
Abstract
The increase in the prevalence of metabolic disorders globally is becoming a public health concern. Previous studies have reported an association between environmental exposures to hazardous substances, including various heavy metals, and the risk for metabolic syndrome. However, reports on the contributions of cadmium (Cd) to the risk for obesity and diabetes remain inconsistent. This study aims to investigate an association between serum Cd levels (SCL) and diabesity and dyslipidemia risk scores. A total of 140 subjects were identified from a public academic institution in Lebanon. Socio-demographic information, diabesity, and obesity risk scores were determined using an interview-based adapted FINDRISC questionnaire and analysis of an acquired blood sample. SCL was quantified using inductively coupled plasma mass spectrometry (ICP-MS). The statistical analysis relied on a chi-squared test and multivariate logistic regression models, along with checks for confounders and effect modifiers. Our results showed a Cd geometric mean of 4.04 μg/L (± 2.5). High SCL was significantly associated with higher dyslipidemia risk (OR: 3.05 [95% CI: 1.19–7.86], P = 0.02), even after adjusting for confounders. However, SCL did not show a statistically significant association with diabetes and obesity outcomes. Elevated SCL increases the risk of dyslipidemia and alters the blood lipid profile. In addition, our findings do not support a role for Cd in diabesity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity is characterized by an increase in adipose tissue mass and adipocyte dysfunction [1] and is mainly associated with increased oxidative stress [2], endoplasmic reticulum stress [3], production of pro-inflammatory adipokines [4,5,6], and insulin resistance [7]. In addition, alterations in lipid metabolism are highly prevalent in obese subjects. About two thirds of patients with obesity are found to be dyslipidemic [8]. Lipid abnormalities in obese patients include elevated serum triglyceride and VLDL levels, non-HDL cholesterol levels, and apolipoprotein B [9]. On the other hand, type II diabetes mellitus (T2DM), accounting for 90% of all diabetics, is characterized by hyperglycemia caused by either low insulin levels or insulin resistance [10]. The interaction between T2DM and obesity is what is known as diabesity, a common metabolic disorder [11, 12]. In diabesity patients, both diabetes and obesity are connected by various pathophysiological mechanisms revolving around insulin disorders [13].
Several studies have reported an association between environmental exposures to hazardous substances and diabesity [14,15,16,17,18]. Various heavy metals and metalloids are reported to play a role in metabolic syndromes pathophysiology [18]. For instance, arsenic exposure was positively associated with fasting glucose levels in 1047 subjects selected from American Indian communities [19]. In addition to arsenic, exposure to cadmium and lead were associated with higher blood pressure [20,21,22]. Furthermore, studies proposed evidence of a gene-environment interaction that may be underlying the development of these metabolic syndromes [23].
Of particular interest is Cadmium (Cd), a naturally occurring trace element and an anthropogenic pollutant arising from fossil fuel combustion, improper solid waste disposal and wastewater management, excessive use of phosphate fertilizers in agricultural settings, industrial effluents, and tobacco smoking [24]. The public health concerns with Cd mainly revolve around its persistence in the environment and high bioaccumulation, and its toxic effects in humans [25]. Cd is classified as an endocrine disruptor with toxic effects at relatively low human exposure levels, and may lead to renal damage and anemia, bone disease and disturbances in calcium metabolism, and lung cancer [26]. Moreover, human exposure to Cd was reported as a potential risk factor for diabetes and dyslipidemia [13, 27]. For instance, evidence suggest that chronic Cd exposure impairs the function of insulin-producing β-cells and may lead to T2DM [28]. However, findings on the contribution of Cd in increasing the risk of diabesity and dyslipidemia remain inconsistent.
Lebanon, an Eastern Mediterranean middle-income country, is characterized by heavy traffic, increased pollution associated with improper waste management, abuse of fertilizers and pesticides, fossil fuel power plants, and prevalent diesel-based domestic generators. Previous studies showed mobile forms of heavy metals, including Cd, polluting groundwater [29]. Recently, a study revealed an unusually elevated Cd health risk compared with global rates and reported multiple polluting sources contributing to the observed Cd health risk [30]. This study aims to investigate an association between serum Cd level (SCL) and the risk of diabesity and dyslipidemia in a Lebanese population.
Materials and Methods
Study Population and Data Collection
The study followed a cross-sectional design. Participants already diagnosed with diabetes, subjects under 35 and pregnant women were excluded from the study. A total of 461 participants were enrolled from faculty members and staff of a public academic institution located in the capital city Beirut. Among these 461 participants, 301 who did not provide blood samples for biochemical analyses and 20 who had missing responses on the questionnaires were excluded from the analysis. A total sample of 140 adult subjects was eligible for analyses. An Institutional Review Board approval was obtained from the Lebanese University and the Ain Wazein Hospital in compliance with the Helsinki Declaration; all participants provided a written consent prior to enrollment. An adapted FINDRISC questionnaire was administered by trained dietitians in native Arabic, using a face-to-face interview from November 2017 to July 2018. A campaign was planned at a booth in each of the faculties visited on campus to invite eligible people to actively participate in the study and to complete the questionnaire. Collected data included socio-demographic characteristics, medical history, diet and exercise, smoking habits, and info on self-reported indicators of diabetes: frequent urination, tingling and numbness in legs and arms, and other indicators.
Obesity Indicators Assessment
In order to assess obesity, body weight, height, and waist circumference were measured for each enrolled subject using a balance and a tape meter on site. The waist circumference was measured around the abdomen at the level of the umbilicus (belly button). The body mass index (BMI) was computed as the ratio of body weight (Kg) to the height squared (m2).
Blood Analysis for Dyslipidemia and Hyperglycemia
Systolic and diastolic blood pressure and heart rate were measured for all enrolled subjects by a trained nurse. In addition, 5 ml of venous blood samples were drawn after an overnight fast in order to screen for dyslipidemia and measure the fasting blood glucose levels. Then, subjects received 75 grams of glucose and blood samples were withdrawn again after 2 h in order to conduct the oral glucose tolerance test. Briefly, collected blood samples were centrifuged, then 0.5 ml was used for the automated biochemical analysis using Cobas C111 machine (Roche Diagnostics, Indianapolis). The remaining volume was then stored at −20 °C until metal analysis was performed.
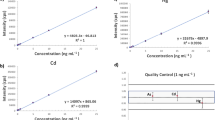
Serum Cd Levels (SCL) Digestion and Quantification
For each collected sample, 0.5 mL of serum blood was mixed with 2 mL of nitric acid (65%, v/v) and 1 mL of hydrogen peroxide (30%, v/v). Samples were then heated at 90 °C on a hot plate for 2 h duration and concentrated by volume reduction to reach 1 ml. Charring of the samples was avoided in order to minimize the possibility of analytic loss. Mineralization was considered complete when the cooled solution was colorless or slightly pale yellow. After cooling, the flasks were rinsed with deionized water to reach a 3 ml final volume. Inductively coupled plasma mass spectrometric (ICP-MS) was then used to quantify Cd levels on an Agilent 7500c ICP-MS (Santa Clara, CA, USA) with a Cetac Auto-sampler and an Octapole Reaction System (ORS). The ORS was pressurized with helium in collision mode for the determination of Cd. Isotopes and integration time per point used for the optimization experiment for cadmium was m/z = 111 a.m.u and 0.1 s/point.
Quality Assurance and Quality Control (QA/QC)
All solutions were prepared using deionized water. All the laboratory ware (transfer pipettes, centrifuge tubes, plastic bottles, vials and glassware material) was cleaned prior to use by soaking in HNO3 (1%) reagent grade (AnalaR NORMAPUR®) for at least 1 h and rinsing one time with deionized water. The auto sampler was washed and purged prior to running blanks in order to avoid cross contamination. A blank was run for every batch of samples. Blank solutions were prepared with 2-ml nitric acid and 1-ml hydrogen peroxide. About 10% of the samples in addition to blank solutions were spiked with 2 ppb (0.6 μl) Cd from a standard solution (multi-element solution 1, Absolute Standards Inc., Connecticut) in order to validate the method and determine Cd percent recovery. All plastics used for analysis were rinsed twice with distilled water prior to usage. Measurements were conducted triplicates per sample for quality control, and the average Cd concentration was reported. All instrumental parameters were optimized daily while aspirating the tuning solution.
Statistical Analysis
Data was analyzed using the Statistical Package for Social Sciences (version 23.0; SPSS, Chicago, IL, USA). All continuous variables were presented as mean (M), and 95% confidence interval, while categorical variables were presented as frequencies and percentages. Tested independent variables included serum cadmium, age, gender, smoking status, family history of diabetes, waist circumference, history of high blood sugar, physical activity, vegetable consumption, and anti-hypertensive medication. Outcome variables included diabetes, obesity/overweight, and dyslipidemia. A subject was considered as “diabetic” following the diagnostic criteria recommended by the American Diabetes Association, when having a fasting blood glucose levels ≥ 5.6 mmol/L or an oral glucose tolerance test (OGTT) ≥ 7.8 mmol/L or both [31]. Thus, according to this criterion, not only persons with diabetes but also persons with prediabetes were included in this group. A subject was considered as “normal” or “overweight” or obese when BMI measures were found to be < 25, between 25 and 29.9, and ≥ 30 kg/m2, respectively [32]. Dyslipidemia was defined as having one or more of the following indicators: total cholesterol (TC) ≥ 6.22 mmol/L (≥ 240 mg/dL), triglycerides (TG) ≥ 1.70 mmol/L (≥ 150 mg/dL), LDL cholesterol ≥ 4.14 mmol/L (≥ 160 mg/dL), and/or HDL cholesterol < 1.04 mmol/L (< 40 mg/dL) [33]. For obesity, a subject was classified as follows: underweight (< 18.5 kg/m2), normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), or obese (≥ 30.0 kg/m2) [34]. In addition, waist circumference was labeled as “normal” if < 102 cm for men and < 88 cm for women [34]. On the other hand, SCL were classified into two categories, “low” (≤ 5 μg/L) and “high” (> 5 μg/L) [35]. A subject was labeled as a “current smoker” if he had smoked at least 100 cigarettes in his lifetime and is still smoking cigarettes at the time of data collection. Student’s t test and ANOVA (for parametric test), or Mann- Whitney U and Kruskal-Wallis tests (for nonparametric test), were applied to compare continuous data in various groups. Logistic regression models were used to investigate the association between SCL diabetes, obesity/overweight and dyslipidemia. Models were performed for the overall population and then stratified by age, smoking status, gender, BMI, smokers, family history of diabetes, blood sugar history, physical activity, vegetable consumption, and anti-hypertensive medication categories. Odds ratios, p values, and 95% confidence intervals were computed; a p value < 0.05 was considered statistically significant. The final multivariate model incorporated exposures and confounding variables that showed significance in the bivariate models.
Results
Characteristics of Study Population and their Association with SCL
This study included 140 adults aged 35 or older; their socio-demographic characteristics are presented in Table 1. The study group had a mean age of 47.3 years, a mean BMI of 27.28 kg/m2, a mean waist circumference of 97.23 cm, and a geometric mean serum cadmium level of 4.04 μg/L. Moreover, 51.4% of the study population was non-smokers. In addition, the prevalence of diabetes, overweight/obesity, and dyslipidemia were 36.4, 66.4, and 84.3%, respectively.
Bivariate Analysis for SCL in Diabesity and Dyslipidemia
When testing for the association between diabetes and SCL, no significant association between the two variables was observed (OR: 0.854 [95% CI: 0.425–1.718], p = 0.66) (Fig. 1). In addition, in all-stratified models, no associations were found between diabetes and SCLs (Fig. 1). Similarly, SCL was not found to be significantly associated with obesity and so did the different risk factors and confounders tested (OR: 0.860 [95% CI: 0.425–1.718], p = 0.66) (Fig. 2). However, elevated SCL were significantly associated with a higher dyslipidemia risk (Fig. 3). The odds of dyslipidemia were found to be three times higher for subjects with high SCL (> 5 μg/L) compared with those with low SCL (≤ 5 μg/L) (OR: 3.05 [95% CI: 1.19–7.86], p = 0.02). In age-stratified models, the risk of dyslipidemia was significantly 6 times higher for subjects with high SCL compared with subjects with low SCL among patients aged between 41 and 60 years (OR: 5.98 [95% CI: 1.15-–31.14], p = 0.03). Similarly, in tobacco-stratified models, the risk of dyslipidemia was 7.7 times higher for subjects with high SCL compared with those with low SCL among those who are current smokers (OR: 7.67 [95% CI: 1.35–43.7], p = 0.02). Among those that do physical activity, those that have high SCL have higher risk of dyslipidemia compared with those that have low SCL (OR: 5.13[95% CI: 1.43-18.37], p = 0.01). In anti-hypertensive medication stratified models, the risk of dyslipidemia was 3.5 times higher for subjects with high SCL compared with subjects with low SCL among patients not taking anti-hypertensive medications (OR: 3.5 [95% CI: 1.11–10.92], p = 0.03).

Logistic regression analysis examining the association between diabetes and SCL and odds ratios with 95% confidence intervals, while adjusting for age, gender, smoking status, family history of diabetes, history of hyperglycemia, physical activity, vegetable consumption, and BMI

Logistic regression analysis examining the association between obesity and SCL and odds ratios with 95% confidence intervals while adjusting for physical activity, vegetable consumption, and smoking status

Logistic regression analysis examining the association between dyslipidemia and SCL and odds ratios with 95% confidence intervals while adjusting for age, gender, smoking status, physical activity, vegetable consumption, BMI score, and anti-hypertensive medication. Statistically significant tests are indicated (*p value < 0.05).
Multivariate logistic Regression Analysis
When testing the association between SCL and dyslipidemia, the risk of dyslipidemia remained significantly higher for patients with high SCL compared with those with low SCL, even after adjusting for age, smoking status, physical activity, and anti-hypertension medication (OR: 3.14 [95% CI: 1.19–8.28], p = 0.02) (Table 2).
Discussion
Cd is a widespread environmental and occupational pollutant that accumulates in the human body with a biological half-life of 20–30 years and may cause a number of diseases [36]. Our results show a higher SCL geometric mean (4.04 μg/L) compared with reported levels in other populations, including middle-aged and elderly Caucasians (0.49 μg/L) [37], adult French smokers (0.86 μg/L) [38], and Korean e-cigarette smokers (0.91 μg/L) [39]. In addition, our studied population showed higher SCL than those reported in a group of Chinese smelting workers with relatively higher occupational exposure to Cd (3.61 μg/L) [33].
Our findings also suggest that subjects with elevated SCL have an almost threefold higher dyslipidemia risk. These results are consistent with other studies in the literature [33, 40]. For instance, a study on a group of about 1500 Chinese workers from seven Cd smelting factories in China showed that workers with elevated SCL were more prevalent among dyslipidemics compared to non-dyslipidemics (OR:1.83, 95% CI 1.32–2.28) [33]. In addition, the prevalence of dyslipidemia followed a dose-response relationship, increasing with elevations in SCL [33]. On the other hand, our results are supported by bioassays in experimental animals. In one study, the exposure of zebrafish to CdCl2 caused a remarkable hyperlipidemia and fatty liver changes, via enhancement of cholesteryl ester transfer protein (CETP) activity [41]. Dyslipidemia is known to be a major independent risk factor for cardiovascular diseases. Although there is a scarcity in studies linking SCL and dyslipidemia, evidence does support an association between SCL and cardiovascular diseases, a possible outcome of dyslipidemia [42]. Elevated cardiovascular disease incidence was found to be associated with Cd exposure in several populations, including Native Americans, Europeans, and US populations [43,44,45]. Cd is also thought to have a diabesigenic effect and may induce hyperglycemia [46, 47]. In vivo studies show that rats exposed to Cd show a reduction in serum insulin levels and a direct Cd-induced damage on insulin-producing cells [28, 35]. Epidemiological studies are also in support of this hypothesis. For instance, each 0.1 μg/L incremental increase in the SCL was found to be associated with a 0.0032 g/L significant increase in blood sugar among French Caucasian smokers [38]. However, in our study, no statistically significant relationships were found between SCL and each of Type II Diabetes (T2DM) and obesity in consistence with similar other studies in the literature [46]. T2DM is a multifactorial disease with modifiable factors such as increased body weight and waist circumference, and other non-modifiable predisposing factors such as genetics and age [48]. These factors may be influencing the examined association with SCL. This is supported by our findings on the association with first degree family history. On the other hand, although many studies found that smoking increases the risk of diabetes [49, 50], likewise in a recent study using a biomarker of diabetes (HbA1c), an association was found between diabetes and smoking status since HbA1c levels were higher in current smokers than in former smokers (by 0.14 percentage points) and in never smokers (by 0.18 percentage points) [38]. These results were not in agreement with our results, since no significant correlation was found between smoking and diabetes in our study population.
Metabolic syndromes are complex conditions with significant variability among their associated symptoms across ethnicities, developmental stages, and gender, making it challenging to examine in epidemiological studies, particularly when attempting to identify underlying exposures. The underlying pathogenic mechanism of metabolic alterations induced by Cd exposure is not fully understood yet. Our study attempted to focus on three interrelated metabolic disorders. One of the main mechanisms by which Cd exerts its toxic action is oxidative stress, indirectly leading to accumulation of reactive oxygen species (ROS) and free radicals, mainly by weakening enzymatic and non-enzymatic antioxidative pathways [51]. Cd-induced alterations in lipid metabolism in the liver is mediated by increased oxidative stress and generation of ROS [52]. Cd has high affinity to sulfhydryl groups and, hence, may deplete cellular antioxidants such as glutathione (GSH), superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (Gpx) in soft tissues [53]. Interestingly, a study showed that the co-administration of virgin coconut oil polyphenol—a known antioxidant—restores lipid profile and cardiovascular risk ratios in rats exposed to Cd and stabilizes antioxidant defense systems to levels comparable to control groups, particularly at the level of the hepatic activities of SOD, CAT, and GSH [54]. In addition, many inflammatory biomarkers, released in response to Cd exposure, were detected in various diseases, with some associated with dyslipidemia such as atherosclerosis and cardiovascular diseases [51]. On the other hand, evidence on the endocrine disruptive ability of Cd is accumulating. In a recent study, men exposed to Cd showed a significant decrease in testosterone levels and in the sex hormone binding globulin, hence adversely affecting the male reproductive function [55]. Cd is also genotoxic, mainly in its capacity to damage DNA and inhibit DNA repair enzymes, as well in influencing gene expression through epigenetic mechanisms [51, 56].
Several limitations could have affected our findings. First, the sample is relatively small and is not representative of the general population. Future studies should target a larger and a more representative population to conduct the analysis. Second, collected data is based on self-reporting; hence a recall bias cannot be excluded. We tried to overcome this limitation by selecting a short recall period for self-reported information, combined with biomarkers and medical testing for our main exposures and outcomes of interest. In addition, Cd was measured in blood, rather than urine, which could be reflecting a recent or continuous exposure, rather than a chronic exposure [57]. However, given the very long half-life of Cd in the kidneys, urine Cd concentrations would have also reflected stored Cd in the kidneys, rather than a repeated exposure.
Conclusion
In summary, our findings highlight an association between SCL and dyslipidemia. Mechanistic studies need to be conducted to further examine this finding. On the other hand, our study is the first report assessing the association between SCL and diabesity in a Lebanese population. Our results indicate that SCL is highly elevated in the target population compared to other populations and ethnic groups. Unlike other studies where high SCL was reported in groups with rather an occupational exposure, our study conducted in subjects selected from the general population gains particular value, in identifying adverse outcomes associated with Cd based on an environmental exposure. Our data do provide decision-makers with reliable guidance in order to mitigate pollution and contamination levels and develop appropriate management programs and policies at the national level, particularly aiming to reduce Cd exposure.
Data Availability
The data set used and analyzed during the current study is available from the corresponding author based on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- °C:
-
Degrees celsius
- WC:
-
Waist circumference
- Bp:
-
Blood pressure
- FINDRISC:
-
Finnish Diabetes Risk Score
- FBG:
-
Fasting blood glucose
- OGTT:
-
Oral glucose tolerance test
- HDL:
-
High-density lipoprotein
- LDL:
-
Low density lipoprotein
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- Cd:
-
Cadmium
- SCL:
-
Serum cadmium level
- ICP-MS:
-
Inductively plasma mass spectrometry
- MetS:
-
Metabolic syndrome
- T2DM:
-
Type 2 diabetes mellitus
- SD:
-
Standard deviation
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- NCD:
-
Non-communicable disease
- ROS:
-
Reactive oxygen species
References
Hajer GR, Van Haeften TW, Visseren FLJ (2008) Adipose tissue dysfunction in obesity, diabetes, and vascular diseases. Eur Heart J 29:2959–2971. https://doi.org/10.1093/eurheartj/ehn387
Furukawa S, Matsuda M, Furukawa S et al (2017) Increased oxidative stress in obesity and its impact on metabolic syndrome find the latest version : increased oxidative stress in obesity and its impact on metabolic syndrome. J Clin Invest 114:1752–1761. https://doi.org/10.1172/JCI200421625.1752
Ozcan U, Cao Q, Yilmaz E et al (2004) Endoplasmic reticulum stress links obesity, insulin action, and type 2 diabetes. Science 306:457–461. https://doi.org/10.1126/science.1103160
Fantuzzi G (2005) Adipose tissue, adipokines, and inflammation. J Allergy Clin Immunol 115:911–919. https://doi.org/10.1016/j.jaci.2005.02.023
Weisberg SP, McCann D, Desai M et al (2003) Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest. 112:1796–808. https://doi.org/10.1172/JCI200319246
Wellen KE, Hotamisligil GS (2003) Obesity-induced inflammatory changes in adipose tissue find the latest version : Obesity-induced inflammatory changes in adipose tissue. J Clin Invest 112:1785–1788. https://doi.org/10.1172/JCI200320514.Obesity
Maury E, Brichard SM (2010) Adipokine dysregulation, adipose tissue inflammation and metabolic syndrome. Mol Cell Endocrinol 314:1–16. https://doi.org/10.1016/j.mce.2009.07.031
Elmaoğullari S, Tepe D, Uçaktürk SA et al (2015) Prevalence of dyslipidemia and associated factors in obese children and adolescents. J Clin Res Pediatr Endocrinol. https://doi.org/10.4274/jcrpe.1867
Klop B, Elte JWF, Cabezas MC (2013) Dyslipidemia in obesity: mechanisms and potential targets. Nutrients 5:1218–1240. https://doi.org/10.3390/nu5041218
Hull RL, Westermark GT, Westermark P, Kahn SE (2004) Islet amyloid: a critical entity in the pathogenesis of type 2 diabetes. J Clin Endocrinol Metab 89:3629–3643. https://doi.org/10.1210/jc.2004-0405
Tinkov AA, Filippini T, Ajsuvakova OP et al (2017) The role of cadmium in obesity and diabetes. Sci Total Environ 601–602:741–755. https://doi.org/10.1016/j.scitotenv.2017.05.224
Danaei G, Finucane MM, Lin JK et al (2011) National, regional, and global trends in systolic blood pressure since 1980: Systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5·4 million participants. Lancet 377:568–577. https://doi.org/10.1016/S0140-6736(10)62036-3
Schmidt MI, Duncan BB (2003) Diabesity: an inflammatory metabolic condition. Clin Chem Lab Med 41:1120–1130. https://doi.org/10.1515/CCLM.2003.174
Madrigano J, Baccarelli A, Wright RO et al (2010) Air pollution, obesity, genes and cellular adhesion molecules. Occup Environ Med 67:312–317. https://doi.org/10.1136/oem.2009.046193
Andersen ZJ, Raaschou-Nielsen O, Ketzel M et al (2012) Diabetes incidence and long-term exposure to air pollution: a cohort study. Diabetes Care 35:92–98. https://doi.org/10.2337/dc11-1155
Bertoli S, Leone A, Battezzati A (2015) Human Bisphenol A Exposure and the “Diabesity Phenotype”. Dose-Response 13:1559325815599173. https://doi.org/10.1177/1559325815599173
Edwards JR, Prozialeck WC (2009) Cadmium, diabetes and chronic kidney disease. Toxicol Appl Pharmacol 238:289–293. https://doi.org/10.1016/j.taap.2009.03.007
Planchart A, Green A, Hoyo C, Mattingly CJ (2018) Heavy metal exposure and metabolic syndrome: evidence from human and model system studies. Curr Environ Health Rep 5:110–124
Spratlen MJ, Grau-Perez M, Best LG et al (2018) The association of arsenic exposure and arsenic metabolism with the metabolic syndrome and its individual components: prospective evidence from the strong heart family study. Am J Epidemiol 187:1598–1612. https://doi.org/10.1093/aje/kwy048
Abhyankar LN, Jones MR, Guallar E, Navas-Acien A (2012) Arsenic exposure and hypertension: a systematic review. Environ Health Perspect 120:494–500. https://doi.org/10.1289/ehp.1103988
Navas-Acien A, Schwartz BS, Rothenberg SJ et al (2008) Bone lead levels and blood pressure endpoints: a meta-analysis. Epidemiology 19:496–504. https://doi.org/10.1097/EDE.0b013e31816a2400
Franceschini N, Fry RC, Balakrishnan P et al (2017) Cadmium body burden and increased blood pressure in middle-aged American Indians: the Strong Heart Study. J Hum Hypertens 31:225–230. https://doi.org/10.1038/jhh.2016.67
Eze IC, Schaffner E, Foraster M et al (2015) Long-term exposure to ambient air pollution and metabolic syndrome in adults. PLoS One 10:1–19. https://doi.org/10.1371/journal.pone.0130337
Ashraf MW (2012) Levels of heavy metals in popular cigarette brands and exposure to these metals via smoking. Sci World J 2012. https://doi.org/10.1100/2012/729430
Wolman A (1985) Public health and environment. Am J Public Health 75:1049–1051. https://doi.org/10.2105/AJPH.75.9.1049
Cabral M, Toure A, Garcon G et al (2015) Effects of environmental cadmium and lead exposure on adults neighboring a discharge: evidences of adverse health effects. Environ Pollut 206:247–255. https://doi.org/10.1016/j.envpol.2015.06.032
Farag YMK, Gaballa MR (2011) Diabesity: an overview of a rising epidemic. Nephrol Dial Transplant 26:28–35. https://doi.org/10.1093/ndt/gfq576
El Muayed M, Raja MR, Zhang X et al (2012) Accumulation of cadmium in insulin-producing β cells. Islets 4:405–416. https://doi.org/10.4161/isl.23101
Kassir LN, Lartiges B, Ouaini N (2012) Effects of fertilizer industry emissions on local soil contamination: a case study of a phosphate plant on the east Mediterranean coast. Environ Technol 33:873–885. https://doi.org/10.1080/09593330.2011.601765
Halwani DA, Jurdi M, Abu Salem FK et al (2019) Cadmium health risk assessment and anthropogenic sources of pollution in Mount-Lebanon Springs. Expo Health. https://doi.org/10.1007/s12403-019-00301-3
Standards of Medical Care in Diabetes (2020) Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care 43:S14 LP–S14S31. https://doi.org/10.2337/dc20-S002
Li ZM, Wu ZX, Han B et al (2016) The association between BMI and gallbladder cancer risk: a meta-analysis. Oncotarget 7:43669–43679. https://doi.org/10.18632/oncotarget.9664
Zhou Z, Lu YH, Pi HF et al (2016) Cadmium exposure is associated with the prevalence of dyslipidemia. Cell Physiol Biochem 40:633–643. https://doi.org/10.1159/000452576
World Health Organization (2008) Waist circumference and waist-hip ratio. Rep a WHO Expert Consult. https://doi.org/10.1038/ejcn.2009.139
Faroon O, Ashizawa A, Wright S, et al (2012) Toxicological Profile for Cadmium. Agency for Toxic Substances and Disease Registry (US), Atlanta (GA)
NJDOH (2010) Hazardous Substance Fact Sheet: Cadmium (Cas number: 7440-43-9). New Jersey Dep Heal, pp 3–6. https://www.nj.gov/health/eoh/rtkweb/documents/fs/0305.pdf
Kim J, Garcia-Esquinas E, Navas-Acien A, Choi Y-H (2018) Blood and urine cadmium concentrations and walking speed in middle-aged and older U.S. adults. Environ Pollut 232:97–104. https://doi.org/10.1016/j.envpol.2017.09.022
Trouiller-Gerfaux P, Podglajen E, Hulo S et al (2019) The association between blood cadmium and glycated haemoglobin among never-, former, and current smokers: A cross-sectional study in France. Environ Res 178:108673. https://doi.org/10.1016/j.envres.2019.108673
Lee JW, Kim Y, Kim Y et al (2020) Cigarette smoking in men and women and electronic cigarette smoking in men are associated with higher risk of elevated cadmium level in the blood. J Korean Med Sci 35:e15. https://doi.org/10.3346/jkms.2020.35.e15
Kim K (2012) Blood cadmium concentration and lipid profile in Korean adults. Environ Res 112:225–229. https://doi.org/10.1016/j.envres.2011.12.008
Kim JY, Kim SJ, Bae MA et al (2018) Cadmium exposure exacerbates severe hyperlipidemia and fatty liver changes in zebrafish via impairment of high-density lipoproteins functionality. Toxicol in Vitro 47:249–258. https://doi.org/10.1016/j.tiv.2017.11.007
Emanuelsson F, Nordestgaard BG, Benn M (2018) Familial hypercholesterolemia and risk of peripheral arterial disease and chronic kidney disease. J Clin Endocrinol Metab 103:4491–4500. https://doi.org/10.1210/jc.2018-01058
Nawrot TS, Van Hecke E, Thijs L et al (2008) Cadmium-related mortality and long-term secular trends in the cadmium body burden of an environmentally exposed population. Environ Health Perspect 116:1620–1628. https://doi.org/10.1289/ehp.11667
Tellez-Plaza M, Guallar E, Howard BV et al (2013) Cadmium exposure and incident cardiovascular disease. Epidemiology 24:421–429. https://doi.org/10.1097/EDE.0b013e31828b0631
Barregard L, Sallsten G, Fagerberg B et al (2016) Blood cadmium levels and incident cardiovascular events during follow-up in a population-based cohort of Swedish adults: The Malmo Diet and Cancer Study. Environ Health Perspect 124:594–600. https://doi.org/10.1289/ehp.1509735
Wu M, Song J, Zhu C et al (2017) Association between cadmium exposure and diabetes mellitus risk: a prisma-compliant systematic review and meta-analysis. Oncotarget 8:113129–113141. https://doi.org/10.18632/oncotarget.21991
Treviño S, Waalkes MP, Flores Hernández JA et al (2015) Chronic cadmium exposure in rats produces pancreatic impairment and insulin resistance in multiple peripheral tissues. Arch Biochem Biophys 583:27–35. https://doi.org/10.1016/j.abb.2015.07.010
Wu Y, Ding Y, Tanaka Y, Zhang W (2014) Risk factors contributing to type 2 diabetes and recent advances in the treatment and prevention. 11. https://doi.org/10.7150/ijms.10001
Chang H-C, Wang M-C, Chen M-H et al (2018) the impact of the hazard correlation between risk factors and diabetes. Int J Environ Res Public Health 15. https://doi.org/10.3390/ijerph15102213
Luo J, Rossouw J, Tong E et al (2013) Smoking and diabetes: does the increased risk ever go away? Am J Epidemiol 178:937–945. https://doi.org/10.1093/aje/kwt071
Mezynska M, Brzóska MM (2018) Environmental exposure to cadmium-a risk for health of the general population in industrialized countries and preventive strategies. Environ Sci Pollut Res Int 25(4):3211–3232. https://doi.org/10.1007/s11356-017-0827-z
Senthilkumar T, Sangeetha N, Ashokkumar N (2012) Antihyperglycemic, antihyperlipidemic, and renoprotective effects of Chlorella pyrenoidosa in diabetic rats exposed to cadmium. Toxicol Mech Methods 22:617–624. https://doi.org/10.3109/15376516.2012.714007
Abdel A, El MS, Abdelhamid AO (2012) European Journal of Chemistry. Eur J Chem 3:455–460. https://doi.org/10.5155/eurjchem.3.3.359
Famurewa AC, Ejezie FE (2018) Polyphenols isolated from virgin coconut oil attenuate cadmium-induced dyslipidemia and oxidative stress due to their antioxidant properties and potential benefits on cardiovascular risk ratios in rats. Avicenna J Phytomed 8:73–84
Parikesit D, Mochtar CA, Umbas R, Hamid ARAH (2016) The impact of obesity towards prostate diseases. Prostate Int 4:1–6. https://doi.org/10.1016/j.prnil.2015.08.001
Olszowski T, Baranowska-Bosiacka I, Gutowska I, Chlubek D (2012) Pro-inflammatory properties of cadmium. Acta Biochim Pol 59:475–482
Barregard L, Engstro G (2014) Cadmium exposure and incidence of diabetes ¨ diet and cancer study mellitus - results from the Malmo 9:1–5. https://doi.org/10.1371/journal.pone.0112277
Author information
Authors and Affiliations
Contributions
ZD (conception and design of the project); ZD, NA, HM and MH (acquisition of data) ZD, NA and HM (analysis, interpretation of data and drafting of the article); ZD and HRD (technical input and significant intellectual content); AM (substantial contribution to statistical analyses). All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors do not declare any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ayoub, N., Mantash, H., Dhaini, H.R. et al. Serum Cadmium Levels and Risk of Metabolic Syndrome: A Cross-Sectional Study. Biol Trace Elem Res 199, 3625–3633 (2021). https://doi.org/10.1007/s12011-020-02502-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-020-02502-3