
Abstract
Provide the basis for clinical pathogeny diagnosis and discuss effective ways of curing the youth cerebral infarction in different TOAST classifications through analysis of the correlation between the youth infarction in different TOAST classifications and high homocysteine (Hcy). The selected young patients who diagnosed with cerebral infarction and admitted to the hospital in the past 3 years were regarded as the study group, and the other 136 persons picked accepted health examination in our hospital in the corresponding period were regarded as the control group, then the 136 patients were grouped according to TOAST classification; Hcy levels were determined by enzymatic cycling to compare and analyze, and NIHSS scale is applied to score. Compared with the control group, serum Hcy levels in young patients with cerebral infarction were significantly higher (P < 0.05). The statistical significance in comparative difference was found in the serum Hcy level and NIHSS score of large artery atherosclerotic (LAA) subtype from TOAST classification and the other four subtypes (P < 0.05), but such significance was absent among the other four subtypes (SAA, CA, SOE, SUE). In conclusion, the cerebral etiology of high Hcy is often related to the atherosclerosis and tends to be more serious than the other subtypes after onset of LAA, which requires more clinical attention. Early intervention and therapy are highly necessary specific to cause of disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Infarction, also known as stroke, is one of the most common cerebrovascular diseases, characterized by high incidence, morbidity, and mortality and seriously endangering the health and life of patients. The youth cerebral infarction refers to the ischemic stroke occurred in young people with the age of onset ranging from 18 to 45 years old. Though, its incidence clinically lower than that of the elderly cerebral infarction, it is not uncommon. Worse still, the clinical findings show that the youth cerebral infarction incidence is increasing year by year [1], saddling families and society with great pressure. Unsurprisingly, it is highly needed to carry out more in-depth and full-scale study. With the improvement of the test, many studies have confirmed that the accumulation of homocysteine (Hcy) in the blood vessels can vitiate similar vessel. The high Hcy caused by metabolic disorders of Hcy is an independent risk factor [2] to thrombosis, coronary heart disease, atherosclerosis and other cardiovascular and cerebrovascular. In recent years, there is a growing emphasis on research of high Hcy. TOAST classification of cerebral infarction functions diversely to the cerebral infarction etiology, severity of disease, and prognosis [3]. The correlation shared by TOAST classification and high Hcy needs further study.
This study selected young patients who diagnosed with cerebral infarction and admitted to the hospital in the past 3 years as the study grand and picked the other 136 persons who accepted health examination in our hospital in the corresponding period as the control group; the 136 patients were grouped according to TOAST classification; Hcy levels were determined by enzymatic cycling to compare and analyze, and NIHSS scale is applied to score, with the purpose of discussion of the high Hcy being an important risk factor for cerebral infarction, analysis of the correlation between different TOAST subtypes and high Hcy, and providing basis for analysis of clinical etiology, treatment, and prognosis. The report is as follows.
Information and Methods
General Information
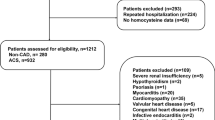
We have selected 136 young patients diagnosed with cerebral infarction and admitted to the hospital in the past 3 years, including 74 males and 62 females with age between 20 and 43 years old and mean age in 32.3 ± 4.7 years old. All the patients are in line with the diagnostic criteria [4] of infarction set by China Society for Neuroscience in 2010, namely (1) acute onset; (2) focal neurological defects while a small number of patients with comprehensive neurological defects; (3) signs and symptoms for continuous hours or more; (4) brain CT or MRI excluding cerebral hemorrhage and other diseases; (5) brain CT or MRI showing responsibility infarction lesions. We have also selected the control group composed of 136 persons who have accepted health examination in our hospital in the same period, and grouped the 136 youths suffered from cerebral infarction according to TOAST classification, who have no high blood pressure, high cholesterol, and other medical history. Determination of Hcy level was performed by enzymatic cycling to get contrastive analysis. Besides, NIHSS scale was put into use to score. The age, gender, years of education in these two groups have no statistical differences (P > 0.05) compared with the study group, so they are of comparability. The study was approved by the hospital ethics committee, and informed consents were signed by all the subjects.
Methods
At 7–8 o’clock in the morning, vacuum blood collection tubes were took to draw 5 mL venous blood on an empty stomach from the two groups; the blood drawn was processed at 4 °C for 30 min of centrifugation, and the upper serum took was stored at −20 °C in the refrigerator to be tested. Hitachi 7170 automatic biochemical analyzer and related reagents coupled with enzymatic cycling [5] were employed to detect serum Hcy levels, in strict accordance with the operational requirements. The normal range of serum Hcy reference values is 5–15 μmol/L. The serum higher than 15 μmol/L is seen as high Hcy. All cases were classified in accordance with TOAST classification. NIHSS was applied to score within 3 days after getting ill.
Statistical Methods
Adoption of SPSS 15.0 statistical software for statistical treatment, measurement data denoted by the mean ± standard deviation (x ± s), comparison among groups tested by t. P < 0.05 is considered statistically significant.
Results
Comparison of Patient’s Hcy Level in the Study Group and the Control Group
Hcy from the study group increased markedly (P < 0.05) with statistical significance, compared with the control group. See Table 1.
Proportion of TOAST Subtypes and Comparison of Hcy Levels from the Study Group and the Control Group
Among the 136 of young patients with cerebral infarction TOAST subtypes, SAA took up the highest proportion, large artery atherosclerotic (LAA) followed; LAA subtype, compared with the other four subtypes, increased significantly in its serum Hcy levels (P < 0.05). There was no significant difference (P > 0.05) between any two subtypes from the other four subtypes. See Table 2.
Comparison of NIHSS Score for TOAST Subtypes from the Study Group
Among the 136 of young patients with cerebral infarction TOAST subtypes, LAA subtype was highest in NIHSS score compared with the other four subtypes, and has a significant difference (P < 0.05). There was no significant difference (P > 0.05) between any two subtypes from the other four subtypes. See Table 3.
Discussion
Frequently used in international classification of cerebrovascular disease, TOAST classification is simple in operation, high in reliability, and suitable for clinical studies. In 2010, it was applied in the Diagnosis and Treatment Guideline of Acute Ischemic Stroke. TOAST classification focuses on the analysis of pathogenesis of cerebral infarction. Based on clinical manifestations, neuroimaging, and other laboratory examinations, ischemic stroke can be divided into five types, LAA, small artery occlusion or lacunar stroke (SAA), cardioembolism (CE), stroke of other determined etiologies (SOE), and stroke of undetermined etiologies (SUE). Studies have shown [6] that hypertension, hyperlipidemia, diabetes, heart disease, alcohol consumption, and smoking are the common risk factors responsible for young cerebral infarction.
Serum Hcy synthesized by the liver is a sulfur-containing amino acid generated during methionine metabolism. Under normal circumstances, fasting serum Hcy level is 5–15 μmol/L; when elevated above the reference range, it is known as high Hcy. Many studies have shown that increase in Hcy levels is one of the causes leading to stroke, accompanied by increase in the incidence of cerebral infarction and atherosclerosis. More peroxide and oxygen free radicals produced in the metabolic process of hyperhomocysteinemia have a strong toxic effect to the endothelial cells, and can indirectly lower the ability of cells to eliminate superoxide, thus resulting in infarction. High Hcy expedites the proliferation of smooth muscle cells, thus initiates atherosclerosis and vascular spasm, enhances platelet aggregation, promotes the formation of fibrinogen, affects blood clotting condition, leading to the occurrence of angiosis [7]. NIHSS score is a scale commonly used in international infarction severity with extensive and detailed content. The scale includes nervous system items to be checked specific to possible symptoms and signs of cerebral artery disease and before and after circulation. The items involved are 13 in total. Higher scores mean higher severity.
This paper studied the relations of serum Hcy levels and the youth cerebral infarction TOAST classification, analyzed multiple types and speculated potential causes, providing the basis for clinical diagnosis of cerebral infarction etiology; furthermore, NIHSS score of TOAST subtypes was also observed. So as to give a more accurate clinical speculation.
The mechanism of high Hcy resulting in damages on artery and cerebral infarction is may be like this: High Hcy increases the expression of cell adhesion molecule and chemokine, thus inducing atherosclerosis; increases the synthesis of thromboxane A2, thus creating blood clots; promotes oxygen free radicals so that the nitric oxide synthase activity in the vascular endothelial cells is decreased, thrombomodulin expression is inhibited, causing damage and toxic effects on vascular endothelial cells and formation of thrombus [8]; accelerates proliferation of vascular smooth muscle cells, leading to occurrence of atherosclerosis and thrombosis. In addition, high Hcy can also speed up lipid deposition in the arterial wall and increase the foam cells to change the fibrosis structure of glycoprotein molecules in the arterial wall and add calcified plaque, thereby undermining the elasticity of blood vessels. Accumulation of blood platelet in the place where the endothelial cells are damaged produces the thrombus [9].
The study has proved that the youth cerebral infarction patients are notably higher than healthy people in Hcy levels. It is hinted that increase in levels of Hcy may cause aggravation of atherosclerosis, that high Hcy is one of the risk factors for cerebral infarction, and Hcy levels and NIHSS scores of LAA subtype are significantly higher than the other four subtypes, possessing statistical significance and more consistent with previous studies [10], which indicates that the neurological function of patients diagnosed with LAA is more serious than the other types. It is predicted that the combined high Hcy will be more serious, calling for more attention for early intervention and treatment. There are many factors to be responsible for the youth cerebral infarction. The research in the etiology and pathogenesis is conducive to finding more effective curing ways and achieving better therapeutic effects. This study creates the basis for the clinical diagnosis of the youth cerebral infarction etiology, contributing to discussing effective ways of curing the youth cerebral infarction in different TOAST classifications.
References
Liu, C., & Du, Y. (2013). The correlation between risk factors for young adults cerebral infarction and TOAST subtype. NingXia Medical Journal, 35(8), 687–688.
Liu, X. (2013). The correlation between hyperhomocysteinemia and cerebral infarction. Journal of Practical Medical Techniques, 20(6), 640–641.
Zhang, C., & Xie, B. (2011). The relationship of cerebral infarction in TOAST subtype with homocysteine and NIHSS scoring. Guangdong Medical Journal, 32(18), 2443–2445.
Cerebrovascular Epidemiology Group of the Psychiatry Branch Affiliated to the Chinese Medical Association. (2010). Guideline for the China’s acute ischemic stroke. Chinese Journal of Neurology, 43(2), 2–3.
Zhang, Q., Yu, W., Zhu, L. J., et al. (2013). The correlation of hyperhomocysteinemia and cerebral infarction. Chinese Journal of Medicinal Guide, (7), 1168-1169.
Wang, Y., Lu, Z., Zhang, Q., et al. (2010). Analysis of risk factors for the chinese youth cerebral apoplexy. Chinese General Practice, 13(3), 254–2010.
Qi, J. (2013). Clinical analysis of hyperhomocysteinemia and cerebral infarction. Medical Journal of Chinese People’s Health, 25(8), 29.
Jiang, L. (2013). Relationship of cerebral apoplexy and hyperhomocysteinemia. Chinese Journal of Practical Medicine, 40(1), 87–88.
Wang, H., Zhang, S., & Zhang, S. (2010). Analysis of homocysteine concentrations of cerebrovascular disease and correlation factors. NingXia Medical Journal, 32(1), 65–66.
Wozniak, M. A., Kittner, S. G., Tuhrim, S., et al. (2010). Frequeney of unrecognized Fabry disease among young European-American and African-American men with first ischemic stroke. Stroke, 41(1), 78–81.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zhang, W., Zhang, X. Correlation Between the Youth Cerebral Infarction in Different TOAST Classifications and High Homocysteine. Cell Biochem Biophys 71, 39–42 (2015). https://doi.org/10.1007/s12013-014-0159-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12013-014-0159-2