
Abstract
Little is known about hair minerals in cancer patients, and serum iron level has been shown to be elevated in breast cancer patients. Therefore, the aim of this study was to evaluate hair iron and hair minerals’ level related to hair iron in breast cancer patients compared to controls. We compared hair mineral analysis data of 40 breast cancer subjects with age and body mass index-matched normal control data (n = 144) by cross-sectional analysis. All breast cancer patients were newly diagnosed at one Breast Cancer Center in Ajou University and had their hair cut before anti-cancer chemotherapy, and the normal controls (without breast cancer) also had their hair cut for various reasons in out-patient clinics of the Department of Family Practice and Community Health. Breast cancer patients had low calcium, magnesium, iron, copper, manganese, and zinc, whereas they had high arsenic, sodium, and potassium compared with the normal control. The hair iron level was positively correlated with hair calcium (r = 0.761, P < 0.001), magnesium (r = 0.643, P < 0.001), and manganese (r = 0.550, P < 0.001) and negatively correlated with arsenic (r = −0.537, P < 0.001). The hair iron level was significantly associated with the hair calcium (β = 0.778, P < 0.001) and manganese (β = 0.240, P < 0.001) by using multiple linear regression analysis. We observed different hair mineral patterns in breast cancer patients compared to normal controls. Especially, hair iron level was significantly reduced and associated with hair calcium and manganese levels.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of breast cancer, common in postmenopausal women, is rising in Korean women [1], and there are well-established risk factors such as early age at menarche, nulliparity, late first full-term pregnancy, and/or late menopause, suggesting that a long life-time exposure to estrogens contributes to breast cancer development [2]. Furthermore, it has been known that breast cancer occurs more frequently in postmenopausal women due to different serum Fe status. Because of cessation of menstrual bleeding, serum Fe levels, such as those bound to ferritin and transferrin, are two to three times higher in post- than in premenopausal women [3–5]. In contrary to western data, Korean Breast Cancer Society (2006) announced that mean age of breast cancer in Korean women was lower than that of western country women, especially that 60% of total breast cancer patients were premenopausal women [6].
Iron (Fe), an essential micronutrient and the most abundant transition metal in the human body, plays an important role in a variety of physiological functions, including oxygen transport, electron transport, energy production, and DNA synthesis [7–8]. However, as a transition metal, iron has loosely bound electrons in its atomic outer shell and catalyzes the production of reactive oxygen species, resulting in increased oxidative stress, mutations, DNA single- and double-strand breaks, and oncogenic activation [9–13].
Garland et al. found a significant inverse association between toenail iron levels and breast cancer risk among premenopausal women [14], and there are several data on serum iron of breast cancer patients; however, little data are available for the hair iron level in newly diagnosed breast cancer patients. The aim of this study was to evaluate hair iron and hair minerals’ level related to hair ion in breast cancer patients compared to the normal controls, in which hair minerals are related to the hair iron level.
Materials and Methods
Study Participants
Forty participants were recruited as newly diagnosed breast cancer patients at Breast Cancer Clinic in Ajou University Hospital, Suwon, Republic of Korea from April, 2007 to March, 2008. They had only breast cancer without any other cancer. Patients who had medical diseases such as diabetes and hypertension were not excluded. As normal controls, we chose out-patients who had no breast cancer but with same age and body mass index and had visited a clinic for some medical reasons such as fatigue, myalgia, obesity, hypertension, diabetes, and so on.
Study Design
This cross-sectional study was approved by the Institutional Review Board of Ajou University Hospital, Suwon City, Republic of Korea. All breast cancer patients received the informed consent form and agreed to provide their hair before cancer chemotherapy. Their body weight, height, and waist circumferences were measured by a trained nurse in out-patient clinic of the Department of Family Practice and Community Health. Also, we matched the normal control’s data with same age and body mass index.
Measurement of Hair Minerals
For analysis of hair minerals, all participants were asked not to chemically process their hair for at least 2 weeks. This included dyeing, perming, straightening, or frosting. The hair had also to be free of all gels, oils, and hair creams before sample collection. Approximately 300 mg of hair were obtained from four to five different locations of the posterior vertex region of the scalp using stainless steel scissors. The only proximal portion (1.5 in. closet to the root) was used as the sample. Upon cutting the sample, the hair was placed directly into a clean hair specimen envelop normally provided by the laboratory and then sealed with glue flap. The hair samples were not washed for the assays. Measurements were performed using a microwave temperature-controlled digestion technique and Perkin-Elmer Mass Spectrometer in a licensed and certified clinical laboratory that undergoes regular inspections by the Clinical Laboratory Division of the Department of Health and Human Services.
Statistical Analysis
Though original data had the unit of milligram percent, which meant that all minerals were milligrams per 100 g hair, we unified milligram percent into micrograms per gram unit to clarify standard reference. We used the independent t test for the comparison of mean values of age, body weight, and body mass index between the two groups (breast cancer patients vs normal controls), and non-parametric t test (Mann–Whitney test) was done in values without normal distribution. For the purpose of correlation between iron and other minerals, Spearman correlation (mineral without normal distribution) coefficients were used. Finally, multiple linear regression was done to evaluate which mineral was associated most with iron level. SPSS version 11.5 was used, and P < 0.05 was considered as a statistically significant value.
Results
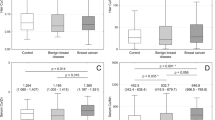
In this cross-sectional case–control study, all the breast cancer patients (n = 40) were not different in age, body weight, and body mass index (BMI; kilograms per square meter) compared to the normal controls because of age and BMI-matched control selection (Table 1). However, the results of mean value comparison between the breast cancer patients and the normal controls showed significant differences in many hair minerals, such as hair calcium, magnesium, sodium, potassium, zinc, iron, copper, manganese, lead, and arsenic (Table 2): Hair calcium, magnesium, iron, zinc, copper, manganese, and lead levels were lower in the breast cancer patients than in the normal controls. On the other hand, hair sodium, potassium, and arsenic levels were higher in the breast cancer patients than in the normal controls, thus showing that micronutrient minerals, except sodium and potassium, in hair are lower, and toxic mineral, arsenic, is higher in the breast cancer patients. In addition, the correlation between hair iron level and some other minerals showed significant difference between the two groups: The hair iron showed significant highly positive correlation with hair calcium, magnesium, and manganese and negative with arsenic in breast cancer patients (Table 3). Finally, multiple linear regression analysis revealed linear relationship between hair iron and some significantly correlated minerals in breast cancer patients: Hair iron level was linearly related significantly with hair calcium and manganese (Table 4).
Discussion and Conclusion
In the present study, we observed that hair calcium, magnesium, zinc, copper, manganese, and iron level in breast cancer patients were significantly lower and hair sodium, potassium, and arsenic were higher than in normal control. Especially, among these hair minerals, hair iron level in breast cancer patients was significantly lower than controls and was correlated with many other hair minerals such as hair calcium, magnesium, manganese, and arsenic. Hair arsenic, which is a toxic mineral, was negatively correlated, whereas the three other hair minerals, which are micronutrients minerals, were positively correlated with hair iron. Among those minerals, hair calcium and manganese were positively correlated with hair iron level in breast cancer patients, but not in normal controls (data not shown), and their levels were significantly low in breast cancer patients compared to the normal controls. In case of hair lead, hair levels in breast cancer patients were all below detection, otherwise, in normal control, 12 subjects of 144 normal subjects had detectable values, but showed within normal ranges, in which differences revealed statistical significance. Therefore, hair lead might have no significant evidence in this study.
In the previous study related to iron, The Shanghai Breast Cancer Study showed that high intake of animal-derived (heme) iron might be associated with an increased risk of primary breast cancer in Chinese women [15]. A recent case–control study nested within a cohort of 9,315 women with benign breast disease found that iron levels in breast tissue were significantly higher in women who subsequently developed breast cancer compared to breast tissue levels in controls [16]. In other study, Stevens et al. found that among women, those in whom cancer developed did not have significantly lower total iron-binding capacity or higher transferring saturation than those who remained cancer free [17]. In contrary to the results of blood and breast tissue level, Garland et al. [14] examined the association of toenail levels of iron and several other trace elements in a cohort of 62,641 women and followed up them for 4 years. Among 433 cases of breast cancer and 459 matched controls, the odds ratio comparing the highest to the lowest quintile of toenail iron adjusted for established breast cancer risk factor was 0.89 (95% CI 0.56–1.40).
There are several studies about relation between selenium and breast cancer [18–20]. Schrauzer GN proposed that selenium had an antitumorigenic effect, and low Se intake might be indicative of increased breast cancer risk. In Koreans, total intake of selenium from soil and food had been lower than other western countries like Norway [21], US [22], and the Netherlands [23]; furthermore, in the study of serum selenium level in Korean men and its association with prostatic cancer [24], the mean serum selenium level of Korean men (116.8 ng/ml) was lower than that of western men (126–136 ng/ml); this result might be associated with the lower selenium content in Korean soil and food. Similar to our study, in the hair mineral study of breast cancer [25], comparison of mean elemental contents of the breast cancer patients with controls showed a significant enhancement of chromium (P < 0.05) but declining trends for manganese (P < 0.05) in breast cancer patients.
However, there was no report for the hair iron level related to the breast cancer, especially in premenopausal women. In our study, mean age of the breast cancer patients was 47.1 years old, which might mean that most of the patients were in the premenopausal state. The difference between other studies and this study might be the mean age of the study subjects, and most of our subjects were premenopausal women compared to postmenopausal western women.
There are only a few data of hair mineral analysis in conventional medical field, even though there are numerous numbers of data on the relation between serum Fe and breast cancer. Hair mineral analysis has not generally been considered as a standard method to detect any diseases and conditions. Therefore, we could not explain the reason of why the levels of hair calcium and manganese were lower in breast cancer patients than in normal controls. Furthermore, we could not conclude whether the low hair calcium and manganese levels in breast cancer patients were related with high serum iron level. However, Cui et al. reported that the level of calcium in benign breast tissue increased and might be associated with a modest increase of subsequent breast cancer risk [19]. In another data on dairy calcium intake and risk of breast cancer, but not tissue level, low calcium intake was associated with breast cancer risk, particularly among premenopausal women [26].
Serum minerals and electrolytes are closely regulated homeostasis by the balance between serum and cellular concentration, until overt diseases occur. And, there can be no further relationship between serum minerals and hair minerals. However, hair mineral content has been known to provide some informative evidence for abnormal serum minerals and electrolytes for the previous 3 months.
We found low hair calcium and manganese levels in breast cancer patients, which were positively correlated with low hair iron level. However, we are not certain whether this explains the role of calcium and manganese in affecting the iron level in breast cancer patients. However, these two minerals, to some extent, might have some roles in the iron level. Because calcium is the most abundant of the minerals in the body, it has been known also to have numerous crucial functions in soft tissues. The active form of calcium in soft tissues is an ionized form, the content of which in blood plasma is homeostasisticly regulated within relatively narrow limits, and deviations from these narrow limits result in several disturbances, including abnormal cell membrane permeability, nerve transmission, and muscle contractions. Hair calcium, however, may be a different thing. If low hair calcium level is related to low serum level within normal limits, it may have the possibility to affect the iron metabolism, which results in various metabolic responses. As for manganese, it participates in urea formation, pyruvate transportation, and bond formation for the biosynthetic enzyme of galactotransferase. And, manganese was known as one of the cofactors in endogenous antioxidant mechanisms such as superoxide dismutase, catalases, and glutathione peroxidase. Similar to low hair calcium level, low hair manganese level showed positive correlation with low hair iron level, and there is a possible relationship with iron level.
There are some limitations in our study. Our study is a cross-sectional study, thus possibly causing selection bias. Furthermore, critical limitations include the facts that serum iron level was not measured to compare the hair iron level and that we did not adjust many other factors influencing hair mineral status such as many medical conditions, medications, pre- or postmenopausal status, cigarette smoking, alcohol consumption, exercise, and so on. In our study, however, 65% of total breast cancer patients were below 50 years old, which might mean that they were premenopausal, and this might show different breast cancer pattern compared to the western country women. Therefore, further large and prospective well-designed studies are needed to reveal the exact difference between breast cancer patients and normal controls.
In spite of these limitations, we found a small but significant difference in hair mineral patterns in breast cancer patients compared to normal controls. Hair iron level was significantly reduced in breast cancer patients. Hair calcium and manganese levels were positively correlated with hair iron level, showing low level in the hair of breast cancer patients. We could not conclude that low hair iron, calcium, and manganese levels were directly related to breast cancer; nevertheless, for further knowledge on hair mineral analysis and making evidence, analysis with large-scale populations of patients with various diseases and conditions should be performed in order to clearly establish the evidence described above.
References
Ministry of Health & Walfare, Korean Central Cancer Registry, Korean Regional Cancer Registry (Korea) (2005) Cancer incidence in Korea 1999–2001. Ministry of Health & Walfare, Gwachon, Korea
ESHRE Capri Workshop Group (2004) Hormones and breast cancer. Hum Reprod Update 10:281–293
Liu JM, Hankinson SE, Stampfer MJ, Rifai N, Willett WC, Ma J (2004) Body iron stores and their determinants in healthy postmenepausal US women. Am J Clin Nutr 78:1160–1167
Milman N, Byg KE, Ovesen L, Kirchhoff M, Jurgensen KS (2003) Iron status in Danish women, 1984–1994: a cohort comparison of changes in iron stores and the prevalence of iron deficiency and iron overload. Eur J Haematol 71:51–61
Koziol JA, Ho NJ, Felitti VJ, Beutler E (2001) Reference centiles for serum ferritin and percentage of transferring saturation, with application to mutations of the HFE gene. Clin Chem 47:1804–1810
Kim S-W, Han W-s, Jeong J, Park H-K, Noh W-C, Han S-H et al (2006) The policy proposal for effective prevention and management of breast cancer. J Breast Cancer 9:270–292
Toyokuni S (1996) Iron-induced carcinogenesis: the role of redox regulation. Free Rad Biol Med 20:553–566
Ponka P, Beaumont C, Richardson DR (1998) Function and regulation of transferring and ferritin. Sem Hematol 35:35–54
McCord JM (1998) Iron, free radicals, and oxidative injury. Sem Hematol 35:5–12
Dreosti IE (2001) Zinc and the gene: review. Mutat Res 475:161–167
Reizenstein P (1991) Iron, free radicals and cancer: a review. Med Oncol Tumor Pharmacother 8:229–233
Huang X (2003) Iron overload and its association with cancer risk in humans: evidence for iron as a carcinogenic metal. Mutat Res 533:153–171
Sahu SC (1992) Dietary iron and cancer: a review. Environ Carcino Ecotox Revs C10:205–237
Garland M, Morris JS, Colditz GA et al (1996) Toenail trace element levels and breast cancer: a prospective study. Am J Epidemiol 144:653–660
Kallianpur AR, Lee SA, Gao YT, Lu W, Zheng Y, Ruan ZX et al (2008) Dietary animal-derived iron and fat intake and breast cancer risk in the Shanghai Breast Cancer Study. Breast Cancer Res Treat 107(1):123–132
Cui Y, Vogt S, Olson N, Glass AG, Rohan TE (2007) Levels of zinc, selenium, calcium, and iron in benign breast tissue and risk of subsequent breast cancer. Cancer Epidomiol Biomarkers Prev 16(8):1682–1685
Stevens RG, Jones DY, Micozzi MS, Taylor PR (1988) Body iron stores and the risk of cancer. N Engl J Med 310:1047–1052
Schrauzer GN (2000) Anticarcinogenic effects of selenium. Cell Mol Life Sci 57:1864–1873
Schrauzer GN (2006) Interactive effects of selenium and chromium on mammary tumor development and growth in MMTV-infected female mice and their relevance to human cancer. Biol Trace Elem Res 109:281–292
Schrauzer GN (2008) Interactive effects of selenium and cadmium on mammary tumor development and growth in MMTV-infected female mice. A model study on the roles of cadmium and selenium in human breast cancer. Biol Trace Elem Res 123:27–34
Ringstad J, Jacobsen BK, Tretli S, Thomassen Y (1988) Serum selenium concentration associated with risk of cancer. J Clin Pathol 41:454–457
Willet WC, Polk BF, Morris JS, Stampfer MJ, Pressel S, Rosner B et al (1983) Prediagnostic serum selenium and risk of cancer. Lancet 2:130–134
Kok FJ, de Bruijn AM, Hofman A, Vermeeren R, Valkenburg HA (1987) Is serum selenium a risk factor for cancer in men only? Am J Epidemiol 125:12–16
Song S-H, Song K-H, Lee S-B, Kim C-S (2006) The serum selenium level in Korean men and its association with age and prostate cancer. Korean J Urol 47:150–153
Kilic E, Saraymen R, Demiroglu A, Engin OK (2004) Chromium and manganese levels in the scalp hair of normals and patients with breast cancer. Biol Trace Elem Res 102:19–26
Kesse-Guyot E, Bertrais S, Duperray B, Arnault N, Bar-Hen A, Galen P et al (2007) Dairy products, calcium and the risk of breast cancer: results of the French SU.VI.MAX prospective study. Ann Nutr Metab 51:139–145
Acknowledgment
We thank the TEI Korea (Trace Element Inc.) company for the hair mineral analysis in breast cancer patients for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joo, NS., Kim, SM., Jung, YS. et al. Hair Iron and Other Minerals’ Level in Breast Cancer Patients. Biol Trace Elem Res 129, 28–35 (2009). https://doi.org/10.1007/s12011-008-8281-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-008-8281-x