
Abstract
This study aimed to determine Blood Lead Levels (BLL) in schoolchildren 6–14 years old exposed to industrial sources of lead and evaluated the role of socioeconomic condition. A cross-sectional study was conducted in an area likely to be exposed to industrial pollutants in northern Cali (i.e., distance and wind direction) and in a “non-exposed” area. In children in two schools of corresponding study areas, venous samples (5 ml) were collected to determine BLL by graphite furnace absorption spectrometry. Using regression models, we evaluated the association between risk factors to BLL and the effect of modification with variables of socioeconomic condition. We enrolled 350 schoolchildren. Schoolchildren in the exposed area had higher prevalence of BLL of ≥5 μg/dl (44.2 vs. 8.2 %, p = 0.000) than those in non-exposed area. A positive association was found between exposure and BLL of ≥5 μg/dl (prevalence ratios (PR), 6.68; 95 % confidence interval (95 % CI), 3.95, 11.29). Demographic characteristics and socioeconomic condition such as age (PR, 1.45; 95 % CI, 1.03, 2.04), sex (PR, 1.84; 95 % CI, 1.30, 2.60), race (PR, 2.32; 95 % CI, 1.39, 3.89) and socioeconomic position (SEP; PR, 2.02; 95 % CI, 1.35, 3.04) were statistically significant and independently associated with BLL. There was a synergistic interaction between exposure to the industrial zone and SEP for higher BLL (coefficient, 0.80; 95 % CI, 0.17, 1.43). Residence in the northern urban area of Cali exposed to pollutants of an industrial zone is associated to an increased risk of higher BLL, especially among children from low SEC who are at greater risk of exposure and susceptibility.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lead exposure remains as a major health problem among children around the world, mainly in poor communities. According to the US Third National Examination Nutrition Survey (NHANES III) approximately 2.2 % of children 1 to 5 years of age have blood lead levels (BLL) at or above 10 μg/dl [1] while prevalence of BLL of ≥5 μg/dl is found in an estimated 8.8 and 3.0 % in children 1–5 and 6–11 years old, respectively [2]. In Colombia, as in many other developing countries, exposure to lead might be even higher, and some studies have found that approximately 9.5 % of children at 7 years of age have BLL of ≥5 μg/dl [3].
Lead exposure has been associated with adverse health effects in children, including cognitive, behavioral, physical abilities, and neuropsychological development deficiencies [4, 5]. Several studies have reported that BLL even below 10 μg/dl is associated with significant declines in children’s IQ coefficient, and mental and psychomotor development indexes [4–7]. In particular, an average reduction of 2 to 4 points in the IQ has been estimated for each micrograms per deciliter of increase in BLL [8, 9].
According to the Centers for Disease Control and Prevention (CDC), toxic BLL in children are above 10 μg/dl. However, the findings of health effects at levels below 10 μg/dl suggest that the threshold of lead should be lower than 10 μg/dl in order to be safer for human health. For a better understanding and estimation of the burden of disease related with lead exposure, the CDC is considering whether to lower the intervention threshold for lead exposure from 10 to 5 μg/dl [10].
The main sources of lead exposure are paints, water, food, soil, dust, kitchen utensils, and leaded gasoline [11]. Industrial emissions under certain circumstances are also responsible for population exposure to heavy metals, including lead [12]. In many cases, mainly in developing countries, exposure to lead sources is determined by socioeconomic conditions, where people with fewer economic resources are more exposed to lead. Moreover, lower socioeconomic conditions also translate to a greater susceptibility to the health effects from exposure to environmental pollutants. Lower socioeconomic conditions are associated with less access to health services, poor nutritional condition, and psychosocial stress. Both, greater exposure and susceptibility make these lower income groups vulnerable to the health effects of lead exposure. Thus, in some studies in environmental epidemiology, variables of socioeconomic condition have been included not only as potential confounders but also as effect modifiers of causal relationships [13].
In our study site, at northern Cali, Colombia, there is a large industrial zone manufacturing steel, batteries, and metals. Previous reports made by the environmental authority in the area have shown high levels of lead in air (1.77 μg/m3) compared with international standards (NAAQS, 0.15 μg/m3) [14]. But there has been no previous evaluation about the exposure to lead among children living near this industrial zone. Additionally, little is known about how BLL varies in populations exposed to industrial sources of lead and what mechanisms of interaction with other conditions.
This is the first study in Colombia that analyses the complex effects of socioeconomic condition on lead exposure. We determined BLL in schoolchildren living near an industrial zone and evaluated the role of socioeconomic condition to better understand the burden of lead exposure and its effect on the increased susceptibility.
Materials and Methods
A cross-sectional study was carried out among children aged 6–14 years attending two schools in Cali, Colombia. This is the third largest city in the country, with approximately 2.4 million inhabitants, and is located about 1,000 m above sea level, in a tropical dry forest, with an average relative humidity of 73 %. On the northern city limits, there is a large industrial zone of steel, batteries, and metals, where neighborhoods in close proximity are exposed to emissions depending on the prevailing wind direction.
Study Area and Population
We selected one school with a high probability of exposure to the industrial air pollutants; specifically, it is located in northern Cali, less than 2 km away the industrial zone of interest. In addition, a “non-exposed” school was selected, located in southern Cali, more than 12 km away from the industrial zone, and without other sources of industrial emissions. Based on municipal census, the two schools share similar socio-demographic characteristics, including income level or socioeconomic position (SEP), and also comparable traffic flow.
Considered eligible for the study were children who have been attending the selected schools for at least 12 months before the study began and who live in nearby neighborhoods. In particular, for those in the defined exposed area, the household must be located within 3 km from the industrial zone.
Data Collection
Prior to the survey, eligible participants received written information regarding study aims and procedures to be reviewed with their parents/guardians. Parents who signed the written informed consent were interviewed by trained nurses to fill out a questionnaire that included demographic characteristics, socioeconomic and housing conditions, potential sources of lead at home and child’s behaviors known to increase likelihood of exposure to lead. The Human Subjects Research Committee at the University of Valle approved this study.
Blood Sample Collection and Analysis
For BLL determination, nurses collected blood samples from the antecubital vein using tubes with heparin. The samples were transported to the laboratory in styrofoam coolers, and the analysis for lead was performed during the first 48 h after sampling using atomic absorption spectophotometry coupled with graphite furnace [15].
Statistical Analysis
We characterized socioeconomic conditions based on multiple variables including: income level or SEP, housing conditions, attained parent’s education, health insurance and race. BLL were reported in micrograms per deciliter. Descriptive and univariate analysis were carried out using distributional plots and tests statistics according to variable type.
We developed multiple regression models (lineal and poisson) to evaluate the association between the exposure of interest (i.e., living in proximity to an industrial zone) and the main outcome variable (i.e., BLL), adjusting for demographic characteristics (i.e., age and sex), socioeconomic conditions (i.e., race, SEP, health insurance, and mother’s education attained), and risk behaviors (i.e., child plays with batteries). For continuous BLL, we used multiple linear regression models. In addition, based on evidence of adverse effects for BLL between 5 and 10 μg/dl [8] and given that all concentrations in our study were below defined toxicity levels (>10 μg/dl), we created two categories for BLL (<5 and ≥5 μg/dl). Analysis for this dichotomous outcome was developed using Poisson regression models with robust variance estimators, which provide correct estimates of prevalence ratios (PR) for the analysis of cross-sectional studies with binary outcomes [16–18].
Additionally, we evaluated whether socioeconomic condition variables modify the effect of the exposure of interest on BLL, and performed tests for interaction. All statistical analyses were conducted using Stata 10.0®.
Results
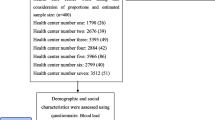
The study was conducted on 350 schoolchildren, 156 of them living in the exposed area. Both exposed and non-exposed areas shared similar distribution on age, sex and residence time. In contrast, schoolchildren in the non-exposed area had lower SEP, less health insurance affiliation, and a higher percentage of black ethnicity (Table 1). However, no statistically significant differences were observed regarding indoor sources of lead between non-exposed and exposed areas. A similar proportion of schoolchildren at both areas were likely to get exposed inside households by playing with (7.1 %) or handling-recycling (2.6 %) batteries (Table 1).
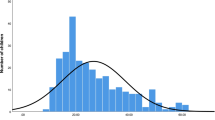
All BLL were below 10 μg/dl (Table 2). Schoolchildren in the exposed area had higher BLL than those in non-exposed area (4.7 ± 1.6 vs. 3.0 ± 1.2, p = 0.00), and the maximum concentration was found in one child among those exposed (9.9 μg/dl) (Fig. 1). In addition, a higher prevalence of BLL of ≥5 μg/dl was found in schoolchildren living in the exposed area as compared with the non-exposed area (44.2 vs. 8.2 %, p = 0.00) (Table 2).

Frequency distribution of BLL in children living in exposed and non-exposed areas
After adjusting for possible confounding factors, residential proximity to an industrial zone was found to be associated with higher BLL (Table 3). On average, exposed children had 1.98 μg/dl higher BLL than those in the non-exposed area (95 % confidence interval (95 % CI), 1.67, 2.29; p = 0.00); children below 10 years of age had higher BLL than older children (0.35 μg/dl; 95 % CI, 0.04, 0.55; p = 0.02), and boys had higher levels than girls (0.58 μg/dl; 95 % CI, 0.29, 0.86; p = 0.00). Regarding variables of socioeconomic condition, we found that black children had 0.92 μg/dl higher lead concentrations than those of other ethnic groups (95 % CI, 0.44; 1.40; p = 0.00), and schoolchildren at low SEP had 0.78 μg/dl higher BLL than those in middle SEP (95 % CI, 0.47, 1.10; p = 0.00). Additionally, children exposed to lead by playing with batteries had higher BLL (0.54 μg/dl, 95 % CI, −0.01, 1.09; p = 0.05). In contrast, we did not find significant differences in BLL by health insurance affiliation status and mother’s education attained (Table 3).
We built a multiple regression poisson model to evaluate factors associated to BLL of ≥5 μg/dl (Table 4), and found that, independent of covariables, schoolchildren in the exposed area were 6.68 (95 % CI, 3.95, 11.29; p = 0.00) times more likely to have BLL of ≥5 μg/dl than schoolchildren in non-exposed area. Other factors found associated with BLL of ≥5 μg/dl were younger age (6–9 years old) and male gender. Regarding variables of socioeconomic condition, we found that black children were 2.32 times more likely to have BLL of ≥5 μg/dl than schoolchildren of other ethnic groups (95 % CI, 1.39, 3.89; p = 0.00), and also, that schoolchildren of low SEP were 2.02 times more likely to have higher BLL than those in middle SEP (95 % CI, 1.35, 3.04; p = 0.01). In addition, we did not find differences in the likelihood of BLL of >5 μg/dl by other variables of socioeconomic condition such as health insurance and mother’s education level (Table 4).
To evaluate interaction, we estimated the independent effects of lead exposure and socioeconomic condition, this latter determined by SEP and race. In particular, we found a synergistic effect between exposure to lead from the industrial zone and SEP with a significant excess of lead concentration among children living in the exposed area with low SEP (interaction coefficient, 0.80; 95 % CI, 0.17, 1.43; p = 0.01), and almost a double prevalence of BLL of >5.0 μg/dl among these children, although not reaching statistical significance (interaction coefficient, 1.90–95 % CI, 0.55; 6.59; p = 0.31) (Table 5).
Additionally, we found an important independent effect of race on BLL, among children in the non-exposed area. In particular, among non-exposed children, black ethnicity was associated with a 0.92 μg/dl increase in BLL with a 3.8 times higher prevalence of BLL of >5.0 μg/dl. This finding suggests an effect no mediated by the same mechanisms of exposure among black children (Table 5).
Discussion
Schoolchildren, both exposed and non-exposed to industrial sources of lead were found to have BLL below 10 μg/dl. Mean concentration was higher among children in the exposed area (4.7 ± 1.6 vs. 2.9 ± 1.2 μg/dl; p = 0.000), and the maximum concentration was also observed in a child living in this zone (9.9 μg/dl). Research since 1990 has found substantial evidence in the effect on children’s neuropsychological and physical development of blood lead concentrations between 5 and 10 μg/dl. Based on this evidence, and given that levels considered safe in children have not been on full agreed [19], in this study, we established for our analysis a cutoff point of 5 μg/dl.
At the moment of this publication, the Advisory Committee on Childhood Lead Poisoning Prevention (ACCLPP) of CDC was recommending that the reference value be lowered to 5 μg/dl (based on the 97.5th percentile of the BLL distribution in children aged 1 to 5 years) and on growing evidence of adverse cognitive, behavioral, and physiological effects of BLLs greater than 10 μg/dl. This recommendation means that the number of children requiring medical care and follow-up environmental services could increase and focus on the importance of primary prevention of lead exposure in children and in consequence could prevent further irreversible effects on health [20].
According to this cutoff point, schoolchildren living in the exposed area had a higher prevalence of BLL of ≥5 μg/dl as compared with non-exposed children (44.2 vs. 8.2 %; p = 0.00). The prevalence we found in our exposed study area was greater than others reported in similar populations. In particular, Morales et al., found in Mexican-American that 19 % of children aged 5–11 years and 12 % of children 12–17 years had BLL of ≥5 μg/dl [21]. In contrast, ours is lower than the prevalence reported by Oliver-Verbel et al., in a study in children aged 5 to 9 years living in different areas of Cartagena-Colombia, in which 57.6 % of children had BLL of ≥5 μg/dl [3]. The main sources of lead exposure for these children were the work-related activities of their parents such as small metal melting factories and fishermen who make lead sinkers for their fishing nets [3]. It is also possible that the socioeconomic conditions in children from Cartagena, Colombia were worse than the children in our study area in Cali.
We found a statistically significant association between exposure to industrial sources of lead and higher BLL independent of age, sex, race, weight, socioeconomic status, and time of residence in the study area. The differences found between exposed and not exposed schoolchildren suggest that the industrial zone is a source of chronic lead exposure in those children. These findings are similar to those found by Lalor et al. who determined higher BLL in children living in urban areas closed to manufacturing and smelting industries in Jamaica [22]. In addition, research made in China has found that BLLs in children living in industrial areas is significantly higher as compared with those living in urban, suburban, and rural areas [23].
We also identified several factors associated with higher BLLs in the study population. Specifically, we found that demographic variables such as age, race and sex were statistically significant and independently associated with BLL. In addition, other sources of lead exposure (i.e., playing with batteries at home) were associated with higher BLL.
This study is consistent with previous research showing a higher BLL among boys, younger and black children [3, 21, 23–25]. Children are susceptible because of their normal hand-to-mouth behavior, which leads to the ingestion of objects or exposure to contaminated soil. Additionally, boys have an active personality and different behavior patterns than girls, because they are more likely to play outdoors or crawl on floors. In contrast with these findings, the study developed in Jamaica by Lalor et al., did not establish differences in BLL concentrations between boys and girls; the geometric mean values for those with BLL of <10 μg/dl was 3.3 and 3.2 μg/dl, respectively, and for BLL of >10, 20.4, and 20.6 μg/dl, respectively [22].
In contrast with other studies, we did not find mother’s attained education to be associated with BLL. In the study conducted by Morales et al., Mexican-American children living in United States whose head of household has less than 6 years of education had higher BLL than those with 13 or more years of education attained [21].
In assessing the role of socioeconomic conditions on lead exposure, we found that lower SEP and black ethnicity were independently associated with a higher risk of exposure to lead. Additionally, we found a synergistic interaction between exposure to the industrial zone and SEP for higher BLL concentrations. These findings are consistent with previous studies that have found that children living in low-income housing and public housing are more likely to have elevated BLL [21]. Similar findings have been reported among pregnant women with low socioeconomic conditions [12].
Historically, it has been identified that communities in low socioeconomic condition and ethnic minorities have a disproportionate exposure to some environmental pollutants. This is attributed to land use patterns, political, economic, and cultural structure of the regions [13]. A confluence of these factors affect housing market dynamics, a systemic racism and class bias in land use decisions that push noxious facilities toward poor neighborhoods, leaving these communities at a disadvantage [13, 26, 27].
In addition to differential exposure by SEP and race, there is an interaction with social factors (i.e., less access to food and to health care services), cultural factors (i.e., nutritional practices and handling batteries in home), and behavioral, educational, and biological factors that make population in low socioeconomic condition more susceptible to lead exposures and its accumulation in blood [12, 21, 22].
Previous researches have shown that children who live in poverty could have poor nutritional conditions and less access to food that results in calcium and iron blood deficiencies. A low calcium diet produces an increase in lead toxicity and deposition in bone while iron deficiency results in increased susceptibility to lead toxicity [12, 22]. A study developed by Lanphear et al., found an inverse and statistically significant relationship between BLL and intake of iron in diet [28].
In our study, we found that black children in the non-exposed area have higher BLL than non-black children in this area, suggesting that race plays an independent role in lead exposure beyond the industrial sources. This could be explained, at least in part, to differential risk practices for lead exposure among black population that can produce higher BLL independent of industrial sources. In a predominantly black community in our city, we found that almost 5.5 % of this population handle or recycle batteries in household (5.3 %; CI, 4.8–5.7). We also found high levels of heavy metals (lead and mercury) in fish that are used for consumption by this community (unpublished results). However, additional studies are necessary to evaluate this hypothesis.
The fact that black and poorest children have statistically significantly higher BLLs than children of other ethnicities and higher SEP independent of exposure to the industrial sources of lead suggests that, race and socioeconomic condition may be important to consider when formulating lead screening and abatement interventions for children in Colombia. Educational campaigns to reduce lead exposure should focus special attention to black and low SEP families, taking into account culturally specific causes of lead exposure such as mentioned above, which are common in Colombia.
In summary, the results of this study show that children living near industrial sources of lead are at higher risk for elevated BLL than children living in other urban areas. Also, levels of exposure are elevated in children from families of low SEP and black ethnicity. The results of this study were presented to the Environmental Authorities who are in the process of declaring this industrial area as a “Source Area,” which means more strict surveillance of the emissions and non-exposed activities. However, due to the history of exposure of these children, additional studies may be needed in evaluating the long-term impact on the health of these children, in particular those related with cognitive and behavioral effects of lead exposure. Nevertheless, this action from the environmental authority shows how the results of research can be translated into the decision-making.
References
Meyer PA, Pivetz T, Dignam TA, Homa DM, Schoonover J, Brody D (2003) Centers for Disease Control and Prevention. Surveillance for elevated blood lead levels among children—United States, 1997–2001. MMWR Morb Mortal Wkly Rep Surveill Summ 52(10):1–21
Iqbala S, Muntnerb P, Batumanc V, Rabitoa F (2008) Estimated burden of blood lead levels ×5 mg/dl in 1999–2002 and declines from 1988 to 1994. Environ Res 107:305–311
Olivero-Verbel J, Duarte D, Echenique M, Guette J, Johnson-Restrepo B, Parsons P (2007) Blood lead levels in children aged 5–9 years living in Cartagena, Colombia. Sci Total Environ 372:707–716
Miranda ML, Kim D, Galeano MAO, Paul CJ, Hull AP, Morgan SP (2007) The relationship between early childhood blood lead levels and performance on end-of-grade tests. Environ Health Perspect 115(8):1242
Norman R, Mathee A, Barnes B, van der Merwe L, Bradshaw D (2007) Estimating the burden of disease attributable to lead exposure in South Africa in 2000. S Afr Med J 97:773–80
Surkan PJ, Zhang A, Trachtenberg F, Daniel D, Sonja McKinlay, Bellinger DC (2007) Neuropsychological function in children with blood lead levels <10 μg/dl. Neurotoxicology 28:1170–77
Wang Q, Zhao HH, Chen JW, Gu KD, Zhang YZ, Zhu YX, Zhou YK, Ye LX (2009) Adverse health effects of lead exposure on children and exploration to internal lead indicator. Sci Total Environ 407:5986–5992
Canfield RL, Henderson CR, Cory-Slechta DA, Cox C, Jusko TA, Lanphear BP (2003) Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 348(16):1517–26
Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC (2005) Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect 113:894–899
Bernard SM (2003) Should the Centers for Disease Control and Prevention’s childhood lead poisoning intervention level be lowered? Am J Public Health 93:1253–60
Reisa F, Sampaioa C, Brantesa A, Anicetoa P, Melimb M, Cardosob L et al (2007) Human exposure to heavy metals in the vicinity of Portuguese solid waste incinerators—part 3: biomonitoring of Pb in blood of children under the age of 6 years. Int J Hyg Environ Health 210:455–459
Farias P, Boria-Aburto V, Rios C, Hertz-Picciotto I, Rojas-Lopez M, Chavez-Ayala R (1996) Blood lead levels in pregnant women of high and low socioeconomic status in Mexico City. Environ Health Perspect 104(10):1070–1074
O’Neill M, Jerrett M, Kawachi I, Levy J, Cohen A, Gouveia N, Wilkinson P, Fletcher T, Cifuentes L, Schwartz J (2003) Health, wealth, and air pollution: advancing theory and methods. Environ Health Perspect 111(16):1861–1870
U.S Environmental Protections Agency. National Ambient Air Quality Standards (NAAGS). http://www.epa.gov/air/criteria.html.
Miller DT, Paschal DC, Gunter EW, Stroud PE, D’Agelo J (1987) Determination of lead in blood using electrothermal atomisation atomic absorption spectrometry, a L’vov platform and matrix modifier. Analyst 112:1701–1704
Barros A, Hirakata N (2003) Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 3:21–46
Coutinho L, Scazufca M, Menezes P (2008) Methods for estimating prevalence ratios in cross-sectional studies. Rev Saude Publica 42(6):1–6
James L, Seng-Tan C, Seng-Chia K (2009) A practical guide for multivariate analysis of dichotomous outcomes. Annals Academy of Medicine 38(8):714–719
CDC (2007) Lead exposure among females of childbearing age—United States, 2004. Morb Mortal Wkly Rep 56(16):397–400
Advisory Committee on Childhood Lead Poisoning Prevention (2012) Centers for Disease Control and Prevention (2012). Low level lead exposure harms children: a renewed call for primary prevention. CDC, Atlanta, GA
Morales L, Gutierrez P, Escarce J (2005) Demographic and Socioeconomic factors associated with blood lead levels among Mexican-American children and adolescents in the United States. Public Health Rep 120:448–454
Lalor G, Vutchkov M, Bryan S (2007) Blood lead levels of Jamaican children island-wide. Sci Total Environ 374(2–3):235–241
Wang S, Zhang J (2006) Blood lead levels in children, China. Environ Res 101:412–418
Rajkumar W, Manohar J, Doon R, Siung-Chang A, Chang-Yen I, Monteil M (2006) Blood lead levels in primary school children in Trinidad and Tobago. Sci Total Environ 361:81–87
Rojas M, Espinosa C, Seijas D (2003) Asociación entre plomo en sangre y parámetros sociodemográficos en población infantil. Rev Saude Publica 37(4):503–509
Been V (1993) What’s fairness got to do with it? Environmental justice and the siting of locally undesirable land uses. Cornell Law Rev 78:1001–1036
Pulido L (2000) Rethinking environmental racism: white privilege and urban development in Southern California. Ann Assoc Am Geogr 90:12–40
Lanphear BP, Hornung R, Ho M, Howard CR, Eberly S, Knauf K (2002) Environ lead exposure during early childhood. J Pediatr 140:40–7 [published correction appears in J Pediatr. 2002; 140:490]
Acknowledgments
Special thanks to schoolchildren living in the study areas for participating and provide valuable information. Additionally, special thanks to the Ministry of Environment (Ministerio de Ambiente, Vivienda y Desarrollo Territorial) for funding support of this project and the regional and local environmental and health authorities for participating in this project.
Conflict of Interest
The authors declare that there is no conflict of interest in conducting this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Filigrana, P.A., Méndez, F. Blood Lead Levels in Schoolchildren Living Near an Industrial Zone in Cali, Colombia: The Role of Socioeconomic Condition. Biol Trace Elem Res 149, 299–306 (2012). https://doi.org/10.1007/s12011-012-9429-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-012-9429-2