
Abstract
Nutritional deficiencies are important and widespread problems in most developing countries. Preventing and correcting micronutrient deficiencies are important because of the multiple negative consequences of these deficiencies. This study was designed to determine the prevalence of copper deficiency in an adult population in Shiraz, southern Iran. We also determined the association between copper status and other factors such as age, sex, and body mass index (BMI).In this cross-sectional study, 416 adults residing in Shiraz were selected by two-stage sampling. Serum copper was measured by flame-atomic absorption spectrometry. The data were analyzed with SPSS software. Mean age in our sample was 39.33 ± 15.06 years, and mean BMI was 26.17 ± 4.81 kg/m2. Mean serum copper concentration was 118.15 ± 54.33 μg/dL in the whole sample, 109.74 ± 56.22 μg/dL in men, and 122.15 ± 53.04 μg/dL in women. The overall prevalence of copper deficiency was 24%. The prevalence of copper deficiency differed significantly between men and women but not between different age groups. Serum copper concentration correlated significantly with BMI (p < 0.05). This study is the first to evaluate serum copper status in a healthy population in southern Iran. We show that the mean copper concentrations were higher than those reported for Iranian populations in northern cities and were also higher compared with studies in most other countries. We suggested more detailed studies to identify the etiological determinants of this nutritional deficiency in Iran and elsewhere.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Micronutrient-related malnutrition is one of the most important nutritional problems worldwide, especially in most developing countries, and represents a serious health threat for more than two billion people worldwide [1, 2]. One threat is the result of insufficient or unbalanced nutritional intake, and another is due to secondary complications from other diseases. Both problems can be evaluated by analyzing element concentrations in serum or other tissues [3].
Minerals, hormones, and different enzymes are known to have beneficial effects on growth. More than 25% of the body's enzymes depend on mineral ions for their proper functioning and metabolic activities [1]. Minerals such as copper are essential because they play a key role in various activities such as regulatory functions, as well as immunological and enzyme functions [4–7]. The most common clinical manifestations of copper deficiency are anemia, bone abnormalities [8], and sensorineural disorders [5]. Because copper plays an important role in the biological transfer of electrons, it is vital for the synthesis of red blood cells and the maintenance of nervous system structure and function [4]. Copper deficiency in adults can therefore result in blood and nervous system disorders [6, 9]. Moreover, copper plays an important role in the body's immune system and immune response [1].
Various studies have assessed copper deficiencies in various diseases, and the prevalence of copper deficiencies has been reported in other healthy populations [1, 4, 5, 9–12]. However, few community-based studies have investigated the prevalence of copper deficiency in the healthy Iranian population, and information about copper status among the people of southern Iran is lacking. Therefore, this study was conducted to determine the prevalence of this nutritional problem in this region.
Materials and Methods
This analytical cross-sectional study was done at the Endocrine Research Center of Shiraz University of Medical Sciences in 2010 in Shiraz, Iran. The study protocol was approved by the Review Board of Shiraz Endocrine Research Center and the Shiraz University of Medical Sciences Ethics Committee.
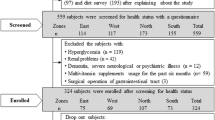
Sample size for the estimation of mean serum copper concentration was calculated as 440 subjects, for an alpha level of 0.05.The subjects were selected by random sampling from each of the eight districts of Shiraz. First, postal codes that ended in even digits were chosen. Then, from each district, 55 individuals were selected (55 families from each district and one adult person from each family) with a table of random numbers. Each participant signed a written informed consent form after the nature of the study was explained to them.
The exclusion criteria were the presence of gastrointestinal disease including malabsorption or hepatic disorders, renal and cardiovascular disease, cancer, smoking, infection, use of oral contraceptives, chronic inflammatory disease, pregnancy, and a vegetarian diet. After excluding participants with any of these conditions, the total number of participants was 416 (134 men, aged 18–95 years and 282 women, aged 18–96 years).
A trained research assistant recorded anthropometric measurements in each participant, with the participants wearing light clothing and no footwear. Each participant was weighed to the nearest 0.1 kg with a portable digital balance. The height in all participants was measured to the nearest 1 cm with a portable stadiometer. Body mass index (BMI) was calculated as weight (kg)/height² (m), and was classified into four groups: BMI < 20, 20 ≤ BMI < 25, 25 ≤ BMI < 30, and BMI ≥ 30.
Serum concentrations of copper were measured by atomic absorption spectrometry (Chemtech Analytical CTA 2000, AAS, Kempston, UK). A copper concentration lower than 80 μg/dL was considered to indicate a low serum copper level [13].
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS version 16.0.1, SPSS Inc, Chicago, IL). The data are presented as the mean ± standard deviation. One-way ANOVA and Student's two-tailed t test were used to compare the mean values obtained in different groups. Frequencies were compared with the chi-squared test. Pearson's correlation coefficient was used to study the correlation of copper concentration with age and BMI. In all analyses, the level of significance was considered p < 0.05.
Results
Two thirds (67.8%) of the 416 participants in study were women. Mean age of the participants was 39.33 ± 15.06 years, and mean BMI was 26.17 ± 4.81 kg/m². One third (30.3%) was less than 30 years old; 26.2% were in the 30–39-year-old group, 20.2% in the 40–49-year-old group, and 23.3% in the over-50-year-old group. Table 1 shows some of the demographic variables of the participants. Mean height and weight differed significantly between men and women (p < 0.05). Except for BMI, the mean value for all other variables was higher in men.
Table 2 shows the serum copper levels in different subgroups based on gender, age, and BMI. The overall mean serum copper level was 118.15 ± 54.33 μg/dL (18.6 ± 8.5 μmol/L). Mean serum copper level did not differ significantly between men and women (p > 0.05). The frequency distribution of copper concentrations in men and women is shown in Fig. 1. Most individuals (60.8% overall, 64.2% women, 53.7% men) had a serum concentration of over 100 μg/dL.

Distribution of serum copper concentrations in the whole sample an in men and women. Each bar represents the percentage frequency distribution of individuals with each concentration of copper
The correlation between serum copper concentration and BMI was statistically significant (p = 0.015, r = 0.12), but we did not find any significant correlation between serum copper concentration and age (p = 0.393, r = −0.04).
There were no significant differences in mean copper concentration among different age or BMI subgroups (p > 0.05), but when we used the post hoc test, it detected a statistically significant difference in copper concentration between subgroups with a BMI of 20–25 or 25–30 and individuals with a BMI ≥ 30 (p < 0.05).
Table 3 shows the frequency distribution of copper deficiency in our study population based on gender, age, and BMI. The overall incidence of copper deficiency was 24%. The incidence of copper deficiency was significantly higher in men (31.3%) than in women (20.6%).
There was no significant difference in the incidence of copper deficiency among age subgroups or BMI subgroups (p > 0.05). However, we found the highest percentage of copper deficiency in the under-40 age groups and the BMI under-30 subgroups.
Discussion
Mean copper concentration in our study population was 118.15 ± 54.33 μg/dL. Other studies in northern cities of Iran such as Mashhad and Tehran showed the mean copper concentrations of 14.7 ± 3.3 μmol/L (93.39 ± 20.96 μg/dL) and 95 ± 20 μg/dL, respectively [6, 14]. Thus, serum copper concentration in this study was higher than in northern parts of Iran. Table 4 compares the mean serum concentrations of copper in the present study and several other studies. The mean concentration for copper in this study was similar to figures for Greece and Northern Ireland and but higher than in Germany, Norway, continental Spain, the Canary Islands (Spain), Oman, China, and India. However, compared with the high value reported for Kuwait, mean serum copper in all adult Iranian populations was lower [15–24]. This difference could be due to local or regional differences in nutritional habits.
Our study found that mean serum copper concentration was higher in women than men, although this difference was not statistically significant. Other studies also found higher copper concentrations in women, which is consistent with the present study [6, 16, 18, 21]. The differences among age subgroups were not statistically significant. In a study of Greek schoolchildren and their parents [25], there was also no significant difference between the age groups; however, a significant trend was seen toward higher concentrations in younger members of the population. In a Northern Ireland study, the opposite trend was seen: Serum copper concentration was higher in older age groups [18].
The total prevalence of copper deficiency among our participants was 24% (20.6% in women, 31. 3% in men). Another study of persons 18 to 75 years old in India reported a prevalence of copper deficiency of 34%, a higher figure compared with our study [15]. However, in a study of people older than 60 years of age in Chile, the prevalence of copper deficiency was 5.1% in women and 6.5% in men, which was lower than in the participants of our study [26]. The different results reported in different studies may reflect personal differences among participants. Although all studies compared groups of adults, the genetic, nutritional, demographic, and racial factors considered were different, and different criteria were used to diagnose copper deficiency. For example, in some studies, the cut-off point for copper deficiency was below 80 μg/dL, whereas other studies used a cut-off value of 75 μg/dL.
One of most noteworthy finding in this study was the statistically significant difference between sexes in the prevalence of copper deficiency, which was higher in men than in women. A study in India reported the same finding [15]: a higher mean copper concentration in females and a lower prevalence of copper deficiency.
In our study population, serum copper status correlated significantly with BMI: As BMI increased, so did serum copper concentration. A similar finding was reported in studies done in Kuwait and Iran [6, 17].
As previous studies have shown, many factors influence the etiology of micronutrient deficiencies, such as genetic factors, insufficient absorption, and some infectious diseases. In developing countries, low dietary quality plays a significant role in the insufficient intake of micronutrients. In addition, environmental factors play a prominent role in the amounts of elements available in the soil [1, 27, 28].
Conclusion
This study shows that mean serum copper concentrations in Shiraz (southern Iran) were higher than those reported for Iranian populations in the northern part of the country and were also higher compared with other countries. We suggest more comprehensive studies are needed to determine the etiology of this micronutrient deficiency in different Iranian populations (as well as other populations) and to explain the differences between populations in different parts of Iran as well as different regions worldwide.
References
Van Nhien N, Khan NC, Ninh NX, Van Huan P, le Hop T, Lam NT, Ota F, Yabutani T, Hoa VQ, Motonaka J, Nishikawa T, Nakaya Y (2008) Micronutrient deficiencies and anemia among preschool children in rural Vietnam. Asia Pac J Clin Nutr 17(1):48–55
Hettiarachchi M, Liyanage C, Wickremasinghe R, Hilmers D, Abrams S (2006) Prevalence and severity of micronutrient deficiency: a cross-sectional study among adolescents in Sri Lanka. Asia Pac J Clin Nutr 15(1):56–63
Kocyigit A, Gur S, Erel O, Gurel MS (2002) Associations among plasma selenium, zinc, copper, and iron concentrations and immunoregulatory cytokine levels in patients with cutaneous leishmaniasis. Biol Trace Elem Res 90(1–3):47–55
Ferdaus MZ, Hasan AK, Shekhar HU (2010) Analysis of serum lipid profiles, metal ions and thyroid hormones levels abnormalities in thalassaemic children of Bangladesh. J Pak Med Assoc 60(5):360–365
Sachdeva R, Chug S, Sangha J (2006) Haemopoetic, serum minerals and intellectual status of institutionalized and non institutionalized boys. J Hum Ecol 19(4):235–238
Ghayour-Mobarhan M, Shapouri-Moghaddam A, Azimi-Nezhad M, Esmaeili H, Parizadeh SM, Safarian M, Kazemi-Bajestani SM, Khodaei GH, Hosseini SJ, Parizadeh SM, Ferns GA (2009) The relationship between established coronary risk factors and serum copper and zinc concentrations in a large Persian cohort. J Trace Elem Med Biol 23(3):167–175
McMillin GA, Travis JJ, Hunt JW (2009) Direct measurement of free copper in serum or plasma ultrafiltrate. Am J Clin Pathol 131(2):160–165
Uauy R, Olivares M, Gonzalez M (1998) Essentiality of copper in humans. Am J Clin Nutr 67(5 Suppl):952S–959S
Shankar P, Boylan M, Sriram K (2010) Micronutrient deficiencies after bariatric surgery. Nutrition 26(11–12):1031–1037
Pathak P, Kapil U, Kapoor SK, Saxena R, Kumar A, Gupta N, Dwivedi SN, Singh R, Singh P (2004) Prevalence of multiple micronutrient deficiencies amongst pregnant women in a rural area of Haryana. Indian J Pediatr 71(11):1007–1014
Awadallah SM, Abu-Elteen KH, Elkarmi AZ, Qaraein SH, Salem NM, Mubarak MS (2004) Maternal and cord blood serum levels of zinc, copper and iron in healthy pregnant Jordanian women. J Trace Elem Exp Med 17(1):1–8
García-Casal MN, Leets I, Bracho C, Hidalgo M, Bastidas G, Gomez A, Peña A, Pérez H (2008) Prevalence of anemia and deficiencies of iron, folic acid and vitamin B12 in an Indigenous community from the Venezuelan Amazon with a high incidence of malaria. Arch Latinoam Nutr 58(1):12–18
Elmer P, Conn N (1975) Analytical methods for atomic absorption spectrophotometry. Oxford University Press, London, pp 273–290
Farzin L, Moassesi ME, Sajadi F, Amiri M, Shams H (2009) Serum levels of antioxidants (Zn, Cu, Se) in healthy volunteers living in Tehran. Biol Trace Elem Res 129(1–3):36–45
Kapil U, Singh P (2005) Serum copper levels among a tribal population in Jharkhand State, India: a pilot survey. Food Nutr Bull 26(3):309–311
Kouremenou-Dona E, Dona A, Papoutsis J, Spiliopoulou C (2006) Copper and zinc concentrations in serum of healthy Greek adults. Sci Total Environ 359(1–3):76–81
Abiaka C, Olusi S, Al-Awadhi A (2003) Reference ranges of copper and zinc and the prevalence of their deficiencies in an Arab population aged 15–80 years. Biol Trace Elem Res 91(1):33–43
McMaster D, McCrum E, Patterson CC, Kerr MM, O'Reilly D, Evans AE, Love AH (1992) Serum copper and zinc in random samples of the population of Northern lreland. Am J Clin Nutr 56(2):440–446
Zhang HQ, Li N, Zhang Z, Gao S, Yin HY, Guo DM, Gao X (2009) Serum zinc, copper, and zinc/copper in healthy residents of Jinan. Biol Trace Elem Res 131(1):25–32
Rükgauer M, Klein J, Kruse-Jarres JD (1997) Reference values for the trace elements copper, manganese, selenium, and zinc in the serum/plasma of children, adolescents, and adults. J Trace Elem Med Biol 11(2):92–98
Díaz Romero C, Henríquez Sánchez P, López Blanco F, Rodríguez Rodríguez E, Serra ML (2002) Serum copper and zinc concentrations in a representative sample of the Canarian population. J Trace Elem Med Biol 16(2):75–81
Terrés-Martos C, Navarro-Alarcón M, Martín-Lagos F, López-G de la Serrana H, López-Martínez MC. (1997 ) Determination of copper levels in serum of healthy subjects by atomic absorption spectrometry. Sci Total Environ 9;198(1):97–103.
Abiaka C, Al-Tobi M, Joshi R (2008) Serum micronutrient and micromineral concentrations and ratios in healthy Omani subjects. Med Princ Pract 17(4):334–339
Helgeland K, Haider T, Jonsen J (1982) Copper and zinc in human serum in Norway: relationship to geography, sex and age. Scand J Clin Lab Invest 42:35–39
Voskaki I, Arvanitidou V, Athanasopoulou H, Tzagkaraki A, Tripsianis G, Giannoulia-Karantana A (2010) Serum copper and zinc levels in healthy Greek children and their parents. Biol Trace Elem Res 134(2):136–145
Olivares M, Hertrampf E, Capurro MT, Wegner D (2000) Prevalence of anemia in elderly subjects living at home: role of micronutrient deficiency and inflammation. Eur J Clin Nutr 54(11):834–839
Fishman SM, Christian P, West KP (2000) The role of vitamins in the prevention and control of anemia. Public Health Nutr 3:125–150
Stoltzfus RJ (2001) Defining iron-deficiency anemia in public health terms: a time for reflection. J Nutr 131:565S–567S
Acknowledgements
We thank K. Shashok (author AID in the Eastern Mediterranean) for improving the use of English in the manuscript and M. Gholami at the Center for Development of Clinical Research of Nemazee Hospital for research assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dabbaghmanesh, M.H., Salehi, N.M., Siadatan, J. et al. Copper Concentration in a Healthy Urban Adult Population of Southern Iran. Biol Trace Elem Res 144, 217–224 (2011). https://doi.org/10.1007/s12011-011-9074-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-011-9074-1