
Abstract
Glucose intolerance in fluorosis areas and when fluoride is administered for the treatment of osteoporosis has been reported. Controlled fluoridation of drinking water is regarded as a safe and effective measure to control dental caries. However, the effect on glucose homeostasis was not studied so far. The aim of this study was to evaluate the effect of the intake of fluoridated water supply on glucose metabolism in rats with normal and deficient renal function. Male Sprague–Dawley rats were divided into eight groups of four rats. Renal insufficiency was induced in four groups (NX) which received drinking water containing 0, 1, 5, and 15 ppm F (NaF) for 60 days. Four groups with simulated surgery acted as controls. There were no differences in plasma glucose concentration after a glucose tolerance test between controls and NX rats and among rats with different intakes of fluoride. However, plasma insulin level increased as a function of fluoride concentration in drinking water, both in controls and in NX rats. It is concluded that the consumption of fluoridated water from water supply did not affect plasma glucose levels even in cases of animals with renal disease. However, a resistance to insulin action was demonstrated
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Controlled fluoridation of drinking water (0.7–1.2 ppm, mg/l) is regarded as a safe and effective measure to control dental caries and is employed in many cities around the world [1]. People that drink water containing around 1.0 ppm fluoride have usually plasma fluoride concentrations between 0.5 and 1.5 μM (μmole/l). Plasma fluoride concentration is controlled by basically two mechanisms: renal fluoride excretion and fluoride uptake by bone. In humans, the renal clearance of fluoride is typically around 28–52 ml/min and depends on the glomerular filtration rate, urinary pH, and plasma flow through the kidney [2]. However, in patients with renal failure, fluoride might accumulate in plasma, even with low intake of the ion, because of the deficiency in the renal function [3]. Osteomalacia and decrease in bone strength by the intake of high-level fluoridated water have been reported in rats [4]. As a consequence, it could be speculated that the occurrence of side effects of fluoride would appear in these patients even with low intake of fluoride, as with the ingestion of optimally fluoridated water, which has not been studied so far.
Fluoride has been reported to produce hyperglycemia as a consequence of an inhibitory effect of fluoride on the secretion of insulin by an alteration in the intracellular signaling pathway related to the secretion of insulin [5]. This effect was observed when plasma fluoride concentration is higher than 5 μM after a single dose of NaF in rats (7.6 mg F/kg body weight) and in humans (60 mg NaF) [6] and also after the administration of drinking water with fluoride 100 ppm to rats for 30 days [7]. The effect appears not to be related to insulin resistance [8], and it disappears when rats have high bone fluoride content, which is consistent with low plasma and tissue fluoride levels [7].
Additionally, it has been reported that humans living in areas of endemic fluorosis have higher bone mineral density when compared to residents of areas with low fluoride levels in the drinking water, and their insulin response is negatively correlated with plasma fluoride concentration [9], which has been attributed to insulin resistance rather than to a decrease in the secretion of insulin [10].
Thus, the aim of the present study was to evaluate the homeostasis of glucose in rats with renal deficiency that had been drinking water with fluoride levels comparable to those present in artificially [1] and in naturally fluoridated water [11] to prevent dental decay.
Materials and Methods
Animals and Treatments
Thirty-two male 7-week-old Sprague–Dawley rats were randomly divided into eight groups (four rats per group). In four groups, renal insufficiency was surgically induced (NX) and four groups acted as controls (Sham). Sodium fluoride (NaF, Sigma Co., Saint Louis, MO, USA) was used as a source of fluoride (F), and it was administered in the drinking water for 60 days after the surgery.
Experiments were carried out in accordance with the International Guidelines of Animal Care. The protocol was approved by the Ethics Committee, School of Medicine, Rosario National University.
The model used to produce renal deficiency was the remnant kidney model that involves the surgical reduction of renal parenchyma. This model is widely used to study events under chronic renal insufficiency [12]. The surgery was performed in order to obtain a renal insufficiency that simulates a moderate decrease in the renal function but not a severe renal disease. All procedures were done with aseptic techniques and under intramuscular anesthesia with ketamine (6 mg/100 g body weight) and xylazine (0.3 mg/100 g body weight). The ablation of the right kidney was done through a 1-cm paramedian lumbar incision. One week later, a 1-cm left paramedian ventral incision was performed and one or two extrarenal branches of the left renal artery were microligated. The described procedure produces an infarction of approximately two thirds of the renal parenchyma. The success of the procedure was immediately verified by the change in the color of the kidney (red to black) and by the measurement of renal function parameters throughout the experiment. Sham-operated rats were subjected to the same procedure but without the ablation of the right kidney and the microligatures of the extrarenal branches of the left renal artery.
Thirty minutes before both surgeries, ceftriaxone was intramuscularly administered (3 mg/100 g body weight), and after surgeries, diclofenac was subcutaneously injected (1.25 mg/100 g body weight). Finally, rats were housed in individual cages for 60 days with water and food ad libitum.
Rats from groups Sham0, Sham1, Sham5, and Sham15 drank water with 0, 1, 5, and 15 ppm F, respectively. Rats from groups NX0, NX1, NX5, and NX15 drank water with 0, 1, 5, and 15 ppm F, respectively.
Every 15 days, body weight (g), 24-h water intake (ml/day), 24-h urinary flow (ml/day), urinary density (g/ml), urea plasma levels (mg/dl), and 24-h urinary fluoride excretion (μmol/day) were measured. Plasma glucose concentration (g/l) were also measured fortnightly at the end of the dark cycle. Body weight was measured with a 1-g sensitivity scale; water intake and urinary volume were measured with a measuring cylinder (0.5-ml sensitivity). Urinary density was measured by weighing 100 μl (micropipette, 5-μl precision) of urine in a 0.1-mg sensitivity scale. Blood was collected from the tail tip into heparinized capillary tubes, which were cut at the level of the buffy coat, and plasma was saved at −20°C for urea and glucose measurements. Plasma concentration of urea and glucose were spectrophotometrically measured with commercial kits (Wiener Lab, Rosario, Argentina) in a Perkin Elmer lambda 11 spectrophotometer.
Fluoride concentration in urine was measured with an ion selective electrode (Orion 94-09, Orion Research, MS, USA) in the direct way after the addition of TISAB II (Orion Research).
At the end of the experiment, glucose tolerance tests were carried out by the intraperitoneal injection of glucose (2.5 ml/100 g body weight of a 0.56 mol/l glucose solution) [7]. Before and after 30, 60, and 120 min of the glucose challenge, samples of blood were collected in heparinized capillary tubes as stated above for glucose measurement. In the 24 h after glucose tolerance test, urine was collected for creatinine measurement. After that, rats were killed by heart puncture under profound volatile anesthesia. Blood was collected with heparin as anticoagulant, and aliquots of plasma were saved for creatinine, insulin, and fluoride measurements
The clearance of creatinine was calculated with urinary volume (ml/min), plasma, and urine creatinine levels (mg/dl) using the following equation
Plasma fluoride concentration was measured with the ion selective electrode Orion 9409 (Orion Research Inc., Cambridge MA, USA) after isothermal distillation [13].
Measurement of plasma insulin levels were carried out by radioimmunoassay (RIA) using a commercial kit (RIA kit Rat insulin, Millipore Corporation, Billerica, MA, USA).
Bone Uptake of Fluoride Measurement
Rats were injected with 67 μl of 15 mM NaF (∼19 µg F) in the vein of the tail at 8.00 a.m. A sample of blood was obtained before the injection of the NaF dose. After the NaF injection, three blood samples were obtained from the tail tip (at 3, 18, and 33 min) and plasma fluoride concentration was measured. After that, urine was collected for 24 h and urinary excretion of fluoride was measured as stated above. With the equations derived from a mathematical model (see Appendix), the rate of fluoride uptake by bone tissue was calculated and expressed in micromoles F per liter per minute.
Statistical Analyses
Data are expressed as mean ± SE. When two samples of independent data were compared, statistical analyses were performed using a two-tailed Student's t test for continuous variables, and regression lines were calculated using the linear least-squares method. When more than two samples were compared, one-way ANOVA and Tukey’s or Bonferroni multiple comparison tests were employed.
Changes in body weight, 24-h water intake, 24-h urinary volume, urinary density, and urea plasma level throughout the experiment were analyzed by linear regression which was performed by finding the line that minimizes the sum of the squares of the vertical distances of the points from the line. When comparing two lines, slopes were compared first. If the slopes were not different, intercepts were compared. Runs test were performed to assure that the data were linear. Differences were considered significant when p < 0.05. The software GraphPad Prism version 2.0 for Windows (GraphPad Software, San Diego, CA USA) was used.
Results
Glucose Homeostasis
There were no significant differences either in glucose plasma levels throughout the experiment between Sham and NX rats or among the groups with different levels of fluoride (ANOVA, p > 0.05).
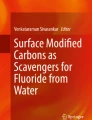
The values of plasma glucose concentration after 120 min of the glucose load did not significantly differ among the different experimental groups (ANOVA, p > 0.05). However, plasma insulin levels were significantly higher as fluoride concentration increased in drinking water (ANOVA, Bonferroni’s post-test, p < 0.05). In addition, insulin levels of NX rats were significantly lower than controls that drunk water with the same level of fluoride (Fig. 1)

Plasma insulin levels in rats with renal insufficiency (NX) and controls (Sham) with drinking water containing 0, 1, 5, and 15 ppm F (NaF). Results are expressed as mean ± SE. aSignificant differences compared to Sham0 and bcompared to NX0 (ANOVA, Bonferroni´s post hoc tests, p < 0.05)
Fluoruria
Urinary fluoride excretion of NX15 and Sham15 rats after 60 days of treatment were significantly higher than the values found for the other groups (ANOVA, Tukey’s test, p < 0.05). Despite NX rats receiving fluoride having lower values when compared to Sham-operated rats, no significant differences were detected between them (p > 0.05, Fig. 2).

Twenty-four-hour urinary fluoride excretion in rats with renal insufficiency (NX) and controls (Sham) with drinking water containing 0, 1, 5, and 15 ppm F (NaF). Results are expressed as mean ± SE. *Significant differences compared to rats with access to drinking water containing 0, 1, and 5 ppm F (ANOVA, Tukey’s post hoc tests, p < 0.05)
Plasma Fluoride Concentration
Plasma fluoride levels after 60 days of drinking fluoridated water were significantly higher in NX15 and Sham15 (ANOVA, Tukey’s test, p < 0.05) compared to the other groups. Despite the fact that the values found for NX15 rats were higher than those observed for the Sham15 rats, no significant differences were detected between them (p > 0.05, Fig. 3).

Plasma fluoride concentration after 60 days of surgery in rats with renal insufficiency (NX) and controls (Sham) with drinking water containing 0, 1, 5, and 15 ppm F (NaF). Results are expressed as mean ± SE. *Significant differences compared to rats with access to drinking water containing 0, 1, and 5 ppm F (ANOVA, Tukey’s post hoc test, p < 0.05)
Rate of Fluoride Uptake by Bone Tissue
The rate of fluoride uptake by bone tissue was significantly higher in NX rats (5.00 ± 0.40 μmol F/l min) than in Sham-operated rats (0.55 ± 0.14 μmol F/l min, Student’s t test).
Parameters of Renal Insufficiency
As there were no significant differences in these parameters among NX rats with different levels of fluoride in water, NX0, NX1, NX5, and NX15 rats were pooled and considered as one group. Similarly, Sham-operated rats were considered as one group independently of the level of fluoride in water. Body weight increased along the time for both groups (NX = 40.07 ± 3.85) and (Sham = 45.71 ± 4.95 g/week). There were no differences in slope and intercepts.
The 24-h water intake increased in both groups along the time without differences in slope, but the intercept was higher in nephrectomized rats (46.6 ± 6.0 ml/day) than in Sham-operated rats (30.6 ± 4.3 ml/day, p < 0.05).
Although 24-h urinary flow did not change in NX and Sham-operated rats throughout the experiment, it was significantly higher in NX (20.1 ± 2.7 ml/day) than in Sham-operated rats (16.0 ± 2.2 ml/day, p < 0.05).
Urinary density did not change along the time, but was significantly lower in NX (1.05 ± 0.01 g/ml) than in Sham-operated rats (1.06 ± 0.01 g/ml, p < 0.05).
Plasma levels of urea were significantly higher in NX (49.4 ± 5.0 mg/dl) when compared to Sham-operated rats (27.9 ± 3.4 mg/dl, p < 0.05), without changes throughout time.
The clearance of creatinine measured after 60 days was significantly lower in NX rats (1.2 ± 0.3 ml/min) than in Sham-operated rats (2.5 ± 0.9 ml/min, p < 0.05).
Discussion
The oral administration of F has been shown to inhibit the secretion of insulin in the rat and human beings, thus leading to lower plasma levels of the hormone [7]. The effect was verified with isolated Langerhans islets and with slices of pancreas, indicating that F probably interferes with calmodulin, cAMP, and protein kinase C signaling pathways [5]. The administration of F in the drinking water did not produce an increase in basal levels of glucose, but tolerance to glucose after a glucose tolerance test was hindered by the presence of fluoride [7]. Regardless the age, the animals that presented an increase in bone mass had a significant decrease in plasma fluoride levels with a consequent normalization of the glucose tolerance test. However, the doses of fluoride employed in the aforementioned studies were high and unlikely to be consumed by humans. It must be pointed out that the rats metabolize fluoride faster than humans [14]. Thus, higher fluoride doses are required for rats to produce plasma fluoride levels similar to those found in humans. In this sense, the dose of 5 ppm F present in the drinking water given to rats would correspond to the fluoride levels usually found in optimally fluoridated water (∼0.8 ppm). On the other hand, the dose of 15 ppm F in the drinking water for rats would be equivalent to the presence of ∼3 ppm F in the drinking water consumed by humans, which can be found in areas of natural occurrence of fluoride in the water [15]. Additionally, considering that the kidney is the main organ responsible for the excretion of fluoride and that water fluoridation is a widespread measure to control dental caries, the possible effects of fluoride from drinking water on glucose metabolism in cases of renal deficiency surely deserves investigation.
In the experiments reported in this paper, rats with renal insufficiency received for 60 days water containing 1, 5, or 15 ppm F. The ingestion of this water produced daily fluoride intakes ranging between 0.2 and 2 mg/kg body weight, which is 40–4 times lower than the values of intake reported in previous experiments [6, 7].
As revealed by the clearance of creatinine, the rats with renal insufficiency had on average 50% of the normal renal function. Body weight, plasma levels of urea, urinary density, 24-h water intake, and 24-h urinary flow support that the rats have lower renal function.
The glomerular rate filtration is the best way to evaluate renal function. In humans, it reaches the normal value (125 ml/min per 1.73 m2) at the age of 20–30 years and then decreases approximately 1 ml/min per 1.73 m2 per year. As a consequence, in elderly people, the normal values are typically around 70–80 ml/min per 1.73 m2, which represents around 60% of the normal value. Hence, fluoride renal excretion is decreased, with the possibility of accumulation in plasma.
In the present study, neither plasma glucose levels nor glycemia after 120 min of a load of glucose were different among the experimental groups. However, plasma insulin levels increased as a function of fluoride in drinking water. In previous experiments, we demonstrated that the metabolism of glucose is perturbed when plasma fluoride concentration is higher that 5 µM [7]. In the present study, this level was not reached even in rats that received water containing 15 ppm F. As it was reported in a previous paper [7], when plasma fluoride levels return to normal levels, the pancreas secretes a mixture of insulin precursors with lower hypoglucemic activity. The results reported in this paper indicate that the intake of fluoridated water induces resistance to insulin, as it was observed in areas of fluorosis [12]. Plasma fluoride concentration did not significantly differ between NX and Sham rats with the same level of fluoride in the drinking water despite NX15 having higher values when compared to Sham. The higher uptake of fluoride by bone tissue of NX rats (5.00 ± 0.40 µmol F/l min) in comparison with Sham rats (0.55 ± 0.14 µmol F/l min) explains the similar levels of plasma fluoride concentration even with the higher urinary fluoride excretion presented by the Sham when compared to NX rats. This faster bone fluoride uptake by NX rats might be explained by the fact that they have only approximately 50% of the normal renal function. Two early complications of chronic kidney disease are vitamin D deficiency and secondary hyperparathyroidism, thus leading to increased bone remodeling [16]. Since fluoride has a high affinity for calcified tissues, this may lead to higher fluoride uptake by bone, which in turn will decrease circulating fluoride levels, reducing its possible side effects.
It is concluded that the intake of fluoridated water from water supply modifies plasma insulin levels without changes in plasma glycemia, both in controls and in rats with renal disease, after 60 days. The consumption of water with safe levels of fluoride used in the prevention of dental decay could reduce the stores of insulin. This long-term effect should be studied both in experimental animals and human beings.
References
McDonagh MS, Whiting PF, Wilson PM et al (2000) Systematic review of water fluoridation. BMJ 321:855–859
Whitford GM (1996) Metabolism and toxicity of fluoride, 2nd edn. Karger, Basel
Schmidt CW, Leuschke W (1986) Metabolism of fluorine in terminal renal failure. Urol Nephrol 79:481–484
Turner CH, Owan I, Brisendine EJ et al (1996) High fluoride intakes cause osteomalacia and diminished bone strength in rats with renal deficiency. Bone 19:595–601
Menoyo I, Rigalli A, Puche RC (2005) Effect of fluoride on the secretion of insulin in the rat. Arzneimittelforschung 55:455–460
Rigalli A, Ballina JC, Roveri E et al (1990) Inhibitory effect of fluoride on the secretion of insulin. Calcif Tissue Int 46:333–338
Rigalli A, Ballina JC, Puche RC (1992) Bone mass increase and glucose tolerance in rats chronically treated with sodium fluoride. Bone Miner 16:101–108
Chehoud KA, Chiba FY, Sassaki KT et al (2008) Effect of fluoride intake on insulin sensitivity and insulin signal transduction. Fluoride 41:270–275
De la Sota M, Puche RC, Rigalli A et al (1997) Bone mass and glucose homeostasis of subjects with high spontaneous fluoride intake. Medicina (B Aires) 57:417–420
Trivedi N, Mithal A, Gupta SK et al (1993) Reversible impairment of glucose tolerance in patients with endemic fluorosis. Diabetologia 36:826–828
Whitford GM, Sampaio FC, Pinto CS et al (2008) Pharmacokinetics of ingested fluoride: lack of effect of chemical compound. Arch Oral Biol 53:1037–1041
Gretz N, Ealdherr A, Strauch N (1993) The remnant kidney model. In: Gretz N, Strauch N (eds) Experimental and genetic rat models of chronic renal failure. Karger, Basel, pp 1–28
Rigalli A, Alloatti R, Puche RC (1999) Measurement of total and diffusible serum fluoride. J Clin Lab Anal 13:151–157
Dunipace AJ, Brizendine EJ, Zhang W et al (1995) Effect of aging on animal response to chronic fluoride exposure. J Dent Res 74:358–368
Pessan JP, Silva SM, Lauris JR et al (2008) Fluoride uptake by plaque from water and from dentifrice. J Dent Res 87:461–465
Parfitt AM (1976) The actions of parathyroid hormone on bone: relation to bone remodeling and turnover, calcium homeostasis, and metabolic bone disease. Part IV of IV parts: The state of the bones in uremic hyperaparathyroidism–the mechanisms of skeletal resistance to PTH in renal failure and pseudohypoparathyroidism and the role of PTH in osteoporosis, osteopetrosis, and osteofluorosis. Metabolism 25:1157–1188
Acknowledgments
This work was funded by a grant from Fundación Alberto J. Roemmers. The authors thank Valeria Dalmau and Agustin Ramirez by the invaluable collaboration in the surgery of induction of renal insufficiency, Hilda Moreno for fluoride measurement, and Digno Alloatti for providing the animals.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
After and intravenous dose of NaF (Do), the distribution of fluoride in the body can be represented as detailed in Fig. 4.

Distribution of fluoride in plasma, bone, and kidney after an intravenous dose (Do). [F] plasma concentration of fluoride, Vo − rate of fluoride uptake by bone tissue, Vo + rate of fluoride released from bone tissue, Vu − rate of renal fluoride excretion, Vu + rate of renal fluoride re-absorption, U cumulative urinary fluoride excretion
In this situation, the variation of plasma fluoride concentration can be represented by the following differential equation:
where
rearranging Eq. 1
After an intravenous dose of NaF, it can be supposed that Vo− > Vo+. This assumption is supported by the high plasma fluoride levels reached after the fluoride injection.
Under this consideration, Vo+ can be considered negligible; as a consequence, Eq. 2 can be written as follows:
The preceding differential equation states that after an intravenous dose of fluoride, the decrease in plasma fluoride concentration is a function of the rate of fluoride uptake by bone tissue and the renal excretion of fluoride.
It can be considered that both rates are linear functions of plasma fluoride concentration.
As a consequence
From Eqs. 3, 4, and 5, the following is obtained:
where ke is the rate constant of elimination of fluoride from plasma compartment.
Integrating both members of Eq. 7 and solving
where [F] and [F o] are the values of plasma fluoride concentration at a definite time and immediately after the injection of NaF, respectively.
Considering the initial concentration of fluoride as the ratio between the intravenous dose (Do) and the distribution volume of fluoride (V d), Eq. 8 can be rewritten as follows
Equation 9 represents the logarithm of plasma fluoride concentration as a linear function of the time. With two or more values of plasma fluoride concentration after an intravenous dose (Do), V d and ke can be obtained with the last square method of linear regression.
On the other hand, the cumulative urinary excretion of fluoride can be described by the following differential equation:
where ku is the rate constant of renal fluoride excretion. This equation states that the excretion of fluoride linearly depends on the plasma fluoride levels
Rearranging Eq. 8
and replacing in Eq. 10, the following is obtained:
Integrating both terms of equation
as U 0 = 0:
After 24 h of the mini dose of NaF, approximately 100% of fluoride not incorporated in bone tissue has been excreted in urine. The cumulative fluoride excretion after 24 h can be considered the limit of Eq. 13 when time tends to infinite. As a consequence, the limit of Eq. 13 can be written:
Solving
where [U]∞ is the cumulative fluoride excretion after 24 h of the intravenous dose. The value of ku is obtained with Eq. 14 and the values of [U]∞, Do, V d, and ke.
With the values of ke and ku using Eq. 6, ko − is obtained.
Finally, with Eq. 4 and the values of ko− and basal plasma fluoride concentration, the value of Vo− is obtained.
Rights and permissions
About this article
Cite this article
Lupo, M., Buzalaf, M.A.R. & Rigalli, A. Effect of Fluoridated Water on Plasma Insulin Levels and Glucose Homeostasis in Rats with Renal Deficiency. Biol Trace Elem Res 140, 198–207 (2011). https://doi.org/10.1007/s12011-010-8690-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-010-8690-5