
Abstract
Selected trace metals were analyzed in human malignant and nonmalignant (benign) breast tissue samples by the flame atomic absorption spectrophotometric method. In malignant tissues, dominant mean concentrations were revealed by Na, K, Ca, Mg, Fe, Zn, and Al at 927, 552, 231, 61.7, 36.5, 18.3, and 8.94 μg/g, respectively, while the mean metal levels in benign tissues were 903, 435, 183, 63.3, 24.7, 14.5, and 10.1 μg/g, respectively. Average concentrations of Cd, Co, Cr, Cu, Fe, Mn, K, Ca, and Zn were noted to be significantly higher in the malignant tissues compared with the benign tissues. Significantly strong correlations (r > 0.50) in malignant tissues were observed between Mn and Co, Mn and Cd, Cd and Cr, Fe and Mn, Cd and Co, Fe and Co, Mg and Pb, Cd and Fe, Mg and Ni, Pb and Ni, Ni and Sr, and Fe and Pb, whereas, Cd and Co, Cd and Mn, Co and Mg, Co and Mn, Cu and Mn, Co and Ni, Mg and Ni, Cd and Cu, Cd and Ni, Ca and Mg, Mn and Pb, Cu and Ni, Fe and Ni, Cd and Mg, Co and Cu, Cr and Na, and Cd and Cr revealed strong and significant relationships in benign tissues at p < 0.001. Principal component analysis of the metals data yielded six principal components for malignant tissues and five principal components for benign tissues, with considerably different loadings, duly supported by cluster analysis. The study revealed a considerably different pattern of distribution and mutual correlations of trace metals in the breast tissues of benign and cancerous patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the last few decades, there has been increasing interest in exploring the exact role of trace metals in human health and diseases. Although trace metals constitute a minor part of living tissues, they play several vital roles in biological systems such as stabilizers, elements of structure, essential minerals for hormonal function, and cofactors in enzymes [1]. The role of different trace metals in the normal vital activities and initiation of some diseases has long been known, and it is assumed that all chemical elements are involved in physiological processes in varying degrees [2, 3]. Any change in the environment as well as in the human body itself can trigger changes in trace metal composition of any organ or tissue, and as a consequence, potentially toxic chemical species may be accumulated, due to which some disease can be produced [4]. Various diseases of previously unknown etiology have been attributed to an imbalance of trace metals [5–7]. It may be assumed that trace metals influence the mechanisms that are responsible for the development of cancer because of their fundamental importance in a number of biochemical and physiological processes in humans [6, 8–9].
Although cancer was mainly considered to be genetically related, it is now well acknowledged that other factors such as diet and environment significantly affect the cancer incidences [10, 11]. It has been reported that human breast cancerous tissues fragments of mouse mammary tumor virus (MMTV) or a closely related ribonucleic acid virus have been detected in a significant percentage, signifying that breast cancer can also have a viral etiology [12, 13]. Epidemiological studies showed that the majority of the factors leading to the development of malignant tumor in humans have arisen from environmental factors including the work environment, followed by nutritional habits as well as viral attacks and only meagerly as consequences of genetic predispositions [14, 15]. Several studies have focused on the relationship between trace metal and breast cancer in humans, which indicated that the trace metals may influence the carcinogenic process [16–23].
The present study is carried out to evaluate the comparative trace metal distribution and correlation in the malignant and benign breast tissues. Multivariate methods have been used for the apportionment of the trace metals in the two groups of donors [4, 24–26].
Materials and Methods
In the present study, subjects were selected from the patients admitted in hospitals of Rawalpindi district, Pakistan namely, POF Hospital, Wah Cantt, and Christian Hospital, Taxila. The breast tissue samples from the patients were collected prior to any chemo- or radiotherapy, and the diagnosis of primary carcinoma was confirmed histologically. During the present study, a total of 53 malignant breast tissue samples were collected from the patients, aged between 35 and 64 years. The benign subjects (n = 61) were selected from the same localities with matched age groups, aged between 36 and 59 years. The tissue samples were collected during the surgery and stored at −20°C in a zip-mouthed high-density polythene bag duly labeled with relevant codes related to the donor’s name, age, eating and drinking habits, and social and general health status, all recorded and compiled on regular proforma at the time of sampling [27, 28]. Before the digestion, the samples were partially thawed, and the thick sections of the surrounding fatty tissues, blood vessels, and membranes, which could have been contaminated in any of the earlier stages, were removed carefully. The tissue samples were digested with nitric acid–perchloric acid (10:5 v/v) mixture with subsequent heating to a soft boil until white dense fumes evolved. Samples were then cooled to room temperature and diluted to a proper volume with doubly distilled water [29, 30]. The blank was prepared the same way but without the tissue sample.
All reagents used were of ultrahigh purity (certified greater than 99.99%) procured from E-Merck. Working solutions were prepared by serial dilution of 1,000-ppm standard solutions. Quantitative analysis was carried out on flame atomic absorption spectrophotometer (Shimadzu AA-670, Japan), with automatic background compensation and under optimum analytical conditions. The samples were analyzed for 18 metals: Al, Ca, Cd, Co, Cr, Cu, Fe, K, Li, Mg, Mn, Mo, Na, Ni, Pb, Sb, Sr, and Zn.
Three subsamples of each sample were treated and run separately onto the spectrophotometer to pool mean metal concentrations. A parallel routine check on the accuracy of quantified results was ensured through the use of a standard reference material (SRM, OL-96). The samples were also analyzed at an independent laboratory for the comparison of the results. A maximum of 5% difference was observed in the results of two laboratories. STATISTICA software was used for statistical analyses of the metal data [31].
Results and Discussion
The statistical distribution parameters for metal concentrations (μg/g, wet weight) in the malignant breast tissues (n = 53) are presented in Table 1. On the average, higher concentrations were shown by Na (927 μg/g), K (552 μg/g), Ca (231 μg/g), Mg (61.7 μg/g), Fe (36.5 μg/g), and Zn (18.3 μg/g), followed by Al (8.94 μg/g) and Pb (8.23 μg/g), Sb (4.76 μg/g), Sr (4.54 μg/g), Cu (3.47 μg/g), Co (2.37 μg/g), Ni (1.87 μg/g), Mo (1.61 μg/g), and Cd (1.21 μg/g). Relatively lower average levels in the malignant tissues were observed for Cr, Li, and Mn. Overall, the trace metals in malignant tissues exhibited following decreasing order in their average concentrations: Na > K > Ca > Mg > Fe > Zn > Al > Pb > Sb > Sr > Cu > Co > Ni > Mo > Cd > Cr > Li > Mn. Most of the selected metals exhibited highly asymmetric distribution as shown by appreciably divergent mean and median values on one hand and large SD and SE values on the other hand. A large value of SD reflected a large spread of metal distribution, as noted in the cases of Na, K, Ca, Mg, Fe, Zn, and Pb. Some of the trace metals (Li, Mn, Cr, Mo, and Ni) exhibited relatively normal distribution pattern, evidenced by comparative low SD and SE values. Somewhat lower values of skewness were noted in favor of Al, Mo, Sb, and Ni, thus manifesting an almost symmetrical distribution pattern of these metals in malignant tissues; however, relatively large asymmetry in the distribution of other metals was evidenced by higher skewness values. The range of the selected trace metals also exhibited a wide spread in their concentrations in the malignant breast tissues.
The statistical parameters indicating the distribution of selected trace metal contents (μg/g, wet weight) in benign breast tissues (n = 61) are presented in Table 2. On the average, higher levels were shown by Na (903 μg/g), K (435 μg/g), Ca (183 μg/g), Mg (63.3 μg/g), Fe (24.7 μg/g), Zn (14.5 μg/g), and Al (10.1 μg/g), followed by Pb (7.41 μg/g), Sb (4.25 μg/g), Sr (4.11 μg/g), Ni (2.08 μg/g), Cu (1.83 μg/g), Mo (1.57 μg/g), and Co (1.35 μg/g). Somewhat lower concentration levels were observed for Li, Cd, Cr, and Mn. On the average basis, the decreasing trend of metal levels in the tissues of benign patients revealed following order: Na > K > Ca > Mg > Fe > Zn > Al > Pb > Sb > Sr > Ni > Cu > Mo > Co > Li > Cd > Cr > Mn. Most of the selected metals exhibited a large dispersion and asymmetry in their distribution as shown by relevant SD, SE, range, and skewness values. A large dispersion of the metals data in terms of SD were noted in the cases of Na, K, Ca, Mg, Fe, Pb, and Zn. Trace metals such as, Mn, Cr, Li, Cd, and Mo exhibited comparatively homogenous distribution pattern, as indicated by small SD and SE values. Lower magnitude of skewness in favor of Al, Sb, and Li manifested an almost symmetrical distribution pattern of these metals in the tissues of benign patients, whereas a large asymmetry in the distribution of Pb, Cr, and Ni was evidenced by the highest skewness values.
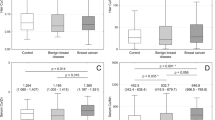
A systematic and detailed comparison of the average concentration levels of trace metals measured in the malignant and benign breast tissues are shown graphically in Fig. 1. In the case of similar average values of concentrations, generally, the data on these plots are grouped along the diagonal line, while deviations from the diagonal line indicate the pragmatic differences of average concentrations. Among the selected trace metals, the statistically significant differences between malignant and benign tissues were observed for the metals, which are shown in bold italic. More detailed results of the statistical tests revealed an increase in the average concentrations of Mn (256%), Cd (209%), Cr (203%), Cu (190%), Co (176%), Fe (148%), K (127%), Ca (126%), and Zn (126%) in the malignant breast tissues as compared to the benign breast tissues. The concentrations of Al, Li, Mg, Mo, Na, Ni, Pb, Sb, and Sr exhibited a nonsignificant disparity in their average levels in the tissues of the two donor groups.

Comparison of average concentrations of trace metals observed in malignant and benign breast tissues. Statistically significant differences at 95% confidence level were found for the metals shown in bold italic
In earlier studies, mean concentrations of Cr, Ca, Fe, Cu, and Zn were reported to be significantly higher in malignant and benign breast tissues compared with the controls [19, 22, 32]. In another study [33], it was suggested that reactive chromium intermediates such as Cr(V) and Cr(IV) generate hydroxyl radicals, which cause deoxyribonucleic acid (DNA) strand breaks, base modification, and lipid peroxidation and also inactivate p53. Similar trends were reported in the blood and scalp hair samples of breast cancer patients [17,18,34]. Moreover, Cr and Zn had been reported to be significantly higher in the blood of breast cancer patients as compared with healthy donors [17]. Breast cancer mortality was found to be strongly contributed by Cr, followed by Cd and Zn [21, 23, 35]. Schrauzer et al. reported that age-corrected breast cancer mortalities in different countries were directly correlated with the estimated dietary intake of Zn, Cr, and Cd and inversely correlated with Se and subsequently demonstrated that Zn, Cd, and Cr abolish the cancer-protecting effects of Se in MMTV-infected C3H mice [36, 37]. The observed elevated concentrations of Cr, Cd, and Zn in the malignant breast tissues, in the current study, are supported by the above-explained carcinogenicity processes.
The excessive accumulation of Fe in humans may be associated with an increased risk of cancer [38]. It causes tissue damage by acting as a catalyst in the conversion of hydrogen peroxide to free radical ions, which attack cellular membranes, cause DNA strand breaks, inactivate enzymes, depolymerize polysaccharides, and initiate lipid peroxidation [39, 40]. Appreciably higher levels of Cu were found in malignant plasma than the plasma of healthy donors, which could induce growth proliferation and cancer by damaging DNA with free hydroxyl radicals [20, 41]. The elevated Cu levels observed in the malignant breast tissues probably promote breast cancer through angiogenesis and oxidative DNA damage [42, 43]. Slightly higher Pb levels in the malignant breast tissues compared with the normal tissues have been reported in a US study [32]. Majewska et al. [16] have reported enhanced concentrations of many trace elements in malignant breast tissues and suggested that these elements compete for the binding sites in the cell, change its enzymatic activity, and exert direct or indirect action on the carcinogenic processes, accelerating the growth of tumors, and that the inhibition of enzymes caused by the variation in trace element concentrations results in the immunological breakdown of the body system.
The Spearman correlation coefficient matrix of selected trace metals in malignant breast tissues is given in Table 3. The significant correlation (r) values between the metal pairs are shown in italics at p < 0.001. Strong positive correlations were noted between, Co and Mn (r = 0.88), Cd and Mn (r = 0.75), Cd and Cr (r = 0.75), Fe and Mn (r = 0.74), Cd and Co (r = 0.73), Co and Fe (r = 0.69), Mg and Pb (r = 0.65), Cd and Fe (r = 0.64), Ni and Pb (r = 0.63), Mg and Ni (r = 0.63), and Ni and Sr (r = 0.55). Some significant but weak correlations were also found between Fe and Pb (r = 0.50), Fe and Mg (r = 0.48), Cr and Mn (r = 0.46), Fe and Ni (r = 0.46), K and Mg (r = 0.46), Al and Mg (r = 0.43), Co and Cr (r = 0.44), Fe and K (r = 0.41), Co and Ni (r = 0.41), and Ca and Sr (r = 0.41). All other metal pairs exhibited nonsignificant positive or negative relationships, which manifested their independent variations in the tissues of breast cancer patients. This simple correlation study revealed that toxic metals, such as Cd, Cr, Co, Mn, and Fe, demonstrated strong mutual relationships and thus contributed mainly toward the carcinogenic processes, while significant correlations among Mg, Pb, Ni, and Sr indicated their common variations in the tissues of breast cancer patients. This correlation study also pointed out the independent origin of the aforementioned two groups of metals in the malignant tissues. These differences may be attributed to the altered metabolism of selected trace metals in the tissues of breast cancer patients, which will be further explored by multivariate methods in a forthcoming discussion.
The data on metal-to-metal Spearman correlations in benign tissues are given in Table 4, wherein significant values are shown in italics, at p < 0.001. Strong positive correlations were noted between following metal pairs: Cd–Mn (r = 0.82), Cd–Co (r = 0.82), Co–Mg (r = 0.74), Co–Mn (r = 0.69), Cu–Mn (r = 0.68), Co–Ni (r = 0.64), Mg–Ni (r = 0.63), Cd–Cu (r = 0.61), Cd–Ni (r = 0.61), Ca–Mg (r = 0.59), Mn–Pb (r = 0.57), Fe–Ni (r = 0.54), Cu–Ni (r = 0.54), Cd–Mg (r = 0.52), Co–Cu (r = 0.51), Cr–Na (r = 0.51), and Cd–Cr (r = 0.51). In addition, weakly significant correlations were also found between Ca and Co, Ca and K, Ca and Sr, Cd and Fe, Cd and K, Cd and Pb, Co and Fe, Co and K, Cr and Cu, Cr and K, Cu and K, Cu and Mg, Fe and Mg, K and Ni, Mg and Mn, Mn and Ni, and K and Na. This correlation study revealed that Ca and Mg are contributed by a common origin, while strong correlations among Cd, Cu, Co, Ni, and Mn indicated their mutual variations in the benign breast tissues. All other metal pairs exhibited very weak relationship between them. A few negative correlations were also observed, but they were not significant.
The present study takes up metal apportionment and source identification in the tissues of the two groups of donors using principal component analysis (PCA) and cluster analysis (CA) [4, 24–26]. The principal component (PC) loadings of selected trace metals in malignant tissues were extracted by using varimax-normalized rotation on the data set, as shown in Table 5. The PCA of the trace metal data in the malignant tissues yielded six PCs with eigen values greater than 1, commutatively containing more than 73% of the total variance of the data. The CA of the selected metal data pertaining to the tissues of breast cancer patients is shown in Fig. 2a, which revealed very strong clusters of Cd–Cr–Co–Mn–Fe and Mg–Pb–Ni. For malignant breast tissues, PC 1 showed higher loadings for Cd, Co, Cr, Fe, and Mn, with a similar strong cluster. These trace metals are believed to share some common source in the malignant tissues as pointed out earlier by the correlation study, and this group of metals was mainly considered to contribute toward the carcinogenesis. PC 2 showed higher loadings of Mg, Ni, Pb, and Zn, and one of the clusters is also composed of Mg, Ni, Pb, and Zn. These metals also manifested a unidirectional relationship in the correlation study. CA revealed a common cluster of Na and K, which contribute to PC 3, along with the significant loadings of Mo and Ca. In the same way, PC 6 exhibited higher loadings for Ca and Cu, sharing a common cluster with the addition of Sr, which showed higher loadings to PC 4 along with Sb and significant loadings of Ni, whereas PC 5 showed maximum loadings only for Li. Overall, CA is in good agreement with PCA findings, and both these multivariate methods revealed some mutual variations, depletion, and uptake of different selected trace metals in the malignant breast tissues.

Cluster analysis of selected metals in a malignant and b benign breast tissues
The PC loadings, extracted by using varimax-normalized rotation on the data set of trace metals in the benign breast tissues, are shown in Table 6. The PCA of the data set yielded five PCs with eigen values greater than 1, commutatively explaining almost 69% of the total variance of selected trace metals in the tissues of benign patients. The CA of the metal data pertaining to benign tissues is shown in Fig. 2b, which exhibited very strong clusters of Cd–Co–Cu–Fe–Mg–Mn–Ni–Pb, Cr–K–Na, Zn–Li, and Sb–Al. In the benign tissues, PC 1 showed higher loadings for Cd, Co, Cu, Fe, Mg, Mn, Ni, and Pb, with similar strong cluster of CA. This PC of mostly carcinogenic metals showed the contribution from environmental pollutants [4, 19]. For PC 2, higher loadings for Cr, Cu, K, and Na were observed duly supported by CA. This group of the metals is mainly believed to be controlled by internal body metabolism. One important aspect of such a grouping evidenced that toxic metals such as Cr grouped together with main electrolytes of the human body, Na and K. This may lead to malfunctioning in the normal metabolic processes. Another important feature is that Cu showed the significantly higher loadings in both PC 1 and PC 2, thus evidencing its contribution from two different sources. Similarly, PC 3 revealed higher loadings of Ca and Sr, and PC 4 showed elevated loadings for Al and Sb; likewise, PC 5 exhibited significantly higher loadings of Li, Zn, and Mo. The CA is in very good agreement with the PCA results.
In conclusion, the present study brings out marked differences in the distribution and correlations of selected trace metals in the malignant breast tissues compared with the benign breast tissues. Major contributions were noted for Na, K, Ca, Mg, Fe, Zn, Al, and Pb in both categories. Although most of the trace metals revealed comparatively higher concentrations in the malignant breast tissues, the mean levels of Cd, Co, Cr, Cu, Fe, Mn, K, Ca, and Zn were significantly higher in the malignant than benign breast tissues. The correlation study manifested significantly strong relationships among Cd, Cr, Co, Mn, and Fe in the malignant breast tissues, which were considerably different than the correlation coefficients observed in the benign tissues. PCA showed the significantly different apportionment mechanism of trace metals in the malignant and benign breast tissues with six and five PCs, respectively, duly supported by the CA findings. These discrepancies were mainly attributed to the buildup of the trace metal concentrations in the malignant tissues, which results in the alteration of body metabolism in the cancer patients.
References
Feinendegen LE, Kasperek K (1980) Medical aspects of trace element research. In: Bratter P, Schramel P (eds) Trace element analytical chemistry in medicine and biology. Walter de Gruyter, Berlin, pp 1–17
Peereboom JWC (1985) General aspects of trace elements and health. Sci Total Environ 42:1–27
Rao AN (2005) Trace element estimation—methods and clinical context. Online J Health Allied Sci 4:1–9
Shtangeeva I, Kulikov V (1995) Study of chemical element behaviour in health and disease by means of neutron activation analysis and multivariate statistics. Nutrition 11:592–594
Swierenga SHH, Gilman JPW, McLean JR (1987) Cancer risk from inorganics. Cancer Metastasis Rev 6:113–154
Bower JJ, Leonard SS, Shi X (2005) Conference overview: molecular mechanisms of metal toxicity and carcinogenesis. Mol Cell Biochem 279:3–15
Yaman M (2006) Comprehensive comparison of trace metal concentrations in cancerous and non-cancerous human tissues. Curr Med Chem 13:2513–2525
Schwartz MK (1975) The role of trace element in cancer. Cancer Res 35:3481–3487
Snow ET (1992) Metal carcinogenesis: mechanistic implications. Pharmac Ther 53:31–65
Feldman EB (1993) Dietary intervention and chemoprevention—1992 perspective. Prev Med 22:661–666
Bowen P (2000) Dietary intervention strategies: validity, execution and interpretation of outcomes in nutrition and cancer prevention. Kluwer, Dordrecht
Pogo BGT, Holland JF (1997) Possibilities of a viral etiology for human breast cancer. Biol Trace Elem Res 56:131–142
Tsai JH, Tsai CH, Cheng MH, Lin SJ, Xu FL, Yang CC (2004) Association of viral factors with non-familial breast cancer in Taiwan by comparison with non-cancerous, fibroadenoma, and thyroid tumor. J Med Virol 75:276–281
Weinstein IB (1988) The origins of human cancer. Cancer Res 48:4135–4143
Clemens MR (1991) Free radicals in chemical carcinogenesis. J Mol Med 69:1123–1134
Majewska U, Braziewicz J, Banas D, Kukus KA, Gozdz S, Pajek M, Smok J, Urbaniak A (1997) An elemental correlation study in cancerous breast tissue by total reflection X-ray fluorescence. Biol Trace Elem Res 60:91–100
Singh V, Garg AN (1998) Trace element correlations in the blood of Indian women with breast cancer. Biol Trace Elem Res 64:237–245
Kilic E, Saravmen R, Demiroglu A, Ok E (2004) Chromium and manganese levels in the scalp hair of normals and patients with breast cancer. Biol Trace Elem Res 102:19–25
Raju GJN, Sarita P, Kumar MR, Murty GAVR, Reddy BS, Lakshminarayana S, Vijayan V, Lakshmi PVBR, Gavarasana S, Reddy SB (2006) Trace elemental correlation study in malignant and normal breast tissue by PIXE technique. Nucl Instrum Methods Phys Res B 247:361–367
Dabek JT, Hyvonen DM, Harkonen M, Adlercreutz H (1992) Evidence for increased non-ceruloplasmin copper in early stage human breast cancer serum. Nutr Cancer 17:195–201
Hayes RB (1997) The carcinogenicity of metals in humans. Cancer Cause Control 8:371–385
Siddiqui MKJ, Jyoti, Singh S, Mehrotra PK, Singh K, Sarangi R (2006) Comparison of some trace elements concentration in blood, tumor free breast and tumor tissues of women with benign and malignant breast lesions: an Indian study. Environ Int 32:630–637
Schrauzer GN (2006) Interactive effects of selenium and chromium on mammary tumor development and growth in MMTV-infected female mice and their relevance to human cancer. Biol Trace Elem Res 109:281–292
Hopke PK (1992) Factor and correlation analysis of multivariate environmental data. In: Hewitt CN (ed) Methods of environmental data analysis. Elsevier, London, pp 139–180
Jackson JE (1991) A user’s guide to principal components. Wiley, New York
Jobson JD (1991) Applied multivariate data analysis. Springer, New York
Katoh Y, Sato T, Yamamoto Y (2002) Determination of multielement concentrations in normal human organs from the Japanese. Biol Trace Elem Res 90:57–70
Aitio A, Jarvisalo J, Stoeppler M (1994) Sampling and sample storage. In: Herber RFM, Stoeppler M (eds) Trace element analysis in biological specimens. Elsevier, Amsterdam, pp 3–13
Sansoni B, Panday VK (1994) Sample treatment of human biological materials. In: Herber RFM, Stoeppler M (eds) Trace element analysis in biological samples. Elsevier, Amsterdam, pp 21–52
Rahil-Khazen R, Bolann BJ, Ulvik RJ (2002) Correlations of trace element levels within and between different normal autopsy tissues analysed by inductively coupled plasma atomic emission spectrometry. Biometals 15:87–98
StatSoft (1999) STATISTICA for Windows. Computer program manual. StatSoft, Tulsa, OK
Rizk SL, Sky-Peck HH (1984) Comparison between concentrations of trace elements in normal and neoplastia human breast tissue. Cancer Res 44:5390–5394
Wang S, Leonard SS, Ye J, Ding M, Shi X (2000) The role of hydroxyl radical as a messenger in Cr(VI)-induced p53 activation. Am J Physiol Cell Physiol 279:C868–C875
Zhao C, Yang J, Li X, Chen S, Chen J (1993) Analysis of trace elements in scalp hair of healthy people, breast cancer and hyperplasia patients with XRF method. J West China Univ Med Sci 24:402–404
Drasch G, Schopfer J, Schrauzer GN (2005) Selenium/Cadmium rations in human prostrates. Indicators for prostate cancer risk of smokers and non-smokers and relevance to the cancer protective effects of selenium. Biol Trace Elem Res 103:103–107
Schrauzer GN, White DA, Schneider CJ (1977) Cancer mortality correlation studies—IV: associations with dietary intakes and blood levels of certain trace elements, notably Se-antagonists. Bioinorg Chem 7:35–56
Schrauzer GN (2008) Interactive effects of selenium and cadmium on mammary tumor development and growth in MMTV-infected female mice. A model study on the roles of cadmium and selenium in human breast cancer. Biol Trace Elem Res, DOI 10.1007/s12011-008-8091-1
Reddy SB, Charles MJ, Raju GJN, Reddy BS, Reddy TS, Lakshmi PVBR, Vijayan V (2004) Trace elemental analysis of cancer-afflicted intestine by PIXE technique. Biol Trace Elem Res 102:265–281
Andrews NC (1999) Disorders of iron metabolism. N Engl J Med 341:1986–1995
McCord JM (1996) Effects of positive iron status at a cellular level. Nutr Rev 54:85–88
Gupta SK, Shukla VK, Vaidya MP, Roy SK, Gupta S (1993) Serum and tissues trace elements in colorectal cancer. J Surg Oncol 52:172–175
Brem S (1999) Angiogenesis and cancer control: from concept to therapeutic trial. Cancer Control 6:436–458
Hu GF (1998) Copper stimulates proliferation of human endothelial cells under culture. J Cell Biochem 69:326–335
Acknowledgments
The funding by Higher Education Commission, Government of Pakistan, to carry out this project is gratefully acknowledged. We are also thankful to the administration of POF Hospital, Wah Cantt, and Christian Hospital, Taxila, for their invaluable help during the sampling.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pasha, Q., Malik, S.A., Iqbal, J. et al. Comparative Evaluation of Trace Metal Distribution and Correlation in Human Malignant and Benign Breast Tissues. Biol Trace Elem Res 125, 30–40 (2008). https://doi.org/10.1007/s12011-008-8158-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-008-8158-z