orbit, thyroid, lung, gall bladder, aorta, retroperitoneum, kidney, prostate, and lymph node. Still, new localizations are proposed, such as the testes in one of our patients [35] and joints [36] (Table 1).
In case no conclusive diagnosis can be made, a short-term (2–4 weeks) treatment with corticosteroids may have to be considered to confirm the diagnosis IAC or AIP. A 2-week course of corticosteroid therapy was shown to be helpful to differentiate between AIP and pancreatic cancer, without negative consequences for resectability in case the tumor did not respond and turned out to be malignant [37].
In the absence of a highly sensitive and specific biomarker, several diagnostic criteria for individual organ manifestations of IgG4-RD in the pancreaticobiliary system have been developed over the years, including the Japanese criteria [25, 38], HISORt criteria [1, 39], and international consensus diagnostic criteria (ICDC) [40]. These criteria combine clinical, biochemical, radiological, and histomorphological findings, together with multiple-organ involvement and response to immunosuppressive therapy. A detailed description of the most generally applied HISORt criteria is depicted in Fig. 3.

Endoscopic retrograde cholangiogram of an 84-year-old former motorboat operator with IgG4 serum levels of 980 mg/dL, mimicking sclerosing cholangitis. All stenoses disappeared after treatment with prednisolone
How to Treat IAC?
Strictures and mass-forming lesions in IAC and AIP, similar to other organ manifestations of IgG4-RD, respond to corticosteroid treatment in up to 97 % [1, 17, 19], whereas corticosteroids in PSC have not shown any benefit.

Recommended initial treatment of IAC and AIP is prednisone at time of diagnosis for up to 3 months [1, 17, 19, 21]. Different starting doses are used worldwide, but common regimens are weight-based (0.6 mg kg−1 day−1) or fixed-dose strategies (20–40 mg/day), followed by a taper of varying duration [19]. However, thorough prospective dose-finding studies should be performed in order to define the lowest possible starting doses to reach a clear-cut therapeutic response, considering that side effects increase with dose.
Although corticosteroid treatment is very effective in the initial phase, relapses after discontinuation or after tapering the corticosteroid maintenance dose are common, reaching up to 50 % in patients with IAC and AIP during follow-up [1, 17, 19, 21, 41, 42]. To date, no consensus exists regarding maintenance regimens. Nevertheless, several studies seem to show a benefit on relapse rates of long-term treatment with low-dose corticosteroids and/or immunomodulators compared with no maintenance treatment [17, 19]. Widely used regimens are low-dose prednisone (2.5–5 mg/day) and/or azathioprine (1–2 mg kg−1 day−1) [1, 19].
Preliminary data of a prospective clinical trial among IgG4-RD patients suggest potential therapeutic efficacy of the anti-CD20 monoclonal antibody, rituximab, inducing remission by CD20+ B cell depletion and avoiding corticosteroid-induced side effects, such as osteoporotic fractures or glucose intolerance in the mostly elderly IAC patients (Stone, J et al. https://ww2.rheumatology.org/apps/MyAnnualMeeting/Abstract/38063). Taking into consideration a number of rare, but serious adverse events described for rituximab, including severe infusion reactions, cardiac arrest, or reactivation of viral infections (e.g., hepatitis B and progressive multifocal leucoencephalopathy), and the high costs, this escape therapy should be considered with reservation and only reserved for well-defined cases refractory to corticosteroid treatment.
Long-term survival is excellent in IAC patients after adequate therapy [18] and surgery for biliary strictures is not needed in most cases. Whether patients with IAC and AIP have an increased risk to develop malignancies as occasionally reported [43–46] is yet unclear [19] and needs further prospective, adequately controlled studies.
Pathogenesis of IAC and IgG4-RD
The pathophysiological mechanisms leading to IAC and other organ manifestations of IgG4-RD are poorly understood. A number of key questions await answers in order to better understand disease development and to further proceed in optimizing therapeutic strategies.
Does IgG4 Have a Pro- or Anti-inflammatory Role in IAC?
IAC and other organ manifestations of IgG4-RD earned their name due to the prominent appearance of IgG4+ B cells and plasma cells in affected tissues and elevated IgG4 serum levels. In some patients, IgG4 accounts for >50 % of total serum IgG, whereas in healthy individuals IgG4 form the smallest IgG fraction (<5 %). It is still unclear to what extent, if at all, IgG4 antibodies contribute to the pathogenesis and local inflammation in IgG4-RD disease, or are produced to dampen ongoing immune responses. The current state of knowledge on the role of IgG4 antibodies is limited in this disease and can be inferred only from research in various fields such as allergy, autoimmunity and cancer.
IgG4 antibodies are thought to have mostly anti-inflammatory properties. Several characteristics distinguish IgG4 from other IgG subclasses. IgG4 antibodies have a relatively low capacity to induce complement activation and to mediate pro-inflammatory immune responses, due to limited affinity for C1q and Fc-gamma receptors on immune cells [47–50]. In addition, IgG4 antibodies are known to have the unique ability of exchanging Fab-arms, a dynamic process by which half of the immunoglobulin molecule, a heavy chain plus attached light chain, is swapped with half of another IgG4 molecule, resulting in a bispecific and functionally monovalent antibody [51]. It thereby looses the capability to cross-link antigen and form immune complexes. Moreover, it has been reported that the Fc tail of IgG4 has the capacity to interact with the Fc tail of other pro-inflammatory IgG subclasses, thereby preventing the formation of immune complexes and blocking Fc-mediated effector functions [52].
This inferred anti-inflammatory activity of IgG4 is confirmed in high-dose allergen exposure models and suggests an import role for IgG4 in peripheral tolerance. In allergen-specific immunotherapy (SIT) for the treatment of allergy during the course of high-dose allergen exposure, clonal expansion of allergen-specific regulatory T cells (Tregs) leads to interleukin (IL)-10 and tumor growth factor beta (TGF-β) secretion suppressing IgE production and inducing B cell class-switching to IgG4 [53]. Consequently, antigen-specific IgG4 increases rapidly during SIT. Notably, allergen-specific IgG4 titers correlate with successful immunotherapy [54]. By competitive binding, IgG4 is thought to block both binding of the allergen to soluble IgE and to the membrane-bound IgE, thereby preventing the activation of mast cells and basophils [55, 56]. Similarly, in nonallergic beekeepers, continuous exposure to high doses of the bee venom allergen phospolipase A2 leads to an in vivo switch from allergen-specific Th1 and Th2 cells toward IL-10-producing Tregs, a diminution of T cell-mediated skin swellings and an increase in antigen-specific IgG4 levels [57]. Given its ability to block immune complex formation, these high (antigen-specific) IgG4 titers may protect against a potential anaphylactic shock upon bee venom exposure. However, the anti-inflammatory properties of IgG4 antibodies could also be disadvantageous. In human melanoma, IgG4 antibodies seem to antagonize IgG1-mediated human anti-melanoma immunity through competitive binding of Fc receptors on effector cells [58]. Furthermore, IgG4 serum titers were inversely correlated with patient survival [58].
Notably, other observations point to a pro-inflammatory role of IgG4: in IgG4-RD, a decrease of serum IgG4 titers under corticosteroid treatment is associated with clinical improvement. In pemphigus vulgaris, an autoimmune disease characterized by skin blistering, IgG4 antibodies against desmosome proteins have been proven to induce dermal–epidermal separation through Fc-dependent activation of leukocytes [59] although IgG4 autoantibodies were significantly less potent than IgG1 autoantibodies. However, in another autoimmune disease, myasthenia gravis, patients may generate IgG4 antibodies directed against muscle-specific kinase (MuSK), a postsynaptic transmembrane protein located at neuromuscular synapses. IgG4 antibodies interfere in the binding of protein Lrp4 to MuSK, thereby inhibiting Agrin-stimulated MuSK phosphorylation, thus reducing the efficiency of synaptic transmission. This results in muscle weakness [60, 61]. Antigen-specific IgG4 titers correlate with disease severity in these patients [62].
The role of IgG4 antibodies in IgG4-RD is unclear. Intriguingly, IgG4 serum titers often remain elevated in IAC patients in clinical remission, suggesting that IgG4 antibodies are not directly pathogenic in contrast to what has been observed in pemphigus vulgaris and MuSK myasthenia gravis.
What Are the Molecular Targets of the Immune Attack Causing IgG4-RD?
We recently reported that blue-collar workers dominated two independent cohorts with IAC and AIP patients, whereas in the control cohorts consisting of PSC patients, blue-collar work was less frequently observed [20]. This suggested to us that chronic exposure to potentially hazardous occupational substances could be causal to the disease, for instance, in response to solvents, industrial dusts, pesticides, or industrial oils to which the vast majority of our patients was exposed over the years. However, many patients were retired at the time of diagnosis. A possible explanation could be that exposure to hazardous substances causes alteration of the conformation of self-antigens, thereby provoking an (auto)immune response. Alternatively, possible tissue injury by these substances could result in the exposure of immunogenic self-antigens or the release of damage-associated molecular pattern molecules (DAMPs), thereby evoking a self-perpetuating immune response. Moreover, our finding of long-term exposure to solvents, industrial dusts, pesticides, or industrial oils in the majority of patients with IgG4-RD could well explain why IAC and AIP are predominantly diagnosed in elderly men. This is in contrast to many autoimmune diseases that generally have a striking female predominance. Intriguingly, a report from Braganza et al. in 1986—long before AIP was recognized as a disease entity—already suggested a potential pathogenic role for chemicals in 12 patients with idiopathic pancreatitis [63]. In retrospect, these patients may have been cases of AIP.
The finding of our group that highly expanded IgG4+ B cell clones dominate the B cell receptor repertoire in IAC patients and not in controls, suggests that an antigen-mediated immune response is pivotal in the pathogenesis of IAC and that these are most autoreactive [64]. This was very recently confirmed by Mattoo et al., who showed that expression of heavy and light chains from expanded plasma blasts found in vivo in IgG4-RD are self-reactive [65]. The search for target antigens has been a major objective in unraveling disease mechanisms in IgG4-RD.
In order to find evidence for autoimmunity, but also to discover diagnostic markers, this search has led to the characterization of several potential autoantibodies. In AIP patients for instance, autoantibodies against lactoferrin [66] and carbonic anhydrase II [67] are frequently detected. These antigens are expressed in acinar and epithelial duct cells of some exocrine glands, including the pancreas, bile ducts, salivary gland, and kidney. Moreover, autoantibodies against typsinogens [68], pancreatic secretory trypsinogen inhibitor [69], and amylase α-2A [70], secreted in the pancreatic juice, have been reported. However, none of these autoantibodies are specific for IgG4-RD and can be held accountable for all organ manifestations in IgG4-RD. In addition, no convincing proof has been delivered (yet) that the presence of these autoantibodies contributes to the pathogenesis of the disease, rather than reflecting an innocent bystander effect. Nevertheless, immunohistochemical staining of “healthy” tissue of various organs with sera from AIP patients showed reactivity of IgG4 against epithelial cells from (nonself) pancreatic ducts, bile ducts, gallbladder and salivary gland ducts [33], suggesting the existence of self-antigen(s).
The idea that an autoimmune response in IgG4-RD is not initiated by autologous antigens, but triggered by molecular mimicry of infectious agents as is thought to occur in Guillain-Barré syndrome [71] and other autoimmune diseases, has also acquired attention. A potential role of Helicobacter pylori infections in the pathogenesis of AIP in genetically predisposed subjects through antibody cross-reactivity has been suggested [72, 73]. This hypothesis was also supported by Frulloni et al., who screened sera from patients with AIP against a random peptide library [74]; 94 % of patients’ sera recognized a peptide that showed homology with the amino acid sequence of plasminogen-binding protein (PBP) of H. pylori and with an ubiquitin–protein ligase, UBR2, highly expressed in pancreatic acinar cells. However, the sequence that was found also showed homology with several other commensal and environmental microbes [75]. Moreover, PBP is expressed by many other enterobacteria. The finding that PBP is related to AIP remains to be confirmed and the report has been criticized on its lack of a proper control group [76].
A proteomics analysis by SELDI-TOF mass spectrometry on immunoprecipitated immune complexes from serum of 28 patients with IgG4-RD with different disease manifestations found a potential antigen of 13.1 kDa, which was not found in healthy and diseased controls, supporting the hypothesis of an antigen-driven immune response [77].
Further research is needed to identify possible target antigens and determine environmental factors and the way they might trigger a pathogenic immune response in IgG4-RD patients. In addition, it is also important to assess what the influence is of genetic makeup on susceptibility to IgG4-RD.
Is IAC a B cell- and/or T cell-Mediated Disease?
The inflammatory infiltrate in affected tissues of IgG4-RD is composed of many inflammatory cells, including IgG4+ B cells, CD4+ (and to a lesser extent CD8+) T cells, eosinophils, fibroblasts, and macrophages. Cytokine profiles in serum of patients with IAC and AIP, but also in patients with other variants of IgG4-RD, suggest a Th2-dominant immune response, with an increase in mRNA expression of IL-4, IL-5, IL-10, and IL-13 [78–80]. These cytokines may account for the activation of elevated serum IgE levels and eosinophilia, which are observed in about half of patients with IgG4-RD [81]. Another subset of CD4+ T lymphocytes that are regularly found in affected tissues are Tregs [78, 82, 83]. Possibly, these cells are secondarily induced in an attempt to inhibit a Th2-dominant immune response stimulating expansion and class-switching of B cells to IgG4 via the production of IL-10 and suppression of IgE [53], further enhancing an anti-inflammatory reaction. Moreover, Tregs may contribute to the process of fibrosis in inflamed tissue by stimulation of fibroblasts through the production of TGF-β [84], potentially fulfilling an important role in the pathogenesis of IgG4-RD.
Other key players are clonally expanded IgG4+ B cells [64], which have undergone affinity maturation as point mutations in the immunoglobulin heavy chain variable region were observed. This process occurs in the presence of T cells (and follicular dendritic cells) in germinal centers [85], which can be found in affected tissues in IgG4-RD [5].
Whether IgG4-producing B cells are driving the immune response or are induced in reaction to an inflammatory immune response to an unknown antigen, remains unclear. However, when B cells are targeted by rituximab inflammation in IgG4-RD patients reduces drastically [86], possibly by eliminating a direct pathogenic effect of B cells. Moreover, we observed an immediate decline of IgG4+ B cell and plasma cell clones in both peripheral blood and affected tissue in IAC suggesting a direct role for B cells and plasma cells in the disease process [64]. Alternatively, a reduction in B cell number could result in reduced B cell-mediated T cell activation, as B cells have been shown to enhance CD4+ T cell responses by presenting antigen and providing costimulation and polarizing cytokines, independently of antibody production [87].
How the innate immune system is involved in the disease process has not been thoroughly investigated. It is likely that dendritic cells, recognizing molecular patterns of damaged cells (DAMPs) and pathogens (PAMPs), present antigens to T and B cells, thereby linking innate and adaptive immunity. Moreover, in patients with IgG4-RD increased levels of B cell-activating factor (BAFF) and a proliferating-inducing ligand (APRIL), both members of the tumor necrosis factor family, were measured [88, 89]. BAFF and APRIL are produced by antigen-presenting cells, including dendritic cells, monocytes, and macrophages, and are known to enhance B cell survival during maturation in the periphery [90] and induce class switching [91].
Given the intimate relation between T cells, B cells, and innate lymphoid cells, unravelling the contribution of individual components of the immune system is challenging, and it seems unlikely that IgG4-RD pathophysiology can be attributed solely to a single immune cell type. Perhaps the interplay of T and B cells, together with innate lymphoid cells, in reaction to chronic exposure to (self) antigens, orchestrates a pathogenic immune response in genetically susceptible people, leading to the development of IAC and corresponding symptoms.
Perspectives and Challenges
Future studies will have to address several topics related to the pathogenesis of IAC and other manifestations of IgG4-RD, including the identification of potential (self-)antigens and determining the relative roles of B cells, T cells, and other immune cells in orchestrating the disease. In addition, the genetic background and environmental influences that make certain individuals more susceptible needs further investigation. Moreover, insights in underlying mechanisms could eventually lead to more specific treatment approaches.
In order to prevent misdiagnosis and unnecessary surgery, it is crucial that accurate diagnostic disease markers are developed. The diagnostic potential of the finding of dominant IgG4-positive BCR clones in active IAC patients, but not in controls [64], appears promising in this regard and is currently being investigated. Additionally, biomarkers that can measure disease activity, even before the onset of clinical symptoms, are needed in the therapeutic setting and could be of great help in developing personalized treatment regimens.
References
Ghazale A, Chari ST, Zhang L et al (2008) Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology 134:706–715
Stone JH, Zen Y, Deshpande V (2012) Mechanisms of disease: IgG4-related disease. N Engl J Med 366:539–551
Maillette de Buy Wenniger L, Rauws EA, Beuers U (2012) What an endoscopist should know about immunoglobulin-G4-associated disease of the pancreas and biliary tree. Endoscopy 44:66–73
Stone JH, Khosroshahi A, Deshpande V et al (2012) Recommendations for the nomenclature of IgG4-related disease and its individual organ system manifestations. Arthritis Rheum 64:3061–3067
Deshpande V, Zen Y, Chan JK et al (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25:1181–1192
Bartholomew LG, Cain JC, Woolner LB et al (1963) Sclerosing cholangitis: its possible association with Riedel’s struma and fibrous retroperitonitis. Report of two cases. N Engl J Med 269:8–12
Wenger J, Gingrich GW, Mendeloff J (1965) Sclerosing cholangitis—a manifestation of systemic disease. Increased serum gamma-globulin, follicular lymph node hyperplasia, and orbital pseudotumor. Arch Intern Med 116:509–514
Comings DE, Skubi KB, Van Eyes J, Motulsky AG (1967) Familial multifocal fibrosclerosis. Findings suggesting that retroperitoneal fibrosis, mediastinal fibrosis, sclerosing cholangitis, Riedel’s thyroiditis, and pseudotumor of the orbit may be different manifestations of a single disease. Ann Intern Med 66:884–892
Waldram R, Kopelman H, Tsantoulas D, Williams R (1975) Chronic pancreatitis, sclerosing cholangitis, and sicca complex in two siblings. Lancet 1:550–552
Sjögren I, Wengle B, Korsgren M (1979) Primary sclerosing cholangitis associated with fibrosis of the submandibular glands and the pancreas. Acta Med Scand 205:139–141
Montefusco PP, Geiss AC, Bronzo RL et al (1984) Sclerosing cholangitis, chronic pancreatitis, and Sjogren’s syndrome: a syndrome complex. Am J Surg 147:822–826
Semba D, Morioka Y (1987) A case of primary sclerosing cholangitis associated with chronic pancreatitis and Sjogren syndrome. Nihon Shokakibyo Gakkai Zasshi 84:2745–2749
Erkelens GW, Vleggaar FP, Lesterhuis W et al (1999) Sclerosing pancreato-cholangitis responsive to steroid therapy. Lancet 354:43–44
Hamano H, Kaw S, Horiuchi A et al (2001) High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 344:732–738
Kamisawa T, Funata N, Hayashi Y et al (2003) A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 38:982–984
Björnsson E, Chari ST, Smyrk TC, Lindor K (2007) Immunoglobulin G4 associated cholangitis: description of an emerging clinical entity based on review of the literature. Hepatology 45:1547–1554
Kamisawa T, Shimosegawa T, Okazaki K et al (2009) Standard steroid treatment for autoimmune pancreatitis. Gut 58:1504–1507
Tanaka A, Tazuma S, Okazaki K et al (2014) Nationwide survey for primary sclerosing cholangitis and IgG4-related sclerosing cholangitis in Japan. J Hepato-Biliary-Pancreat Sci 21:43–50
Hart PA, Kamisawa T, Brugge WR et al (2013) Long-term outcomes of autoimmune pancreatitis: a multicentre, international analysis. Gut 62:1771–1776
de Buy Wenniger LJM, Culver EL, Beuers U (2014) Exposure to occupational antigens might predispose to IgG4-related disease. Hepatology 60. doi:10.1002/hep.26999
Kanno A, Nishimori I, Kikuta K et al (2012) Nationwide epidemiological survey of autoimmune pancreatitis in Japan. Pancreas 41:835–839
Perez Alamino R, Espinoza LR, Zea AH (2013) The great mimicker: IgG4-related disease. Clin Rheumatol 32:1267–1273
Koyabu M, Uchida K, Fukata N et al (2010) Primary sclerosing cholangitis with elevated serum IgG4 levels and/or infiltration of abundant IgG4-positive plasma cells. J Gastroenterol 45:122–129
Erdogan D, Kloek JJ, ten Kate FJW et al (2008) Immunoglobulin G4-related sclerosing cholangitis in patients resected for presumed malignant bile duct strictures. Br J Surg 95:727–734
Ohara H, Okazaki K, Tsubouchi H et al (2012) Clinical diagnostic criteria of IgG4-related sclerosing cholangitis 2012. J Hepato-Biliary-Pancreat Sci 19:536–542
Kloek JJ, van Delden OM, Erdogan D et al (2008) Differentiation of malignant and benign proximal bile duct strictures: the diagnostic dilemma. World J Gastroenterol 14:5032–5038
Kamisawa T, Ohara H, Kim MH et al (2014) Role of endoscopy in the diagnosis of autoimmune pancreatitis and immunoglobulin G4-related sclerosing cholangitis. Dig Endosc 14:100–106
Mendes FD, Jorgensen R, Keach J et al (2006) Elevated serum IgG4 concentration in patients with primary sclerosing cholangitis. Am J Gastroenterol 101:2070–2075
Oseini AM, Chaiteerakij R, Shire AM et al (2011) Utility of serum immunoglobulin G4 in distinguishing immunoglobulin G4-associated cholangitis from cholangiocarcinoma. Hepatology 54:940–948
Ghazale A, Chari ST, Smyrk TC et al (2007) Value of serum IgG4 in the diagnosis of autoimmune pancreatitis and in distinguishing it from pancreatic cancer. Am J Gastroenterol 102:1646–1653
Kamisawa T, Takuma K, Tabata T et al (2011) Serum IgG4-negative autoimmune pancreatitis. J Gastroenterol 46:108–116
Sah RP, Chari ST (2011) Serologic issues in IgG4-related systemic disease and autoimmune pancreatitis. Curr Opin Rheumatol 23:108–113
Aoki S, Nakazawa T, Ohara H et al (2005) Immunohistochemical study of autoimmune pancreatitis using anti-IgG4 antibody and patients’ sera. Histopathology 47:147–158
Kawakami H, Zen Y, Kuwatani M et al (2010) IgG4-related sclerosing cholangitis and autoimmune pancreatitis: histological assessment of biopsies from Vater’s ampulla and the bile duct. J Gastroenterol Hepatol 25:1648–1655
De Buy Wenniger LM, Scheltema JM, Verheij J, Beuers U (2013) Testicular inflammation as a new manifestation of IgG4-associated disease. Urology 82:e15–e16
Shinoda K, Matsui S, Taki H et al (2011) Deforming arthropathy in a patient with IgG4-related systemic disease: comment on the article by Stone et al. Arthritis Care Res 63:172
Moon S-H, Kim M-H, Park DH et al (2008) Is a 2-week steroid trial after initial negative investigation for malignancy useful in differentiating autoimmune pancreatitis from pancreatic cancer? A prospective outcome study. Gut 57:1704–1712
Okazaki K, Kawa S, Kamisawa T et al (2006) Clinical diagnostic criteria of autoimmune pancreatitis: revised proposal. J Gastroenterol 41:626–631
Chari ST, Takahashi N, Levy MJ et al (2009) A diagnostic strategy to distinguish autoimmune pancreatitis from pancreatic cancer. Clin Gastroenterol Hepatol 7:1097–1103
Shimosegawa T, Chari ST, Frulloni L et al (2011) International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 40:352–358
Sah RP, Chari ST, Pannala R et al (2010) Differences in clinical profile and relapse rate of type 1 versus type 2 autoimmune pancreatitis. Gastroenterology 139:140–148, quiz e12–e13
Sandanayake NS, Church NI, Chapman MH et al (2009) Presentation and management of post-treatment relapse in autoimmune pancreatitis/immunoglobulin G4-associated cholangitis. Clin Gastroenterol Hepatol 7:1089–1096
Gupta R, Khosroshahi A, Shinagare S et al (2013) Does autoimmune pancreatitis increase the risk of pancreatic carcinoma?: a retrospective analysis of pancreatic resections. Pancreas 42:506–510
Shiokawa M, Kodama Y, Yoshimura K et al (2013) Risk of cancer in patients with autoimmune pancreatitis. Am J Gastroenterol 108:610–617
Yamamoto M, Takahashi H, Tabeya T et al (2012) Risk of malignancies in IgG4-related disease. Mod Rheumatol 22:414–418
Takahashi N, Ghazale AH, Smyrk TC et al (2009) Possible association between IgG4-associated systemic disease with or without autoimmune pancreatitis and non-Hodgkin lymphoma. Pancreas 38:523–526
Van der Zee JS, van Swieten P, Aalberse RC (1986) Inhibition of complement activation by IgG4 antibodies. Clin Exp Immunol 64:415–422
Bindon CI, Hale G, Brüggemann M, Waldmann H (1988) Human monoclonal IgG isotypes differ in complement activating function at the level of C4 as well as C1q. J Exp Med 168:127–142
Aalberse RC, Schuurman J (2002) IgG4 breaking the rules. Immunology 105:9–19
Aalberse RC, Stapel SO, Schuurman J, Rispens T (2009) Immunoglobulin G4: an odd antibody. Clin Exp Allergy 39:469–477
Van der Neut Kolfschoten M, Schuurman J, Losen M et al (2007) Anti-inflammatory activity of human IgG4 antibodies by dynamic Fab arm exchange. Science 317:1554–1557 (80-)
Kawa S, Kitahara K, Hamano H et al (2008) A novel immunoglobulin-immunoglobulin interaction in autoimmunity. PLoS One 3:e1637
Meiler F, Klunker S, Zimmermann M et al (2008) Distinct regulation of IgE, IgG4 and IgA by T regulatory cells and toll-like receptors. Allergy 63:1455–1463
Shamji MH, Ljørring C, Francis JN et al (2012) Functional rather than immunoreactive levels of IgG4 correlate closely with clinical response to grass pollen immunotherapy. Allergy 67:217–226
Nouri-Aria KT, Wachholz PA, Francis JN et al (2004) Grass pollen immunotherapy induces mucosal and peripheral IL-10 responses and blocking IgG activity. J Immunol 172:3252–3259
James LK, Bowen H, Calvert RA et al (2012) Allergen specificity of IgG(4)-expressing B cells in patients with grass pollen allergy undergoing immunotherapy. J Allergy Clin Immunol 130:663.e3–670.e3
Meiler F, Zumkehr J, Klunker S et al (2008) In vivo switch to IL-10-secreting T regulatory cells in high dose allergen exposure. J Exp Med 205:2887–2898
Karagiannis P, Gilbert AE, Josephs DH et al (2013) IgG4 subclass antibodies impair antitumor immunity in melanoma. J Clin Invest 123:1457–1474
Mihai S, Chiriac MT, Herrero-González JE et al (2007) IgG4 autoantibodies induce dermal-epidermal separation. J Cell Mol Med 11:1117–1128
Huijbers MG, Zhang W, Klooster R et al (2013) MuSK IgG4 autoantibodies cause myasthenia gravis by inhibiting binding between MuSK and Lrp4. Proc Natl Acad Sci U S A 110:20783–20788
Klooster R, Plomp JJ, Huijbers MG et al (2012) Muscle-specific kinase myasthenia gravis IgG4 autoantibodies cause severe neuromuscular junction dysfunction in mice. Brain 135:1081–1101
Niks EH, van Leeuwen Y, Leite MI et al (2008) Clinical fluctuations in MuSK myasthenia gravis are related to antigen-specific IgG4 instead of IgG1. J Neuroimmunol 195:151–156
Braganza JM, Jolley JE, Lee WR (1986) Occupational chemicals and pancreatitis: a link? Int J Pancreatol 1:9–19
Maillette de Buy Wenniger LJ, Doorenspleet ME, Klarenbeek PL et al (2013) Immunoglobulin G4+ clones identified by next-generation sequencing dominate the B cell receptor repertoire in immunoglobulin G4 associated cholangitis. Hepatology 57:2390–2398
Mattoo H, Mahajan VS, Della-Torre E et al (2014) De novo oligoclonal expansions of circulating plasmablasts in active and relapsing IgG4-related disease. J Allergy Clin Immunol. doi:10.1016/j.jaci.2014.03.034
Okazaki K, Uchida K, Ohana M et al (2000) Autoimmune-related pancreatitis is associated with autoantibodies and a Th1/Th2-type cellular immune response. Gastroenterology 118:573–581
Aparisi L, Farre A, Gomez-Cambronero L et al (2005) Antibodies to carbonic anhydrase and IgG4 levels in idiopathic chronic pancreatitis: relevance for diagnosis of autoimmune pancreatitis. Gut 54:703–709
Löhr J-M, Faissner R, Koczan D et al (2010) Autoantibodies against the exocrine pancreas in autoimmune pancreatitis: gene and protein expression profiling and immunoassays identify pancreatic enzymes as a major target of the inflammatory process. Am J Gastroenterol 105:2060–2071
Pancreatitis A, Asada M, Nishio A, Uchida K (2006) Identification of a novel autoantibody against pancreatic secretory trypsin inhibitor in patients with autoimmune pancreatitis. Pancreas 33:20–26
Endo T, Takizawa S et al (2009) Amylase alpha-2A autoantibodies: novel marker of autoimmune pancreatitis and fulminant type 1 diabetes. Diabetes 58(3):732–737
Yuki N, Hartung H (2012) Guillain–Barré syndrome. N Engl J Med 366(24):2294–2304
Kountouras J, Zavos C, Chatzopoulos D (2005) A concept on the role of Helicobacter pylori infection in autoimmune pancreatitis. J Cell Mol Med 9:196–207
Guarneri F, Guarneri C, Benvenga S (2005) Helicobacter pylori and autoimmune pancreatitis: role of carbonic anhydrase via molecular mimicry? J Cell Mol Med 9:741–744
Frulloni L, Lunardi C, Simone R et al (2009) Identification of a novel antibody associated with autoimmune pancreatitis. N Engl J Med 361:2135–2142
Mahajan VS, Mattoo H, Deshpande V et al (2013) IgG4-related disease. Annu Rev Pathol. doi:10.1146/annurev-pathol-012513-104708
Park DH, Hwang JY, Kim M-H (2010) A novel antibody associated with autoimmune pancreatitis. N Engl J Med 362:759–760, author reply 760–761
Yamamoto M, Naishiro Y, Suzuki C et al (2010) Proteomics analysis in 28 patients with systemic IgG4-related plasmacytic syndrome. Rheumatol Int 30:565–568
Zen Y, Fujii T, Harada K et al (2007) Th2 and regulatory immune reactions are increased in immunoglobin G4-related sclerosing pancreatitis and cholangitis. Hepatology 45:1538–1546
Moriyama M, Tanaka A, Maehara T et al (2014) T helper subsets in Sjögren’s syndrome and IgG4-related dacryoadenitis and sialoadenitis: A critical review. J Autoimmun 51C:81–88
Tanaka A, Moriyama M, Nakashima H et al (2012) Th2 and regulatory immune reactions contribute to IgG4 production and the initiation of Mikulicz disease. Arthritis Rheum 64:254–263
Kamisawa T, Anjiki H, Egawa N, Kubota N (2009) Allergic manifestations in autoimmune pancreatitis. Eur J Gastroenterol Hepatol 21:1136–1139
Koyabu M, Uchida K, Miyoshi H et al (2010) Analysis of regulatory T cells and IgG4-positive plasma cells among patients of IgG4-related sclerosing cholangitis and autoimmune liver diseases. J Gastroenterol 45:732–741
Uchida K, Kusuda T, Koyabu M et al (2012) Regulatory T cells in type 1 autoimmune pancreatitis. Int J Rheumatol 2012:795026
Wynn TA (2004) Fibrotic disease and the T(H)1/T(H)2 paradigm. Nat Rev Immunol 4:583–594
Vinuesa CG, Tangye SG, Moser B, Mackay CR (2005) Follicular B helper T cells in antibody responses and autoimmunity. Nat Rev Immunol 5:853–865
Khosroshahi A, Carruthers MN, Deshpande V et al (2012) Rituximab for the treatment of IgG4-related disease: lessons from 10 consecutive patients. Medicine (Baltimore) 91:57–66
Lund FE, Randall TD (2010) Effector and regulatory B cells: modulators of CD4+ T cell immunity. Nat Rev Immunol 10:236–247
Kiyama K, Kawabata D, Hosono Y et al (2012) Serum BAFF and APRIL levels in patients with IgG4-related disease and their clinical significance. Arthritis Res Ther 14:R86
Yamanishi H, Kumagi T, Yokota T et al (2011) Clinical significance of B cell-activating factor in autoimmune pancreatitis. Pancreas 40:840–845
Mackay F, Schneider P, Rennert P, Browning J (2003) BAFF AND APRIL: a tutorial on B cell survival. Annu Rev Immunol 21:231–264
Litinskiy MB, Nardelli B, Hilbert DM et al (2002) DCs induce CD40-independent immunoglobulin class switching through BLyS and APRIL. Nat Immunol 3:822–829
Alderlieste YA, van den Elzen BDJ, Rauws EAJ, Beuers U (2009) Immunoglobulin G4-Associated cholangitis: one variant of immunoglobulin G4-related systemic disease. Digestion 79:220–228
Conflict of Interest
Lowiek M. Hubers, Lucas J. Maillette de Buy Wenniger, Marieke E. Doorenspleet, Paul L. Klarenbeek, Joanne Verheij, Erik A. Rauws, Thomas M. van Gulik, Ronald P.J. Oude Elferink, Stan F.J. van de Graaf, Niek de Vries, and Ulrich Beuers declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hubers, L.M., Maillette de Buy Wenniger, L.J., Doorenspleet, M.E. et al. IgG4-Associated Cholangitis: A Comprehensive Review. Clinic Rev Allerg Immunol 48, 198–206 (2015). https://doi.org/10.1007/s12016-014-8430-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12016-014-8430-2