
Abstract
The aim of the study was to investigate the association between serum selenium levels in patients with gestational diabetes mellitus (GDM) and glucose intolerants and compare them with those of glucose-tolerant pregnant women. This cross-sectional study was prospectively performed in a total of 178 pregnant women undergoing a 50-g oral glucose tolerance test between 24 and 28 weeks of gestation who were grouped according to their status of glucose tolerance as with gestational diabetes (group A, abnormal 1- and 3-h glucose tolerance test; n = 30), glucose intolerant (group B, abnormal 1-h but normal 3-h glucose tolerance test; n = 47), or normal controls (group C, normal 1-h glucose test; n = 101). Serum selenium levels were measured with a graphite furnace atomic absorption spectrophotometer using a matrix modifier. Median maternal age and gestational age at the time of diagnosis in group A (gestational age = 24.8 [24–27]), group B (gestational age = 24.7 [24–27]), and group C (gestational age = 25 [24–28]) did not differ. Patients with gestational diabetes mellitus and those with glucose intolerants had lower selenium level than that of the normal pregnant women (P < 0.001). There was a significant inverse correlation between selenium and blood glucose level, and also selenium supplementation might prove beneficial on patients with GDM and prevent or retard them from secondary complications of diabetes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Kuhl [1] indicated that gestational diabetes mellitus (GDM) is one of the most prevalent complications of pregnancy and a temporary form of type 2 diabetes that occurs in about 2–3% of all pregnant women. It is like type 2 diabetes and carries risk for the mother and the fetus, and high blood glucose levels are harmful to developing child and must be carefully managed. Gestational hyperglycemia induces oxidative stress in the mother and the fetus that may be correlated to adverse fetal outcomes (fetal distress, macrosomia, or other congenital anomalies) [2, 3].
Many of the benefits of selenium are related to its role as a cofactor in the production of glutathione peroxidase (GP), an antioxidant enzyme that helps detoxify the body and protects the cell against oxidative damage by peroxides produced from lipid metabolism. GP, which holds about 60% of the selenium in the body, is the most abundant selenium-containing protein in mammals. Selenium, a common dietary supplement, is an antioxidant material that helps prevent harmful effects of free radicals, molecules that can damage cell membranes and genetic material and contribute to the development of cancer and heart disease. Selenium is involved in processes that protect the cell against oxidative damage by peroxides produced from lipid metabolism [4]. There is an increased requirement for selenium during pregnancy, presumably for fetal growth, which manifests as decreasing maternal blood and tissue selenium concentrations [5, 6]. These decreases are greater in pregnant women with gestational or pre-existing diabetes. A lower level of selenium has been described in GDM, and it has been shown that there was a inverse relationship with this trace element status and glucose tolerance [5–9].
In light of these premises, the aim of this study was to investigate the association level of serum selenium in Turkish pregnant women with GDM, glucose intolerants, and glucose-tolerant pregnant women.
Materials and Methods
Subjects
This cross-sectional study was performed at the Kahramanmaras Sutcu Imam University, Department of Obstetrics and Gynecology, between June 2002 and December 2003. Research ethics approval was obtained before the initiation of the study, and signed informed consents were obtained from all patients and volunteers. Subjects were eligible for the study if they were nonsmokers, had no history of hypertension and personal history of cardiovascular disease, had no previous medical history of diabetes, had no personal or family history of deep venous thrombosis, were not taking any medication (apart from iron supplementation), and had no known vitamin deficiency and prior significant medical illnesses. Women who had taken any vitamin supplements 2 weeks before the test were excluded.
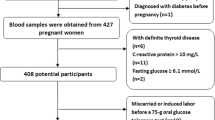
The study population consisted of 178 pregnant women between 24 and 28 weeks of gestation, which were divided into three groups according to their status of glucose tolerance. In our institution, we routinely survey our patients between 24 and 28 weeks of gestation with a 50-g oral glucose tolerance test (OGTT). All glucose tolerance tests were done in fasting status. Patients are considered negative (normal) when their postprandial serum glucose level is less than 140 mg/dl. If their 1-h postprandial serum glucose concentration is greater than or equal to 140 mg/dl, they receive a 3-h 100-g OGTT. To ensure consistency, all patients are instructed to add 150 g of carbohydrate to their usual meals for 3 days before the 100-g OGTT. Blood samples are collected at 08:00 hours (after 12 h of fasting) and at 60, 120, and 180 min after glucose ingestion. The diagnosis of gestational diabetes is based upon the criteria of Coustan and Carpenter [10] by which after a 100-g oral glucose load, two or more of the following plasma values were met or exceeded: fasting 95 mg/dl, 1 h 180 mg/dl, 2 h 155 mg/dl, and 3 h 140 mg/dl.
Blood Sampling
Fasting venous blood specimens were drawn from the antecubital vein and collected in no-additive vacutainer (Becton-Dickinson, Franklin Lakes, NJ) blood-collecting tubes according to standard hospital guidelines for venipuncture and sample collection. The serum separator tube specimens were allowed to clot and then were centrifuged for 10 min at 3,000 × g to separate the serum. Serum glucose levels were measured with a same-day-calibrated autoanalyzer, and the serum was stored at −20°C until analysis of selenium levels.
Serum Selenium Levels
Selenium measurement was done in graphite furnace atomic absorption spectrophotometer (Perkin Elmer Analyst 800) using Zeeman background correction. We used palladium (4 μg in 20-μL sample) and magnesium sulfate (3 μg in 20-μL sample) as matrix modifiers. Samples and calibration standards were diluted 1 in 3 with 0.05% Triton X- 100 to improve sample viscosity and reproducibility of the results. All groups’ selenium levels were evaluated to standard deviation. Selenium calibration standards were prepared from the commercial Se standard (1,000 mg/L) by serial dilutions.
Statistical Analyses
For the statistical analysis of the mean, median, standard deviation, ratios, and correlation tests of the data, SPSS 11.5 statistical package was used. The normality of distributions of variables were analyzed by Kolmogorov–Smirnov equality of distribution test. The Kruskall–Wallis test was used for statistical significance of differences in non-normal distributed variables among groups, and the Bonferroni post-hock test was used for multiple comparisons when significant result was obtained. A P value of less than 0.05 was considered statistically significant.
Results
Group A (gestational age = 24.8 [24–27] weeks) included 101 pregnant women with a normal 50-g glucose tolerance test. Group B (gestational age = 24.7 [24–27] weeks) included 30 pregnant women with an abnormal 50-g and abnormal 100-g OGTT. Group C (gestational age = 25 [24–28] weeks) included 47 women with an abnormal 50-g OGTT but normal 100-g OGTT. The median age of the patients were 26.8 (18–34), 28.2 (18–37), and 27.4 (18–35) years in groups A, B, and C, respectively.
Serum selenium levels of GDM, glucose intolerants, and normal controls are shown in Table 1 and Fig. 1. There was a significant difference between serum selenium levels of GDM and controls and also between serum selenium levels of glucose intolerants and controls (P < 0.001).

Serum selenium levels in pregnant women with gestational diabetes (GDM), glucose intolerants (GIT), and control groups
Discussion
In Turkey, approximately 27.4% of women are at reproductive age seen in (approximately 18 million). The rate of obesity is approximately 30% among the women. Estimated prevalence of gestational diabetes range is 3–4%, and the childbearing rate is 2.4%. These results show us that more than 17,000 women have GDM in Turkey [11]. Our city, Kahramanmaras, with a population of one million with environs, has more than 250 women with GDM in a year. This number is remarkably high, and GDM has a particular importance as a health problem [12–15]. GDM is in close relationship with body weight and BMI. Obesity is associated with diabetes mellitus [16], and insulin resistance has been very commonly seen.
Diabetes causes oxidative stress, which damages the insulin-producing cells of the pancreas in rats, which can worsen diabetes [17]. Oxidative stress plays a role during pregnancy and normal parturition and in initiation of preterm labor [18, 19]. The pathological effects are exerted by various mechanisms including lipid damage, inhibition of protein synthesis, and depletion of adenosine triphosphate. This situation can cause harmful effects in women and their fetuses. Oxidative effects balance is maintained by the presence of adequate amount of antioxidants. Superoxide dismutase, catalase, and selenium-dependent GP are some antioxidant enzymes.
Selenium has an important antioxidant element, which is a constituent of selenoenzyme GP and glutathione. Glutathione and GP are both antioxidants that neutralize the free radicals and lipid peroxides to maintain the intracellular homeostasis and redox balance [20]. The association between a lower serum level of selenium and gestational hyperglycemia has been reported previously [21–23]. Asayama et al. [24] reported that selenium-deficient rats had a decreased insulin secretory reserve, when combined with vitamin E, and selenium deficiency resulted in glucose intolerance with a significant correlation between high blood sugar level and depletion of antioxidants. It appears that this depletion is a major risk factor for developing complications, and antioxidant supplements could lower the risk. Dietary intakes and serum level of selenium decreased with a decrease in glucose tolerance. The correlation between selenium and gestational hyperglycemia might be due to the antioxidant and insulin-mimetic function of this element. Selenium has been shown to be involved in maintaining normal glucose uptake, regulating cellular glucose use, and decreasing the severity of insulin resistance and, therefore, has a biological function similar to that of insulin [25]. Women with lower plasma GP activities during pregnancy also tended to have higher fasting glucose levels with inverse relationships between selenium status and glucose tolerance [5].
Selenium must be taken daily in certain amounts in gestational periods. Dietary intakes of selenium is not the only determinant of their serum levels; other factors such as oxidative stress, age, increased elimination rate, chronic illness or inflammation, and drugs might influence their levels [3]. In general, selenium is not taken enough during gestation, which can cause selenium deficiency. Our study showed that the selenium level of gestational diabetes and intolerant pregnancies was lower than that of normal pregnant women. The results were similar to the reports of previous researches [5–8]. The results from both studies demonstrated that selenium is a very important element for glucose intolerants, and its deficiency could aggravate diabetes in the gestational period and increase diabetic complications.
In conclusion, selenium would help to prevent diabetic end-organ damage (blindness, kidney failure, increased risk of heart disease, and painful peripheral nerve damage) when it is given every period of gestation through supplementing with foods, nutrients, and herbs that have antioxidant activity. We believe that selenium has a useful antioxidant effect to prevent GDM and its complications. This study should be supported by research including an explanation of the pathophysiological mechanism of GDM.
References
Kuhl C (1998) Etiology and pathogenesis of gestational diabetes. Diabetes Care 21:19–26
Kamath U, Rao G, Raghothama C, Rai L, Rao P (1998) Erythrocyte indicators of oxidative stress in gestational diabetes. Acta Paediatr 87:676–679
Bo S, Lezo A, Menato G et al (2005) Gestational hyperglycemia, zinc, selenium, and antioxidant vitamins. Nutrition 21:186–191
Holben DH, Smith AM (1999) The diverse role of selenium within selenoproteins: a review. J Am Diet Assoc 99:836–843
Hawkes WC, Alkan Z, Lang K, King JC (2004) Plasma selenium decrease during pregnancy is associated with glucose intolerance. Biol Trace Elem Res 100:19–29
Al-Saleh E, Nandakumaran M, Al-Shammari M, Al-Harouny A (2004) Maternal-fetal status of copper, iron, molybdenum, selenium and zinc in patients with gestational diabetes. J Matern Fetal Neonatal Med 16:15–21
Tan M, Sheng L, Qian Y et al (2001) Changes of serum selenium in pregnant women with gestational diabetes mellitus. Biol Trace Elem Res 83:231–237
Orhan H, Onderoglu L, Yucel A, Sahin G (2003) Circulating biomarkers of oxidative stress in complicated pregnancies. Arch Gynecol Obstet 267:189–195
Quilliot D, Dousset B, Guerci B, Dubois F, Drouin P, Ziegler O (2001) Evidence that diabetes mellitus favors impaired metabolism of zinc, copper, and selenium in chronic pancreatitis. Pancreas 22:299–306
Coustan DR, Carpenter MW (1998) The diagnosis of gestational diabetes. Diabetes Care 21:5–8
Mokdad AH, Ford ES, Bowman BA, Nelson DE, Engelgau MM, Vinicor F, Mark JS (2000) Diabetes trends in the US: 1990–1998. Diabetes Care 23:1278–1283
Kieffer EC, Carman WJ, Gillespie BW, Nolan GH, Worley SE, Guzman JR (2001) Obesity and gestational diabetes among African-American women and Latinas in Detroit: implications for disparities in women’s health. J Am Med Womens Assoc 56:181–187, 196
Ferrara A, Hedderson MM, Quesenberry CP, Selby JV (2002) Prevalence of gestational diabetes mellitus detected by the national diabetes data group or the carpenter and coustan plasma glucose thresholds. Diabetes Care 25:1625–1630
Health Canada (1999) Diabetes in Canada: national statistics and opportunities for improved surveillance, prevention and control. Public Health Agency of Canada, Canada
T.C. Sağlık Bakanlığı, Ana Çocuk Sağlığı ve Aile Planlaması Genel Müdürlüğü (2000) Ulusal Aile Planlaması Hizmet Rehberi. Cilt I, II Ankara
Felber JP, Golay A (2002) Pathways from obesity to diabetes. Int J Obes Metab Disord 26:39–45
Ihara Y, Yamada Y, Toyokuni S et al (2000) Antioxidant alpha-tocopherol ameliorates glycemic control of GK rats, a model of type 2 diabetes. FEBS Lett 473:24–26
Myatt L, Cui X (2004) Oxidative stress in the placenta. Histochem Cell Biol 122:369–382
Fainaru O, Almog B, Pinchuk I, Kupferminc MJ, Lichtenberg D, Many A (2002) Active labour is associated with increased oxidisibility of serum lipids ex vivo. BJOG 109:938–941
Mocatta TJ, Winterbourn CC, Inder TE, Darlow BA (2004) The effect of gestational age and labour on markers of lipid and protein oxidation in cord plasma. Free Radic Res 38:185–191
Wall PD, Pressman EK, Woods JR Jr (2002) Preterm premature rupture of the membranes and antioxidants: the free radical connection. J Perinat Med 30:447–457
Pressman EK, Cavanaugh JL, Mingione M, Norkus EP, Woods JR (2003) Effects of maternal antioxidant supplementation on maternal and fetal antioxidant levels: a randomized, double-blind study. Am J Obstet Gynecol 189:1720–1725
Agarwal A, Gupta S, Sharma RK (2005) Role of oxidative stress in female reproduction. Reprod Biol Endocrinol 14:3–28
Asayama K, Kooy NW, Burr IM (1986) Effect of vitamin E deficiency and selenium deficiency on insulin secretory reserve and free radical scavenging systems in islets: decrease of islet manganosuperoxide dismutase. J Lab Clin Med 107:459–464
Ezaki O (1990) The insulin like effect of selenate in rat adipocytes. J Biol Chem 265:1124–1128
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kilinc, M., Guven, M.A., Ezer, M. et al. Evaluation of Serum Selenium Levels in Turkish Women with Gestational Diabetes Mellitus, Glucose Intolerants, and Normal Controls. Biol Trace Elem Res 123, 35–40 (2008). https://doi.org/10.1007/s12011-007-8087-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-007-8087-2